
Research Article | DOI: https://doi.org/10.31579/2578-8965/190
1 Women’s Health Clinic.
2 Academia Mexicana de Cirugia y Academia Nacional de Medicina de Mexico.
3 PRONATAL Clinic (Hospital Bité Médica) Mexico.
*Corresponding Author: Vargas Hernández Victor Manuel Ciudad de Mexico, Insurgentes Sur 605-1403, Nápoles, 03810 CDMX,
Citation: Victor Manuel Vargas Hernandez, Jesús e. Lujan irastorza, victor Manuel Vargas Aguilar, (2023), Management of Menopause Towards Natural Management Without Hormones, J. Obstetrics Gynecology and Reproductive Sciences, 7(7) DOI:10.31579/2578-8965/190
Copyright: © 2023, Victor Manuel Vargas Hernandez. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 October 2023 | Accepted: 18 October 2023 | Published: 25 October 2023
Keywords: hormone therapy; menopause; cancer; cryopreservation and ovarian tissue transplantation
Background: Formerly, the life expectancy of women was around the third decade, preserving their ovarian function; With technological development, better socioeconomic and health conditions, they currently live until the ninth decade of life; with a third or more after menopause; with the risk that this entails due to chronic non-communicable diseases associated with hormonal deficiency; It has been suggested that transplantation of cryopreserved ovarian tissue in reproductive life, implanted at menopause, would restore ovarian activity after menopause.
Methodology: To obtain the information, a bibliographic review was carried out in the electronic databases of Google and PubMed-Medline. Articles in English were reviewed between the years 2015 and 2023, with the combination of English terms MeSH: Ovarian tissue cryopreservation and transplantation in menopause.
Results: 59 articles were located, of which 32 were excluded as they were considered not appropriate for the specific topic of the review. 27 articles were selected, including originals, prospective studies and reviews.
Conclusions: Ovarian tissue transplantation could become the anti-aging therapy by restoring long-term ovarian endocrine function; However, more evidence is required to achieve and promote the health of women in menopause.
The development of the ovary from birth to menopause occurs as follows: during fetal life, 100 to 2000 primordial germ cells participate in a massive proliferation process, in the middle of pregnancy; There are several million potential oocytes, 85% are lost before birth and at birth the number of primordial follicles, which do not grow, decreases year after year until puberty, even in the absence of ovarian activity (1). The ovaries of a newborn contain on average 1 million primordial follicles, decreasing to 100,000 at 20 years of age and 65,000 at 25 years of age (95% prediction interval 7700–546,000), the decrease in the number of follicles It continues throughout reproductive life and only 450 of them are used in a lifetime, with around 450 menstrual cycles associated with ovulation, most follicles degenerate and reabsorb during their growth phase (1,2). Cyclic ovulatory folliculogenesis, associated with massive follicular atresia and aging-induced apoptosis, results in ovarian atrophy that decreases fertility in women after 40 years of age, with poor quality oocytes due to genetic alterations in the chromosomes, meiotic spindle, misalignment and shortened
telomeres. Ovarian failure at an early age is a consequence of oncological management with chemotherapy with or without radiotherapy (3), oncological surgery or benign diseases that affect the ovaries such as severe endometriosis or recurrent ovarian cysts that reduce ovarian reserve; Other known risk factors for premature menopause are Turner syndrome, or family history (3,4).
At menopause, follicular density is low and about 1,500 primordial follicles remain, but most are inactive, age has changed very little over centuries, and life expectancy has increased; In the past it was until the third decade and few reached menopause; currently live until the ninth decade, thanks to technological development, better socioeconomic and health conditions and it is estimated that 50% of them will live to be over 100 years of age and extended longevity will increase the high risk of chronic non-communicable diseases related to deficiency. of estrogen (5).
Hormonal Therapy of Menopause
In the 1980s, menopausal hormone therapy (MHT) was considered to prevent osteoporosis, coronary heart disease and dementia, with a significant decrease in mortality. In 1992, the American College of Physicians recommended it to prevent coronary heart disease. In the early 2000s, the Women's Health Initiative (WHI) study suggested more risks than benefits for breast cancer (BC) and reduced its use by 50% (6), 10 years after The WHI and recent studies stratified it and found that with the use of MHT, women aged 50 to 59 years or within 10 years of menopause, decreased coronary heart disease and mortality from all causes, without increased risks, even for CM (5-8); in women 50 to 59 years of age who participated in the WHI with the use of conjugated equine estrogens alone, after 13 years, they had a relative risk for heart disease of 0.65 (0.44 to 0.96), for CM 0.76 (0.52 to 1.11) and for total mortality 0.78 (0.59 to 1.03). MHT reduces the incidence of menopausal symptoms and the risk of osteoporotic fractures, improving quality of life, the risk-benefit balance is positive with the use of MHT, the risks are rare in healthy women of 50-60 years of age, Therefore, it is a suggested window of opportunity and for now its use should be considered as a general prevention strategy for women in the menopausal transition (5-8).
MHT is currently used, but it is difficult to determine the appropriate administration dose and dosing frequency, compared to the naturally produced hormone; There are long-term side effects of oral MHT, such as the increasing incidence of hormone-dependent cancers, stroke, thromboembolism, and heart disease; Cryopreservation of ovarian tissue is an alternative for patients who can postpone menopause, similar to the use of MHT (9,10).
MHT is recommended for the treatment of vasomotor symptoms, genitourinary syndrome of menopause and prevention of osteoporosis, the precise association between MHT and the risks of cardiovascular diseases, venous thromboembolism or neurodegenerative diseases, BC and endometrial cancer It remains controversial to determine how to improve and control the risks of MHT by adjusting its initiation time, regimen, and duration; MHT is not related to the risk of all-cause cardiovascular disease or BC mortality, although it may increase the incidence of some chronic non-communicable diseases; in symptomatic postmenopausal women under 60 years of age without contraindications, early initiation of MHT is safe and shows a long-term mortality benefit; mainly if started during the menopause transition at the lowest effective dose; transdermal or vaginal routes have lower risk, but recent evidence suggests additional clinical benefits with oral MHT to relieve vasomotor symptoms and prevent osteoporosis (11).
Replacement of Thm by Reimplantation of Ovarian Tissue
Cryopreservation of ovarian tissue to restore female reproductive function and recover ovarian endocrine function is under investigation. The first indication for cryopreservation of ovarian tissue is for the cancer patient to restore fertility, and the second indication is hormone replacement for menopausal patients. Ovarian aging is a continuous physiological phenomenon and menopause represents the end of ovarian function. Genetics, measured as family history for age at onset of menopause, is the main determinant. However, physical activity, diet and lifestyle are important factors that influence the age of menopause. Low estrogen levels after natural or premature menopause increase the risk of several diseases, resulting in an increased risk of mortality; Furthermore, the decrease in ovarian reserve is associated with a reduction in fertility (12).
There are limited data on the reimplantation of ovarian tissue for replacement of MHT and these conclude that it is unlikely that heterotopic grafts will have the duration for adequate replacement of MHT in normal menopause; It has been observed that folliculogenesis is evident for 18 months after reimplantation; other studies observed restoration of ovarian activity with resumption of menstruation in 100% of cases when primordial follicles were present in frozen biopsies (2). In other studies ovarian activity did not resume in their tissue grafts and the importance of an intact follicular reserve is highlighted. The long-term duration of ovarian function with ovarian tissue cryopreserved at a mean age of 19 years and reimplantation restored ovarian activity over a period of 6 to 7 years and when the procedure is repeated extends to 12 years. Biopsies should be taken when follicular density is high (between 20 and 25 years of age), where ovarian function is restored for long periods of time. In another report (13) there is ovarian activity for 6-7 years, even with functional ovaries 11 years after the initial procedure. In patients of reproductive age grafted in a heterotopic site and long-term follow-up, the recovery period of ovarian function was short (3-6 months) and was recovered with a second transplant; Likewise, the graft was still functioning after 7 years, considering that, if the objective is to restore ovarian function, not fertility, a heterotopic location could be an easy and effective solution for reimplantation. Heterotopic transplantation preserved the integrity of the ovarian follicle in an animal model, without reporting endocrine secretion. One study reported that heterotopic autografts increase ovarian function in the long term and also after autograft of vitrified ovarian tissue to a heterotopic site (14-15 ).
Removing five to six biopsies 1cm long and 5mm wide will have little or no effect on fertility or age at menopause. Even removal of an entire ovary is not significant; Women with one ovary remain as fertile as women with both; The onset of menopause is minimally affected in women with only one ovary and begins about 1 year earlier; Removal of less than 30% of an ovary has little effect on ovarian reserve and subsequent follicular recruitment (4).
In the long term, endocrine function could persist for more than 7 years (12 years with repetition of the procedure) after freezing-thawing the reimplantation of ovarian tissue (2,13), the restoration of endocrine function prevents conditions related to menopause, such as osteoporosis and others during aging; Reimplantation of ovarian tissue is capable of restoring ovarian activity after induced menopause and in natural menopause, the graft site could be heterotopic, because the objective is not the restoration of fertility and will be initially considered in women with ovarian tissue. already frozen (13) and its application will be the future management of menopause (4).
If the implants stop working, the ovarian tissue transplant is repeated and endocrine function is restored for a longer time; Mainly with new techniques for revascularization, follicle loss rates are reduced and the benefits of the graft could be observed earlier and for longer (16); but, there are still controversies (2,13). Extensive experience in heterotopic grafting has confirmed that progesterone secretion is similar to orthotopic grafting; a progesterone level of 5 mg/ml for 10 days is sufficient to induce differentiation of the endometrium in the secretory phase.
Heterotopic transplantation is not optimal for oocyte quality, but corpora lutea develop in these sites, as well as heterotopic grafts that allow pregnancy and birth. Another drawback of transplantation is whether there is an increased risk of BC or ovarian cancer after tissue reimplantation, taking into account that the well-balanced benefits of MHT have been overestimated; The risk-benefit balance of MHT use in healthy women aged 50 to 59 years or within 10 years of menopause shows lower rates of all-cause mortality, without any increase in MC (5), follow-up of implants placed under the skin is simple, biopsy between 20-25 years of age and risk of developing ovarian cancer in a period of 10 years is low, but increases after natural menopause, when the ovary is over 50 years old, This risk is avoided by isolating the follicles, transferring them into an artificial ovary reimplantation model. The ideal strategy to delay ovarian aging should have the following characteristics (17):
(1) be started in the presence of good ovarian reserve;
(2) be preserved for a long period;
(3) have an action on the dynamics of primordial follicles, controlling the activation rate and atresia; and
(4) safe use in preconception, pregnancy and lactation.
Cryopreservation and transplantation of ovarian tissue is an alternative method that delays menopause with secretion of reproductive hormones. This is achieved by transplanted ovarian tissue that was cryopreserved at a younger age. Cryopreservation and transplantation of ovarian tissue is increasingly used in young cancer patients for restoration of fertility and prevention of premature ovarian failure and has recently been recommended as a method to delay menopause. This is achieved by cryopreserving ovarian tissue that is removed laparoscopically in thin pieces at a young age. The cryopreserved tissue will be transplanted at menopause, when ovarian function is no longer present; Sometimes it will need to be repeated to achieve long-term restoration of ovarian function; It is unknown whether the need to restore ovarian activity appears earlier in women who undergo cryopreservation and ovarian tissue transplantation to delay menopause, indirect data suggest that it is possible (18). The success of cryopreservation and ovarian tissue transplantation could be used to postpone childbearing and/or delay menopause in healthy women without any medical indication for this procedure. At least two-thirds of women who receive autologous cryopreservation of ovarian tissue have menopause reversal and some preliminary experiences indicate a success rate of almost 100% in preventing menopause-related diseases, ovarian transplantation should provide rapid endocrine restoration with a constant hormonal release over time (7,19-22).
Freezing of ovarian tissue and reimplantation can restore ovarian hormonal function for iatrogenic menopause and potentially for natural menopause (2-4,23); In women without a uterus, conventional estrogen MHT should be given, while frozen-thawed ovarian tissue transplantation is beneficial for patients with an intact uterus, since progesterone is not necessary. Studies support ovarian tissue grafting as a way to postpone menopause; with individualization, similar to choose the type of MHT and avoid the effects of menopause, considering family predisposition to osteoporosis, previous hysterectomy, age of menopause and many other factors for its use (13). More research is required, most natural estrogens are produced by the ovary itself (3); Medical and ethical issues must be fully addressed and previously offered as a potential alternative to menopause treatment (24); In the ethical-moral challenge regarding efficacy, the ability to extract ovarian tissue at an early age to maintain its own youth and not adapt to the patient's real age, where the expected ovarian function can be maintained, is questioned. for 6-7 years or more, since the procedure can be easily repeated, to prolong ovarian function for more than 12 years (2,13), investigations must be carried out in accordance with ethical-moral responsibility, to establish whether the Frozen ovarian tissue at a young age followed by reimplantation at menopause could be the anti-aging therapy of the future. The claim that ovarian tissue freezing and reimplantation is a more physiological approach to restoring hormonal function compared to MHT remains controversial. Transplantation will restore ovarian function in most cases; it is unknown if it will maintain hormonal function similar to the reproductive years and for how long. The follicular reserve contained in the graft is small, similar to that which occurs during the transition to menopause (18). Although the role of ovarian tissue cryopreservation as a new anti-aging treatment modality is quite promising, the safety and efficacy of this approach need to be investigated in clinical settings (25-27). Hormone replacement therapy (HRT) administered from the onset of menopausal symptoms usually improves quality and life expectancy; But, it is not without risks; table 1 (17); fertility preservation with cryopreserved ovarian tissue, for the woman who wants to delay her menopause, or wants to take this therapeutic route instead of classic HRT, the risks could outweigh the benefits, since many aspects of the technique have not yet been clarified; With improvements in new techniques serving to accelerate revascularization, rates of follicle loss can be reduced and the benefits of the graft seen earlier and for longer periods. Conventional HRT is currently the most effective route in the treatment of menopause, Long-term use is associated with various side effects, the most important of which is increased risk of breast cancer. With regard to menopause, reestablishing a natural pulsatile hormonal secretion constitutes a substitute for traditional HRT for the treatment of menopausal symptoms.
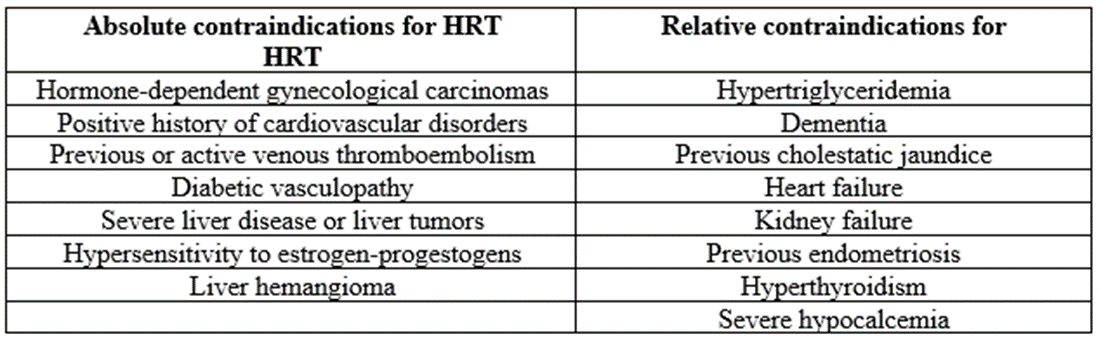
Table: 1 Absolute and Relative Contraindication for Hormonal Replacement Therapy (Hrt).
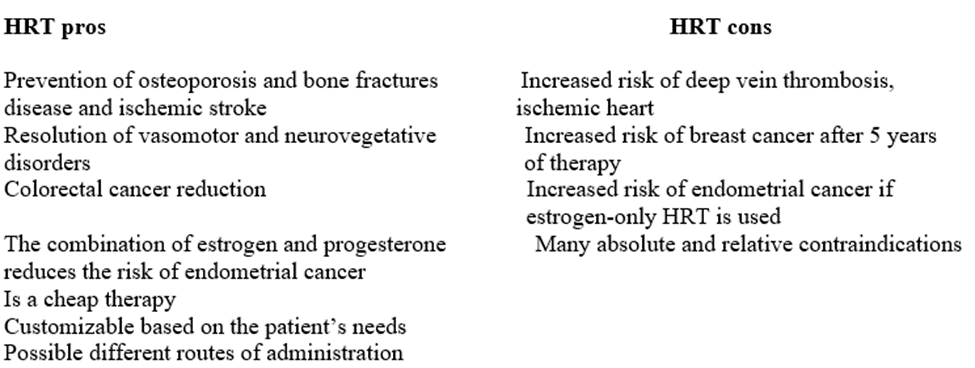
Table: 2 Hormonal Replacement Therapy (Hrt) Pros and Cons.
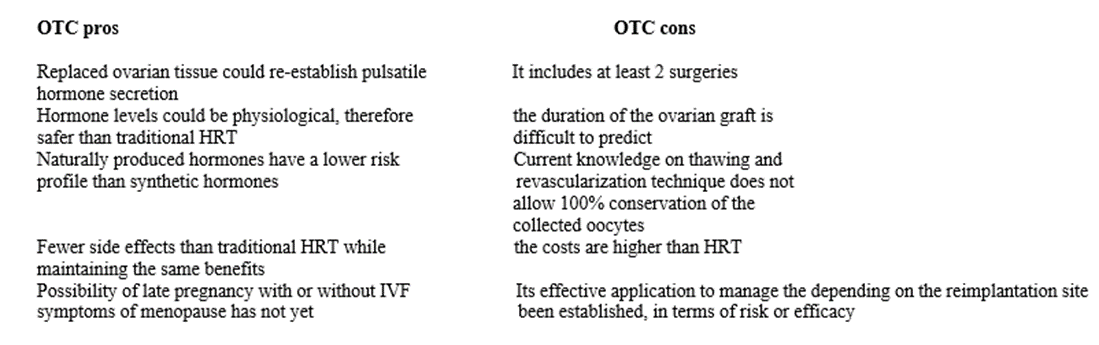
Table: 3 Cryopreservation of Ovarian Tissue (Otc) Pros and Cons.
Ovarian tissue freezing and reimplantation can restore ovarian hormonal function in case of iatrogenic menopause and potentially for natural menopause which could be the anti-aging therapy of the future.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
