
Case Report | DOI: https://doi.org/10.31579/2768-2757/022
*Corresponding Author: Luis Argote-Greene, Department of Thoracic Surgery, University Hospitals Cleveland Medical Center, Cleveland, USA.
Citation: R Gardner, A Tipton, M Janko, P Linden, Luis A Greene, et al. (2021) Management of Bilateral Spontaneous Pneumothorax Related to COVID-19 Infection. Journal of Clinical Surgery and Research. 2(3) DOI: 10.31579/2768-2757/022
Copyright: ©2021 Luis Argote-Greene, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 July 2021 | Accepted: 26 July 2021 | Published: 29 July 2021
Keywords: covid pneumothorax; spontaneous pneumothorax; bilateral pneumothorax; covid pneumonia
Spontaneous pneumothorax is a rare but potentially fatal complication of coronavirus infection and COVID-19 pneumonia. Data is limited to guide clinicians in the setting of spontaneous pneumothorax when conservative management fails and operative intervention is required. We report the clinical course and operative strategy for a patient who presented with sequential bilateral spontaneous pneumothorax after being diagnosed with severe COVID-19 pneumonia. Conservative management with bilateral tube thoracostomies failed to resolve persistent alveolar-pleural fistulae, and ultimately the patient recovered after synchronous bilateral VATS blebectomies in the operating room. The timing and treatment of spontaneous pneumothorax requires follow-up education and surveillance for patients with this disease, as lack of prompt treatment outside the hospital could increase patient mortality. Spontaneous pneumothorax is a concern in patients who re-present with recurrent symptoms after COVID-19 diagnosis. When conservative treatment fails, surgery can safely be performed in COVID-19 patients with simultaneous bilateral pneumothorax with full functional recovery.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes a systemic infection (COVID-19) that is associated with barotrauma in 15% of ventilated patients including both pneumothorax (PTX) and pneumomediastinum [1]. Limited data is available for management of COVID-19 patients with spontaneous pneumothorax (SPTX) [2]. Medical management alone may be related to prolonged hospitalization, intubation, and additional complications [3, 4]. Here, we present a COVID-19 patient with bilateral SPTX treated successfully with thoracoscopy and bleb resection.
A 62-year-old male non-smoker with chronic untreated hepatitis C was diagnosed with COVID-19 by nasal swab in May 2020. He presented with fever, tachycardia, and hypoxia requiring supplemental oxygen by nasal cannula. He was treated with Remdesivir 200 milligrams (mg) intravenously (IV) followed by 100 mg IV daily for five days. No PTX was seen on computed tomography (CT). He was discharged after seven days.
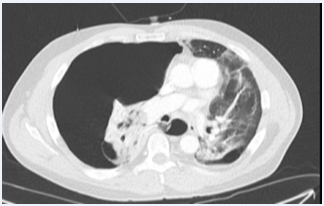
He re-presented 17 days later with shortness of breath, chest pain, tachypnea, hypoxia, and mild leukocytosis. Repeat COVID-19 nasal swab was negative. An echocardiogram demonstrated right heart strain. CT demonstrated a right tension PTX without evidence of pulmonary embolism (Figure 1). A right pleural thoracostomy tube facilitated re-expansion of the right lung. Intravenous cefepime was initiated for possible hospital-acquired pneumonia. Nasal cannula oxygen was supplemented. On hospital day two, a new left pneumothorax was discovered and a left pleural thoracostomy tube was placed, resolving the pneumothorax. Water-seal trials showed persistent alveolar-pleural leaks, likely secondary to ruptured blebs from cystic lung changes.
After 12 days of failing to progress with persistent air leaks and pleural effusions, the patient underwent video-assisted thoracoscopic surgery (VATS), left lower and upper lobe blebectomies, and a right upper lobe wedge resection. The previously-placed small diameter right thoracostomy tube was exchanged and connected to suction with the patient on double-lung ventilation in the supine position. The left lung was then isolated in the right lateral decubitus position, and a left 6th intercostal space mini-thoracotomy was performed. Copious sero-sanguineous pleural fluid was drained. A thickened visceral pleura contained such a sizable sub-pleural accumulation of sanguineous fluid that the parenchyma floated inside the sac. The visceral pleural sac and affected lung were removed with Endo-GIA purple load staplers (Covidien, Dublin, Ireland). Similar, but less dramatic, findings were seen on the contralateral lung. Bilateral chest-tubes remained in place after the operation.
The postoperative course was uncomplicated. No further alveolar-pleural leaks were detected. Chest tubes were removed three days later. The patient was discharged home on postoperative day seven without supplemental oxygen. Histological examination of the operative specimens demonstrated pulmonary blebs with organizing pleuritis, subpleural hemorrhages, and fibrosis. Two months later, he had recovered well with improved exercise tolerance. Follow-up CT demonstrated postsurgical changes and non-specific interstitial opacities (Figure 2).

Approximately 1% of patients with COVID-19 develop SPTX [5]. Bellini reported the first two cases of COVID-19 patients with SPTXs treated surgically [3]. Like our patient, both patients were readmitted weeks after initial hospitalization. The authors concluded that blebectomy and wedge resection were safe and efficacious alternatives to conservative management. Aiolfi also reported two COVID-19 patients with unilateral SPTXs who were successfully treated with thoracoscopy and bleb resection [4]. While ideal timing of thoracoscopy in COVID-19 patients with persistent pneumothorax remains unclear, operative intervention under one week from chest tube drainage led to air leak control, contributing to a faster recovery.
The thickened, stiff parenchyma found in COVID-19 lungs prevents proper function, requires prolonged mechanical ventilation, and predisposes to complications such as interstitial pneumonia, acute respiratory distress syndrome, and PTX [1, 4]. The authors suggest that COVID-19 patients be informed of their risk for subsequent complications, such as SPTX, after resolution of their acute symptoms, and seek medical attention if they experience chest pain or shortness of breath in the weeks following their diagnosis.
SPTX may occur weeks after a COVID-19 diagnosis. When conservative treatment fails, surgery may safely be performed in COVID-19 patients with simultaneous bilateral SPTX.
No conflicts of interest.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
