
Research Article | DOI: https://doi.org/10.31579/2690-8794/200
Department of Stroke Medicine, Fairfield General Hospital, UK.
*Corresponding Author: Marwa Eltemamy, Department of Stroke Medicine, Fairfield General Hospital, UK.
Citation: Marwa Eltemamy, Irrum Aneela, Jacob Mather and Narayanamoorthi Saravanan, (2024), Management of Post Stroke Urinary Retention in the Stroke Unit at Fairfield General Hospital, Bury, UK, Clinical Medical Reviews and Reports, 6(3); DOI:10.31579/2690-8794/200
Copyright: © 2024, Marwa Eltemamy. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 January 2024 | Accepted: 12 February 2024 | Published: 05 March 2024
Keywords: stroke; urinary retention; disease control and prevention; anticholinergics
Background:
Voiding dysfunction after a stroke has a significant impact on the patient’s quality of life and can negatively affect their rehabilitation. During the first 72 hours after the incidence of stroke, 21-47% of patients usually get urine retention². Post-stroke urinary retention can be easily missed especially if associated with overflow.
There is little in the guidelines about the management of urinary retention after stroke. Bladder ultrasound is a well-established non-invasive procedure to diagnose urine retention by measuring post-void residual (PVR) volume⁴. There is no consensus about the optimal time for Trial Without Catheter (TWOC) after stroke.
Objective:
Methods:
We reviewed the medical records of 30 patients from the acute and rehabilitation stroke wards at FGH in January 2022. All the patients were diagnosed with stroke and had documented voiding dysfunction. We counted the days from the stroke incidence to the onset of their voiding problem. We calculated the days of catheterization ended by the review or TWOC. We reviewed the outcome of TWOC in relation to the duration of the catheterization.
Results:
In general, catheter care at our stroke unit conforms to the RCN guidance in regard to the indication of insertion and documentation of that. We lacked good practice in ruling out urinary tract infections by urine testing at the time of catheter insertion. 75% of the patients with urine retention developed this problem during the first week after having a stroke. TWOC was successful during the second week after insertion in 60% of patients while it failed in 80% of patients who had it after 3 weeks of insertion.
Conclusion:
Urine retention usually occurs early after a stroke. We suggest the use of the bladder scan at least once during the first week of admission and consider TWOC during the second week after insertion especially if the cause of retention is treated (infection, constipation, medications)
Voiding dysfunction after a stroke has a significant impact on the patient’s quality of life and can negatively affect their rehabilitation. Around 40-60% of the patients admitted with a stroke develop urinary incontinence which persists in 15% of them at the end of the first year¹. During the first 72 hours after the incidence of stroke, 21-47% of patients usually get urine retention². Post-stroke urinary retention can be easily missed especially if associated with overflow.
The mechanism of urine retention after stroke is multi-factorial. Detrusor areflexia referred to as cerebral shock may occur immediately after stroke leading to urinary retention³. However, detrusor hyperreflexia could be the reason for the retention in presence of either detrusor-sphincter dyssynergia or prostatic hyperplasia. Other possible contributing factors are cognitive impairment, aphasia, diabetes mellitus, and poor functional state.
There is little in the guidelines about the management of urinary retention after stroke. There are still areas that need to be specified when we consider this significant complication of stroke. Bladder ultrasound is a well-established non-invasive procedure to diagnose urine retention by measuring post-void residual (PVR)volume⁴. The use of the portable machine makes it an easy bedside test.
One of the main points that are still questionable is when we should scan the bladder in patients admitted with acute stroke. It is usually done when the patient struggles with voiding or is noticed to have low urine output. Cognitive impairment and/or communication difficulties that occur after a stroke could mask these symptoms.
One of the studies, done in Taiwan⁵, assessed the benefit of portable bladder ultrasound (PBU) in the acute stroke ward. In their results, the incidence of urinary tract infection (UTI) was less after they had started the use of the scanner regularly while the percentage of patients who needed urinary catheters increased.
In their Update to 2009 Comprehensive Nursing Care Scientific Statement, AHA recommended monitoring of PVR with a bladder scan⁶. If the PVR is less than 100 mL for 3 consecutive readings, monitoring can be stopped. When the PVR is more than 100 mL, intermittent catheterisation will be necessary, every 4–6 h ⁷. Most of the patients after stroke have some physical disability that makes self-catheterisation unpractical. The addition of four-times catheterisation to daily nursing care will increase the workload and may not be possible when there is a shortage of staff. In such cases, leaving the catheter in for some time will be a reasonable option.
The second point that we need to consider is the duration of keeping the catheter in place. Apart from AHA guidelines⁸, there was no clear consensus about when we should try without a catheter (TWOC). AHA agrees with the Centres for Disease Control and Prevention (CDC) recommendations about the removal of indwelling urinary catheters within 24 hours for all hospitalized patients to prevent catheter-associated urinary tract infections regardless of the reason for its insertion⁹. Post-stroke urinary retention usually resolves with time and has a favourable prognosis. This means that the catheter is a temporary solution and TWOC should be in mind even if it failed on the first attempt.
In our project, we aimed generally to assess urinary continence care in our stroke units. In particular, we tried to detect the duration between the onset of the voiding dysfunction and stroke incidence to predict when we should use the bladder scan for newly admitted patients. We reviewed the documentation and circumstances of the catheter insertion to compare it with the best practice. We also checked the duration between the insertion and removal of the catheter. We tried to correlate the successful removal with that duration to predict the ideal time for TWOC.
The place of this project is the stroke unit at Fairfield General Hospital in Bury. It is one out of three units that provide acute stroke service in Greater Manchester, UK. It includes an acute ward and two rehabilitation wards.
We reviewed the medical records of 30 patients from the three wards. All the patients were diagnosed with stroke. We chose the patients who had documented voiding dysfunction that started after their admission to the unit.
We collected their demographic data (age and gender), diagnosis (acute ischaemic stroke or haemorrhagic stroke) and whether they were having a pre-existing urinary problem before their admission.
We divided the voiding dysfunction into retention versus incontinence. We counted the days from the stroke incidence to the onset of their voiding problem. We checked if these patients had an immediate clinical examination, bladder scan and urine examination after their symptoms started. For catheterisation, we looked at the following: 1) The reason for the insertion and whether it was documented or not, 2) A recorded plan for TWOC, 3) The number of days since insertion to the time of review and 4) The number of days between the insertion and the first TWOC and whether it was successful or not
Our sample had 16 male and 14 female patients. Only two patients were diagnosed with haemorrhagic stroke while the other 28 patients had an acute ischaemic stroke. 20% [6] of the voiding dysfunction was incontinence and 80% [24] was retention. Two of the incontinent patients had pre-existing incontinence.
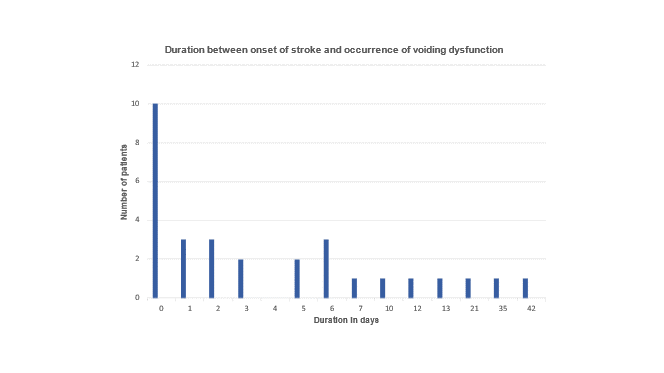
One-third of the patients [10] had the dysfunction at the onset of their stroke including all the incontinent cases. 75% [18] of the urine retention occurred within the first week after the stroke.
All the patients had been examined after the start of their symptoms but only 4 had urine examinations after the insertion of the catheter. All incontinent patients didn’t have a bladder scan while 2 patients with retention had their catheter inserted without a scan.
The reason for the insertion of a catheter was urine retention in all cases. The reason was recorded for all catheters but only 25% [6] patients had a documented plan for removal. At the time of review, the duration that the catheter had been in place ranged between 6 and 90 days. Eleven patients had their catheters for more than 6 weeks.
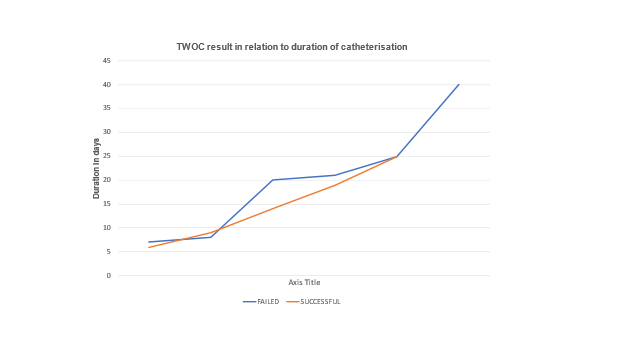
Thirteen patients out of twenty-four didn’t have TWOC. The other eleven patients had their first TWOC after 6-40 days of the insertion. TWOC within the second week for five patients was successful in three of them while it failed in four patients out of five who had it after 3 weeks.

This QIP aimed initially on evaluating bladder care after acute stroke in our hospital. Our current practice for catheterisation was at the core of this project. This may explain the higher number of urine retention compared with incontinence in our cases.
We compared our catheterisation practice with the Catheter Care Guidance of the Royal College of Nursing (RCN)¹⁰. Our practice followed their recommendations regarding the indication and documentation of the reason. All the catheters in this study were inserted to relieve urine retention. All incontinent patients didn’t have a catheter. All the cases had documented reasons for insertion as per the guidance.
Only a few patients had their urine tested for infection at the time of diagnosis of retention. Urinary tract infection is frequently seen with urine retention but its role as a causative factor is not confirmed yet. Sending a urine sample for examination and culture immediately after insertion of the catheter is a good practice which we lacked in our wards.
75% of the patients with urine retention developed this dysfunction during the first week after having a stroke. A bladder scan was done in almost all patients with retention. As it is an easy and reliable bedside test, we recommend its use regularly for new patients during their first week of admission.
TWOC plan was recorded only in one-fourth of the patients which is considered against best care practice. RCN advise having a TWOC plan for short-term catheters, however, it wasn’t mentioned when the removal of the catheter should be tried.
The optimal time of TWOC is yet questionable. Apart from AHA and CDC recommendations for TWOC after 24 hours of catheter insertion, there is no clear guidance. Some authors¹¹ suggested early removal within a few days in cases of acute retention if the reason (constipation, medication or infection) is treated with a success rate of 40%. In our sample, around half of the patients had the catheter for more than 6 weeks. TWOC occurred only in half of the patients at variable timings. It was successful during the second week after insertion in 60% of patients while it failed in 80% of patients who had it after 3 weeks of insertion.
The limitation of this QIP is the small sample size, however, we concluded with the following recommendations:
This QIP needs to be repeated after a few months to evaluate the implications of these recommendations on the improvement of bladder care in our stroke unit.
Voiding dysfunction after acute stroke is a common problem which has a significant impact on the patient's recovery. Routine screening with a bladder scan in the first week of admission may help to diagnose retention early and prevent urinary tract infection. A plan for TWOC should be always in place and reviewed regularly. TWOC shouldn’t be delayed after the treatment of possible causes of retention.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
