
Research Article | DOI: https://doi.org/10.31579/2692-9562/123
1A.T. Still University, Mesa, School of Osteopathic Medicine
2Scripps Memorial Hospital, La Jolla, Department of Electrophysiology
3University of California, San Francisco, Department of Radiology & Biomedical Imaging
*Corresponding Author: Joshua Elmore, A.T. Still University, Mesa, School of Osteopathic Medicine.
Citation: Joshua Elmore, Henry Chen, Gwen Janczyk, Leonard Goldstein, Douglas Gibson, (2024), Management of Induced Brugada Syndrome in Pregnancy: A Case Report, Journal of Clinical Otorhinolaryngology, 6(4); DOI:10.31579/2692-9562/123
Copyright: © 2024, Leonard Goldstein. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 05 May 2024 | Accepted: 24 May 2024 | Published: 04 June 2024
Keywords: stuttering; child; interleukin-10; immune system; pathophysiology
Physiological changes in the cardiovascular system during pregnancy create an impact on the risk and management of women with Brugada Syndrome (BrS). Since the initial diagnosis of BrS in 1992, there have only been a handful of cases regarding BrS during pregnancy. Interestingly, this patient was treated with bupivacaine which was originally believed to be contraindicated indicating the need for additional research involving this medication during pregnancy in BrS patients. The scarcity of data on managing BrS in pregnant individuals accentuates the significance of investigating this topic to optimize maternal and fetal outcomes. We are presenting a 37-year-old antepartum multigravida patient with BrS who was referred to electrophysiology (EP) due to a long history of significant premature ventricular contractions (PVCs) and supraventricular tachycardia (SVT). When gathering information on the patient's family history, we uncovered various cardiac abnormalities among relatives, including right bundle branch block, bradycardia, benign arrhythmias, myocardial infarction (MI), and atrial fibrillation (A-fib). Genetic analysis indicated the inheritance of a genetic variant named SCN5A which is associated with BrS and emphasizes the necessity to conduct genetic analysis on pregnant patients presenting with cardiac anomalies. To minimize symptoms, two cavotricuspid isthmus (CTI) ablations were conducted. Subsequently, a positive EP study demonstrated inducible ventricular fibrillation and a Brugada type III ECG pattern. In conclusion, this case report features the rare and challenging clinical scenario of a pregnant woman diagnosed with BrS after the onset of pregnancy and demonstrates the importance of a multidisciplinary approach involving electrophysiologists, obstetricians, perinatologists, and anesthesiologists. Cardiac monitoring, a careful balance between medication risks and benefits, and individualized care is necessary. Additionally, there is a need for further research to establish evidence-based guidelines for managing BrS during pregnancy. Our goal is to enhance outcomes for both the mother and the fetus in these challenging cases.
Brugada syndrome (BrS) is a rare genetic cardiac rhythm disorder characterized by irregular heartbeats originating from the ventricles, resulting in ventricular arrhythmias, syncope, and potentially sudden death [1,2,3,4]. Since its initial diagnosis in 1992, there have only been a handful of cases regarding BrS during pregnancy emphasizing the need for additional research in this disorder. Pregnancy grants distinctive challenges due to the physiological changes that occur in the cardiovascular system, further impacting the risk and management of arrhythmias in women with BrS. Additionally, this patient was treated with bupivacaine which was originally believed to be contraindicated indicating the need for additional research involving this medication during pregnancy in BrS patients. A comprehensive approach to address concerns during pregnancy and delivery involves heightened surveillance and specialized care from specialized obstetricians, clinical geneticists, cardiologists, pediatric/fetal cardiologists, and anesthetists [5]. The scarcity of data on managing BrS in pregnant individuals accentuates the significance of investigating this topic. In this case report, we present the clinical details and management of a pregnant woman with BrS. We intend to provide support in the understanding of clinical guidelines and therapeutic approaches in such cases is crucial for optimizing maternal and fetal outcomes.
Case Outline
We are presenting a 37-year-old antepartum multigravida patient with BrS who was referred to electrophysiology (EP) due to a long history of significant premature ventricular contractions (PVCs) and supraventricular tachycardia (SVT). When gathering information on the patient's family history, we uncovered various cardiac abnormalities among relatives, including right bundle branch block, bradycardia, benign arrhythmias, myocardial infarction (MI), and atrial fibrillation (A-fib). Genetic analysis indicated the inheritance of a genetic variant associated with BrS and emphasized the necessity to conduct genetic analysis on pregnant patients presenting with cardiac anomalies. The patient's initial cardiac symptoms began at the age of nineteen and she was subsequently diagnosed with SSS (Sick Sinus Syndrome) for which a pacemaker was implanted for bradycardia. Despite pacemaker implantation, the patient's symptoms worsened, and she was admitted for syncope induced by exercise. At the time of syncope, the patient's pacemaker recorded rates as high as 312 beats per minute (BPM). To minimize her symptoms, an EP study and Cavo tricuspid isthmus (CTI) ablation were conducted. Proceeding the operation, the patient’s symptoms greatly improved, however, a few years later her symptoms returned, and she underwent an additional CTI ablation. The patient's first delivery occurred at 41+ weeks in the setting of induction of labor with a prolonged 2nd stage and was unremarkable except for the need for a C-section and one episode of SVT at 17 weeks. However, shortly after delivery, she experienced frequent episodes of short- burst SVT and NSVTs which we believe was due to her recent pregnancy. A few months later, the patient's ECGs showed an abnormal Brugada pattern (see Figure 1) for the first time. This new finding paired with the VUSes in the SCN5A gene (see Table 1) warranted another EP Study which was positive. Another ablation was reasonable at this time due to worsening symptoms which we carried out.

Figure 1: Follow-up Electrocardiogram (ECG) Post-Pregnancy Onset
| Gene | Variant | Zygosity | Variant Classification |
| ANKRD1 | c.347C>T (p. Thr116Met) | heterozygous | Uncertain Significance |
| NEBL | c.1119A>G (Silent) | heterozygous | Uncertain Significance |
| NEBL | c.1837C>T (p. Arg613*) | heterozygous | Uncertain Significance |
| SCN5A | c.3583>T (p. Arg1195Cys) | heterozygous | Uncertain Significance |
| SCN5A | c.2768T>C (p. Met923Thr) | heterozygous | Uncertain Significance |
Table 1: Patient’s Genetic Testing Results from Invintae
In pursuit of expanding their family, the patient opted for a subsequent EP study a few months later. This investigation unequivocally confirmed the existence of BrS. Notably, the study induced Ventricular Tachycardia (VT), necessitating defibrillation intervention. Successively, she received an automatic implantable cardioverter-defibrillator (AICD) to reduce the risk of sudden cardiac death by ventricular fibrillation. At 13 weeks’ gestation of the patient’s second pregnancy, she experienced successive episodes of PVCs with a rate of 197 bpm, with a potential to be hormone related. This subsequently resulted in ventricular tachycardia (VT), necessitating defibrillation to restore normal cardiac rhythm. To manage her condition, a therapeutic regimen of 12.5mg of metoprolol administered twice daily (BID) was initiated and the AICD rate was increased to bypass the PVCs. This course of treatment effectively prevented the recurrence of arrhythmias for approximately five weeks and should be considered in pregnant patients experiencing similar symptoms during pregnancy. Because of an intensification of symptoms during the 18th week of pregnancy, the metoprolol dosage was augmented to 25mg BID, followed by a further escalation to 25mg three times daily (TID) in the 20th week. This elevated dosage regimen was sustained for the duration of the patient's pregnancy. Additionally, as part of the management plan, a prescribed regimen of limited physical activity was implemented to assist in suppressing the occurrence of her arrhythmias. Before delivery, there were extensive discussions with anesthesiology, EP, and perinatology regarding the administration of bupivacaine during spinal anesthesia, as it is considered a medication to avoid in BrS. After considering the risks and the patient’s preference, a successful low-dose spinal block was administered for delivery. This successful medication management outlines the varying cases of Brigada in pregnancy and highlights the need for individualized care and further research. Furthermore, the patient underwent an uncomplicated C-section delivery which highlights the possibility of a C-section requiring considerations regarding the temporary deactivation of the AICD during the procedure. The patient observed that her symptoms improved after ablation procedures but worsened with both pregnancies late in the first trimester and early second trimester putting additional strain on her heart. When gathering information on the patient's family history, we uncovered various cardiac abnormalities among relatives, including right bundle branch block, bradycardia, benign arrhythmias, myocardial infarction (MI), and atrial fibrillation (A-fib). Genetic analysis indicated the inheritance of a genetic variant associated with BrS.
This case report explores a rare and challenging clinical scenario, detailing the management of BrS in a pregnant woman and contributing valuable insights to the literature on this rare genetic cardiac rhythm disorder during pregnancy. This report involves a single patient, and as such, the findings and management strategies may not be universally applicable to all individuals with BrS during pregnancy. There is a recognized correlation with a higher occurrence of arrhythmias which may be exacerbated during pregnancy. Specifically, milder forms of arrhythmias, such as premature atrial and ventricular contractions, tend to exhibit a greater frequency during pregnancy compared to the period before conception [6,7]. The proarrhythmic mechanisms of pregnancy are believed to be associated with various changes in the cardiovascular system, autonomic function, and hormonal levels but more research is required to determine the onset of our patient's BrS. Factors such as elevated plasma catecholamine levels, the chronotropic effects of relaxin, the mechanical impact of atrial stretching, increased ventricular end-diastolic volume resulting from the expanded intravascular volume, as well as hormonal and emotional fluctuations collectively contribute to the development of arrhythmia [6,7]. While cardiac modifications are seen throughout pregnancy, the majority of women maintain values within the range of normal physiological levels [8]. Nonetheless, in individuals with an inherent predisposition to repolarization abnormalities, pregnancy can pose a vulnerable phase, increasing the risk of cardiac arrhythmias which was seen in our case.A retrospective cohort study conducted in 2021 emphasized women with BrS revealed no increased risk of serious cardiac events during pregnancy, although the spontaneous abortion rate might be increased [9]. Table 2 outlines the results of available literature regarding pregnant women with BrS.
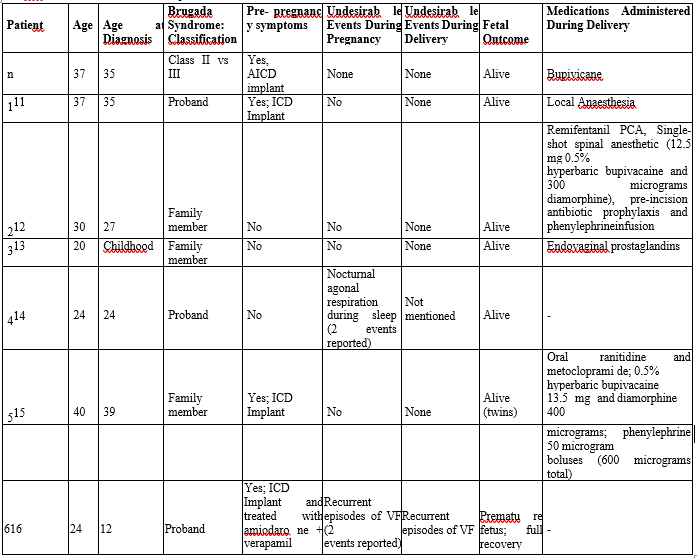
Table 2: Brugada Study Data [3,10,11,13,14]
In conclusion, this case report features the rare and challenging clinical scenario of a pregnant woman diagnosed with BrS after the onset of pregnancy. The physiological changes during pregnancy, including hormonal fluctuations and increased cardiac output, can influence the electrical stability of the heart, and potentially exacerbate arrhythmias. Balancing the risks associated with medications, the management of arrhythmias, and the well-being of both the mother and fetus is of the utmost importance. This novel case demonstrates the importance of a multidisciplinary approach involving electrophysiologists, obstetricians, perinatologists, and anesthesiologists to optimize the care of pregnant women with BrS. The initial diagnosis of BrS was made based on the characteristic ECG findings and supported by genetic testing. Careful monitoring of the patient’s cardiac status was critical throughout her pregnancy to precipitously detect any changes or arrhythmias. It is important to recognize the limited data and guidelines available for managing pregnant women with BrS. By sharing our experiences and insights, we hope to contribute to the growing body of knowledge and improve the understanding and management of pregnancy induced BrS.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
