
Research Article | DOI: https://doi.org/10.31579/2693-4779/168
Family Physician & Public Health Consultant Bengaluru.
*Corresponding Author: Suresh Kishanrao, MD, DIH, DF, FIAP, FIPHA, FISCD, Family Physician & Public Health Consultant Bengaluru.
Citation: : Suresh Kishanrao, (2024), Management of Asthma & Its Exacerbations in smaller settings, Clinical Research and Clinical Trials, 9(1); DOI:10.31579/2693-4779/168
Copyright: © 2024, Suresh Kishanrao. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 November 2023 | Accepted: 01 December 2023 | Published: 03 January 2024
Keywords: asthma; severe (exacerbated)asthma; non-eosinophilic asthma; asthma phenotype; asthma endotype; neutrophilic asthma; biological; monoclonal antibodies; patient perspectives of asthma; the global initiative for asthma (gina)
Asthma is a common heterogeneous lung disease that affects people of all ages, characterized by chronic airway inflammation, diagnosed mostly by the history of shortness of breath, wheeze, cough, and chest tightness that vary over time and in intensity, with variable expiratory airflow limitation. When symptoms make breathing hard, due to a trigger or severe inflammation it is known as Asthma exacerbation or attack. A trigger is defined as an exposure which elicits an exacerbation in a stable or previously asymptomatic patient of asthma. Although food and environmental allergens are common triggers for asthma, but for asthma attacks allergens or air pollutants are responsible and not food.
Asthma affects more than 300 million people worldwide; it is responsible for over 1000 deaths a day. India contributes to about 39 million (13%) cases and 450 (42%) of global deaths. While deaths due to asthma in most developed countries have declined steadily, in India it has increased by 33% over last 3 decades indicating timely accessibility and poor management of acute attacks. Bengaluru city is considered as asthma capital of India due to sheer numbers it reports every year. Disparity between the perception of an Indian patient and the objective criteria in asthma control also contribute.
Two main categories of severe asthma are identified in India based on a person's response to treatment i) Type-2 inflammation e.g., Allergic asthma and eosinophilic asthma and ii) non-type-2 inflammation e.g., non-eosinophilic asthma (NEA). NEA is characterized by airway inflammation with the absence of eosinophils, after activation of non-predominant type 2 immunologic pathways, defined by an eosinophil count <2% in sputum and poor response to known therapeutic options.
The differential diagnosis in Filaria endemic districts globally and in India need to include Tropical Pulmonary Eosinophilia (TPE), a hyperresponsive pulmonary syndrome to trapped microfilariae of lymphatic filariasis caused by filarial nematode Wuchereria bancrofti within the lung tissue.
The general approach to treatment of an acute asthma exacerbation includes administration of inhaled bronchodilators (beta-agonist therapy -e.g., Albuterol), as well as systemic glucocorticoids in most patients. Asthma medications in inhaled form is considered better as compared to systemic formulations (oral/IV) to improve clinical outcomes, as Inhaled medicines work faster to improve the symptoms and outcomes and are safer as compared to oral or IV route. Initial treatment of acute asthma exacerbations can be provided in the primary care setting or even at home. However, children with moderate-to-severe exacerbations need to be managed in an inpatient setting as they require close observation for clinical deterioration, frequent treatments, and repeated evaluation.
Materials and Methods: This review is based on personal experience of managing three anecdotes of three varieties of Asthma cases in adults, over last 5 decades, literature review and latest national guidelines and GINA recommendation of Asthma management.
Asthma is a common lung disease that affects people of all ages, but often starts during childhood. It is a heterogeneous disease, characterized by chronic airway inflammation. It is defined and clinically diagnosed mostly by the history of respiratory symptoms of shortness of breath, wheeze, cough, and chest tightness that vary over time and in intensity, with variable expiratory airflow limitation. This is long-haul condition affecting the ability to breathe due to inflammation & narrowed airways in lungs. When severe inflammation occurs and asthma symptoms make breathing hard, it is known an asthma exacerbation or asthma attack. Asthma affects more than 300 million people worldwide, is the most common chronic condition in childhood, and is responsible for over 1000 deaths a day, the majority of which are preventable. India contributes to about 39 million cases. [1] While deaths due to asthma in most developed countries have declined steadily, in India it increased by 33% over last 3 decades. India now contributes to an alarming 42.4% of all global asthma deaths, despite accounting for only 13% of the global asthma cases indicting management lacunae. Bengaluru, this author’s home city is considered as asthma capital of India due to sheer numbers reported every year [2].
Disparity exists between the perception of an Indian patient with asthma and the objective criteria in asthma control. Asthma is basically a clinical diagnosis in adults, General Practitioners (GPs) or Family Physicians (FPs), use peak expiratory flow (PEF) as a good indicator for asthma diagnosis & prognosis if it shows reversibility on bronchodilator medication. Asthma diagnosis in young children is mainly based on recurrent symptom patterns plus assessment of family history plus physical findings plus differential diagnostic possibilities. Clinicians recognise 4 types of Asthma i) mild intermittent asthma with symptoms fewer than two times a week, ii) mild persistent asthma with symptoms more than two times a week, but no more than once a day, iii) moderate persistent asthma with Symptoms every day, iv) Severe persistent asthma with constant symptoms [3].
A trigger is defined as a factor or an exposure which elicits an exacerbation in a stable or previously asymptomatic patient of asthma. Although food and environmental allergens are common triggers for asthma, but for asthma attacks allergens or air pollutants are responsible and not food [3].
Two main categories of severe asthma are identified in India based on a person's response to treatment i) Type-2 inflammation e.g., Allergic asthma and eosinophilic asthma and ii) non-type-2 inflammation e.g., non-eosinophilic asthma (NEA). NEA is characterized by airway inflammation with the absence of eosinophils, after activation of non-predominant type 2 immunologic pathways, defined by an eosinophil count <2>
The differential diagnosis in Filaria endemic districts in India include Tropical Pulmonary Eosinophilia (TPE), a hyperresponsive pulmonary syndrome in response to trapped microfilariae of lymphatic filariasis within the lung tissue. TPE is caused by filarial nematodes most common in Karnataka & India being Wuchereria bancrofti. The other two nematodes are Brugia Malayi, & B. Timori [4-5].
This article is the result of managing an atypical case of Asthma in a young lady of 23 years in September 2023, A case of Non-Eosinophilic Asthma in December 2021 and comparing with a similar symptomatic case of Tropical pulmonary eosinophilia (1973) 50 years ago, in one of Lymphatic Filaria endemic district in Karnataka.
1. Soumya- First attack of Atypical Asthma:
On 18 September 2023, Soumya a 23-year-old girl student of architecture, in an institute in Yelahanka, Bengaluru reports to a local private clinic with the complaints of cough and vomiting since last 24 hours. she also complaint of chest and abdominal pain. On examination her RR= 30, BP-120/80, Respiratory rate 32/minute and SpO2-92%. Without any provisional diagnosis or investigations symptomatic treatment she was prescribed i) Tablet Pan (an acid-reducing medicine, used to treat stomach ulcers, gastroesophageal reflux disease (GERD) and other acidity-related problems). GERD occurs due to frequent acid reflux (burning pain or discomfort in the chest)40mg twice a day, ii) Tab Deriphyllin Retard 150 mg, BD for 5 days {(a combination medicine used to prevent and treat wheezing, shortness of breath, chest tightness associated with lung diseases like asthma, chronic bronchitis, emphysema, chronic obstructive pulmonary disorder (COPD)}, iii) Tab Levoday (an antibiotic containing Levofloxacin) 500 mg once day iv) Tab Allut Dl (Norethisterone used in heavy menstrual bleeding, dysmenorrhea, endometriosis & Premenstrual syndrome etc) ,v) Ascoril D syrup (contains chlorpheniramine and phenylephrine- anti-histamine or allergy drug for relief of the common cold and nasal congestion) 10 ml twice a day.
Since there was no relief from any of the symptoms and breathing became difficult, she went back in the evening to the same doctor, who now gave Inj. Hydrocortisone 100mg IM with Formoterol + Budesonide tablets twice a day. As she was in Paying Guest house, her father (my nephew) called me to help. I asked the girl to come home, that she did around 1930 hrs. Her amin complaint was Chest pain under sternum, cough but sputum not coming out easily and no fever. Family history of Asthma was elicited by talking to her father over phone (her grandfather did have Asthma and was using Nebulizer). On examination Her RR was 28/minute, BP =118/78, SpO2-95%, No Rhonchi. I made a provisional diagnosis of Asthma exacerbation and responding to the cortisone injection given in the evening. I asked her to continue same drugs but added Rico-fast Plus {Paracetamol (500mg) + Pseudoephedrine (60mg) + Triprolidine (2.5mg) provides relief from symptoms such as headache, sore throat, runny nose, muscular pain, and fever} and Ibuprofen 400mg (anti-inflammatory) asked her to inhale steam for 10 minutes before retiring for the day. As an emergency requirement I bought Deriphyllin injection and simple Nebulizer, if need be, to use in the night. He could have sound sleep over night and next day 919th September) morning she was feeling better though the chest pain had reduced but still nagging. By end of 19 September, she was more comfortable and by morning of 20th her chest pain had vanished. I reduced the drugs over next 2 days and girl was normal by 21 September 2023. Currently she gets a few attacks (once to twice a week for 1-2 hours) of breathlessness for short while, may need to asked to use Nebulizer in case of exacerbration.
2.A case of Non-Eosinophilic Asthma (December 2021):
A 36-year-old Obese female patient came to the tertiary care hospital with complaints of progressively worsening dyspnoea, persistent dry cough at night, wheezing, along with symptoms of occasional runny nose and sneezing. She had a 4-year history of asthma and had reported 8 exacerbation episodes in first 11 months of 2021, out of which two episodes required intensive care unit (ICU) admission. The current exacerbation was following an overtime work in her occupation exposed to some fumes and increased smoking due to work pressure. On admission she reported being on Inhaled corticosteroids (ICSs) plus LABA, long-acting muscarinic antagonist (LAMA), LTRA, thromboxane A2 antagonist, and oral prednisolone (30 mg/day). When presented she was an obese lady of 5.2 ft height and weighing 90Kgs. The pulse rate was 132/minute, Respiratory rate 46/min and SpO2 -86%. Her Blood eosinophilic count was 1.6% and her pulmonary function tests revealed FEV1 30% of predicted value and FEV1/forced vital capacity (FVC) ratio was 55%, and fractional exhaled nitric oxide (FeNO) levels of 60 ppb. As in the previous episode managed in ICU the drugs prescribed did not benefit her. Her ACT score was 12, Global Initiative for Asthma (GINA) asthma severity score was 4, Asthma Control Questionnaire score was 5.3, and Asthma Quality of Life Questionnaire score was 1.28. She also reported frequent attacks of GERD, anxiety, or depression since October 2022. Her serum total IgE levels (200 IU/mL,)
As developing strategies to regulate neutrophil function to modulate non-eosinophilic inflammation is the approach, she was put on AZD5069, a selective small-molecule antagonist of the human CXCR2 chemokine receptors, with greater than 100-fold selectivity. In addition, she was advised to change her job of exposure to occupational pollutants and smoking cessation may reduce neutrophilic inflammation in asthma. After cessation of exposure to occupational agents, neutrophilic inflammation was reduced, and she showed improvement over next 3 days and almost normal by the weekend. She ahs moved to some executive work to minimize the exposure.
3.Kashappa, a case of Tropical Pulmonary Eosinophilia (TPE) 1973:
It was winter 1973, nearly 50 years ago, I was my fifth year of service, working as a medical officer in one of the Primary Health Centre (PHC) in Kalburgi a known Filaria endemic district. A 36-year-old male patient presented with complaints of dry cough and shortness of breath on exertion for two months. His cough was worse at night. He also complained of low-grade intermittent fever for two months. His appetite was normal, and he denied any history of weight loss, joint pain, night sweats, chills, rash, rhinorrhoea, epistaxis, haemoptysis, haematuria or burning sensation in hands and feet. There was no history of smoking or any kind of drug intake. His past medical history was unremarkable. He was a resident of a village in Mangalore District Western part of Karnataka and worked as a manager on a poultry farm in this district, both known endemic district for Filarial Elephantiasis limbs & Hydrocele.
Two weeks before presenting to our medical care facility, he was diagnosed with a lower respiratory tract infection by a private practitioner and was prescribed a short course of oral antibiotics. But he continued to have fever, cough, and breathlessness. On presentation to our facility, his physical examination was notable for rhonchi throughout both lung fields. His vital signs were normal. The results of initial laboratory investigations available at PHC level were as follows: haemoglobin 12.8 gm/dL (reference range: 13-17 gm/dL), total leukocyte count 50,230/µL (reference range: 4,000-11,000/µL), absolute eosinophil count 37,510/µL (reference range: 40-440/µL, over 500 eosinophils per microliter of blood is thought to be eosinophilia in adults), and random blood sugar 93 mg/dL (reference range: 70-100 mg/dL). Peripheral blood smear showed leucocytosis with marked eosinophilia without any left shift. The chest radiograph showed the presence of reticulonodular opacities involving all zones of both lung fields.
Being in endemic district and having seen many filarial hydroceles in vasectomy camps, I decided to treat both for Asthma and TPE. Having given IV Aminophylline, on day one, I put him on Tab Deriphyllin thrice a day and tab. Banocide Forte (Diethylcarbamazine-100MG) three times a day alerting him that he must take the tablets for full 3 weeks and even threatening him to say “if you default you will end up in Tuberculosis and might have to be treated for 12-18months’.
To my utter surprise and his happiness, he started showing improvement from day 4, had negligible cough by 10th day, and completely relieved of all symptoms and Eosinophil count falling to normal level when tested after 3 weeks. It was a sort of miracle in highly TB endemic district.
Asthma has been known as common heterogeneous lung disease that affects people of all ages, characterized by chronic airway inflammation, diagnosed mostly by the history with variable expiratory airflow limitation and sometimes known as Exacerbation or Asthma attack if symptoms make breathing hard, due to a trigger or severe inflammation. A trigger is defined as an exposure that elicits an exacerbation in a stable or previously asymptomatic patient of asthma. Although food and environmental allergens are common triggers for asthma, but for asthma attacks allergens it is air pollutants and not food that are responsible. The challenge in management is mainly due to disparity that exists between the perception of the patients and the objective criteria in asthma control Globally. To address this disparity The Global Initiative for Asthma (GINA) was launched in 1993 under the auspices of the National Heart, Lung, and Blood Institute, National Institutes of Health, USA, and the World Health Organization. GINA works with health care professionals and public health officials around the globe to reduce asthma prevalence, morbidity, and mortality [1].
GINA 2023 defined Asthma by the history of respiratory symptoms of shortness of breath, wheeze, cough, and chest tightness that vary over time and in intensity, together with variable expiratory airflow limitation. While it affects 1-29% of the population in different countries.
In 2019, a total of 262.41 million prevalent cases were estimated, with an age-standardized prevalence of 3415.53 per 100,000, a decrease of 24.05% since 1990. The Global Burden of Disease (1990–2019) estimated the total burden of asthma in India as 34.3 million, accounting for 13.09% of the global burden [3]. The prevalence of current wheeze in the 6–7 years, 13–14 years and adults was 3.16%, 3.63% and 3.30%, respectively. The GINA Indian Study estimated the national burden of asthma at 17.23 million with an overall prevalence of 2.05%. The trends in India indicated that asthma prevalence among children increased from 8.7% in 2001 to 9.5% in 2011 and then decreased significantly to 6.5% in 2019, whereas in adults it increased from 6.9% in 2001 to 8.0% in 2021 [3]. There was a significant reduction in current wheeze in GAN Phase I compared with the previous ISAAC Phase III study [1] It also estimated that 13.2 per thousand deaths due to asthma. Symptoms and airflow limitation are influenced by exercise, allergens, or irritants, change in weather or Viral respiratory infections, and sometimes resolve spontaneously or in response to medication. Most patients end up in periodical exacerbations carrying significant burden to the patient’s, their families, and the Governments in low- and Middle-income countries like India [1].
Symptoms of an Asthma Exacerbation
Asthma symptoms can vary based on the season or from year to year. Asthma Attack or an exacerbated Asthma symptoms are similar, except that they are worse during an exacerbation. In mild/moderate cases, symptoms might last just a few minutes, but they usually linger for several hours or even days. If an individual is experiencing Shortness of Breath, Coughing, Wheezing, Chest tightness and vomiting coupled with the signs of Low Peak Expiratory Flow readings, or more frequently, S/he needs use rescue inhaler more often, points to worsening asthma.
The latest understanding of common signs and symptoms are listed below, but neither there is a need to have each one of them nor for them to occur in the order indicated [1].
1. Shortness of Breath: Common experience shortness of breath, as though S/he is suffocating or can’t catch breath, either S/he can’t take deep breaths or breathlessness occurs during rest or physical activity. One can see, the skin on the neck & chest begins to suck inward as patient breaths.
2. Coughing: The person may have a tight, dry cough that won’t stop, making it harder for him/her to catch breath. These coughs are typically nonproductive, don’t help clear the throat or any mucus in lungs. It’s more common for coughing early in the morning or at night, waking from a sound sleep.
3. Wheezing: Wheezing is a purring or whistling sound, usually audible when a patient breathes out. It may start like a low-pitched whistle and get higher pitched as patient breathes. Patient may report of feeling a rattling sensation in the chest.
4. Chest Tightness: The person may feel a tight, squeezing pressure as if someone is sitting on the chest or the air is being sucked out, and patient may feel lightheaded.
5.Chest Pain: Chest pain usually attributed to heart conditions can be a symptom of asthma attacks. Asthma-related chest pain is often felt in the sternum. Patients describe chest pain as dull and aching or sharp & stabbing as was in our Soumya’s case. In some patients the dull chest pain became sharp or stabbing when they coughed or breathed in deeply, and subsiding when the attack is resolved.
6.Troubled Breathing: Difficult breathing in asthma does not always appear as the classic symptoms. but is characterised by i) Rapid breathing, ii) High-pitched sound when inhaling, iii) Taking a long time to exhale iv) Sniffing the air v) Intercostal retractions muscles are important for breathing, when they pull inward, if the trachea or bronchi are blocked. Intercostal retractions indicate breathing difficulty present in moderate and severe asthma attacks.
7. Low Peak Expiratory Flow (PEF) Readings: A peak flow meter (PFM) measures the amount of air we breathe out. During an asthma attack, airways narrow and block airflow, dropping our PEF readings. A reading between 50 and 80% is the time to use rescue medication. If your PEF reading falls below 50% seek emergency care immediately.
Non-respiratory symptoms Asthma:
8. Troubled Sleeping: People with asthma may have trouble sleeping due to shortness of breath, wheezing, or nighttime coughing. Some asthmatics develop obstructive sleep apnoea (OSA), leading to interrupted sleep, fatigue, & daytime sleepiness. Patients OSA find it difficult to control asthma.
9.Fatigue: Feeling tired or sleepy can be signs of an oncoming asthma attack or occur during an attack and Fatigue has a negative effect on quality of life.
Sweating: Sweating can be an indication of an oncoming asthma attack and can occur during severe asthma attacks. Nearly one thirds of the patient’s report sweating before their asthma attack, and two thirds report sweating during the attack.
Tachycardia: A rapid pulse can be a symptom of a severe asthma attack. A pulse of 140 or more per minute in children aged 2 to 5, 125 or more per minute in children older than 5, a pulse of 120 or more per minute in adults respectively indicates a severe exacerbation or a severe asthma attack.
Cardiac Problems: There is emerging evidence that persistent asthma is associated with tachycardia and atrial fibrillation due to Beta-agonist, used to treat Asthma. A 2020 study of 6,615 adults with asthma has reported that those with persistent asthma were at greater risk of atrial fibrillation.
Mood Disorders: Mood disorders like anxiety and depression are common in people with asthma. Anxiety and depression can impact a person’s asthma management. Patients with an anxiety, or a depression, or both have a higher rate of asthma-related emergency room visits than those without a mental health disturbance.
Anxiety: Anxiety can trigger asthma, and, at the same time, poorly controlled asthma is associated with anxiety symptoms. Feeling a lack of control over your asthma can promote feelings of stress. Sometimes it is challenging to differentiate between the physical manifestations like a tight feeling in the chest or shallow breathing can mimic asthma and can even exacerbate asthma symptoms. Panic attacks can also be difficult to distinguish from asthma attacks, as in both cases, one may feel short of breath or be unable to speak.
Depression: Depression is common in people with chronic health conditions, due to long term treatment or limitations related to the condition. One study of adults has reported Asthmatics twice as depressed than the general population.
Treatments for an Asthma Exacerbation
Of the medications used to treat asthma attacks some help reduce swelling, while others open the airways so that patient can breathe better. These medicines are better administered with an inhaler, or Nebulizers sometimes paired with a spacer. There are four types of asthma inhaler devices that deliver medicine: metered dose inhalers (MDI), dry powder inhalers (DPI), breath actuated inhalers, and soft mist inhalers. These equipment’s may have more than one medication to help manage symptoms. The asthmatic individuals need to carry these quick-relief medications always to start the treatment in case of a sudden asthma attack. Some people may need to be training. A PHC doctor will check your lung function through a series of tests, including spirometry and prepare an Asthma plan. Individual specific Asthma plan must address [1,6,7,8,9,10]:
The commonly used medications are:
1. Short-Acting Beta-2 Agonists (SABAs): help open the airways in the lungs so that air can flow more easily, making it easier to breathe. These are prescribed as rescue inhalers or for use in a nebulizer, which creates a medicated mist to inhale. The two most used SABAs for an asthma attack are Albuterol sulphate (Accuneb, ProAir Digihaler, ProAir HFA, Proair Respiclick, Proventil, Proventil HFA, ReliOn Ventolin HFA, and Ventolin) and levalbuterol tartrate (Xopenex HFA).
2. Corticosteroids: Corticosteroids (steroids) are given in the emergency room to reduce airway inflammation during an asthma attack. They are given as oral tablets, or inhalers or in severe cases, as an intravenous injection to alleviate an attack- i) Oral corticosteroids are used for short-term treatment as they cause side effects, like osteoporosis and weight gain- e.g., Prednisolone ii) Inhaled corticosteroids are typically used as maintenance therapies to prevent asthma exacerbations.
Recent evidence is in favour of combining an inhaled corticosteroid, such as budesonide, with albuterol in a rescue inhaler to treat asthma attacks and improve lung function.
3. Short-Acting Muscarinic Antagonists (SAMAs): These are occasionally used to treat asthma attacks when albuterol isn’t completely effective, as they also open airways to help breathe easier. The most used SAMA is ipratropium bromide (Atrovent).
4. Airsupra: Airsupra (Albuterol 90mcg & Budesonide 80mcg) Inhalation aerosol is a new rescue medication in USA. The drug is the first approved to combine albuterol (a beta-2 adrenergic agonist) and budesonide (a corticosteroid). It is the first and only 2-in-1 asthma rescue inhaler FDA-approved to treat symptoms and reduce the risk of asthma attacks. It can’t be used for more than 12 puffs (which equals 6 doses) within a 24-hour period and is not to be used as a maintenance treatment for asthma. Currently taking medicine for long-term to maintain control of asthma symptoms, must be continued. It costs around US$ 500 for about 10.7 grams lasting 120 inhalations.
5. Monoclonal Antibodies: The availability of monoclonal antibodies has provided excellent clinical results in properly selected patients. The discovery of new molecules pose challenge to clinicians to select agent case by case. Careful attention to the clinical profile of the patient, targeted investigations of the phenotype and endotype of the individual, and a thorough knowledge of the available evidence will be needed in decision-making as to the choice of the agent

Practical aspects to be considered by clinicians.
The cost of monoclonal antibodies therapy remains a stumbling block for many Indian patients [13].
Indicators to Seek Emergency Treatment: Whenever a patient’s symptoms do not improve, even after using quick-relief medication, Extreme wheezing, or shortness of breath, even during rest, Signs of low oxygen levels, such as fingernails or lips turning blue or grey or SpO2 is less than 90% or patient has trouble concentrating, or in Confusion or agitation S/he needs to be rushed to hospital.
Eosinophilic asthma (EA): EA is a severe form of asthma characterized by high levels of eosinophils in the blood and lungs. Eosinophils promote inflammation, resulting in the tissue damage, mucus production, and hyperresponsive airways that lead to the symptoms of eosinophilic asthma. The symptoms of Shortness of Breath, Coughing, Wheezing, Chest tightness is like that observed in AE. left untreated, inflammation and damage to the lungs caused by eosinophilic asthma leads to permanent thickening of basement membranes in the lungs, causing reduced lung function and poor airflow. EA can be mistaken for COPD due to similarity symptoms and signs. A test for eosinophil count in a blood smear clinches the diagnosis. occasionally, eosinophils in the sputum or a bronchial biopsy or extract bronchial fluid from lungs for evaluation may be needed.
Non-Eosinophilic Asthma (NEA):
TPE is a syndrome of wheezing, fever and eosinophilia seen predominantly in the Indian subcontinent and other tropical areas. Fortunately, only a small percentage (< 0>
Therefore, the endemic districts in these sates need to keep in mind TPE as a possible condition in the differential diagnosis in Asthma like attacks. Tropical Pulmonary Eosinophilia (TPE) is a hyperresponsive pulmonary syndrome in response to trapped microfilariae of lymphatic filariasis caused by filarial nematode Wuchereria bancrofti within the lung tissue.
Some of the TPE manifestation to distinguish it from Asthma include- i) NEA patients usually have late-onset asthma, as aging has been associated with an increase in sputum neutrophil. ii) NEA is more commonly found in obese patients with asthma iii) These patients tend to have poorer asthma control and higher risks of exacerbation iv) Another common feature in NEA asthma is a poor response to inhaled and oral corticosteroid v) Airway neutrophilic inflammation is associated with smoking, road traffic air pollution, inhaled ozone, and other pollutants including nitrogen dioxide. vi)Intensive exercise and cold environment have also been recognized as inducers of neutrophilic asthma. Infective asthma exacerbations cause airway neutrophilia. Moraxella, Streptococcus and Haemophilus species colonization in the airway microbiota is associated with higher sputum neutrophilia and IL-8 concentrations in asthmatic patients. Bronchiectasis is another confounder for sputum neutrophilia. NEA Patients may have bronchiectasis contributing to a neutrophilic or a pleiotropic bronchitis.
The clearance of rapidly opsonised microfilariae from the bloodstream results in a hypersensitive immunological process and abnormal recruitment of eosinophils, as reflected by extremely high IgE levels of over 1000 kU/L. The typical patient is a young adult man /woman from the Indian subcontinent with history midnight fever and rigors. A persistent or recurrent cough that is aggravated at night, along with fatigue, weight loss and a low-grade fever in an individual who has lived or travelled in an area where filariasis is endemic suggests the diagnosis of this disease. Some people with this disease may also have enlarged lymph nodes in the neck, axillae, or inguinal areas. The diagnostic criteria for TPE are: (a) history of residence or travel to a filarial endemic region, (b) paroxysmal and nocturnal cough with dyspnoea, (c) leucocytosis with peripheral blood eosinophilia >3,000/mm3, (d) peripheral blood negative for microfilariae; (e) pulmonary infiltrations in chest x-ray, f) elevated serum IgE and filarial antibody titres, and a clinical response to diethylcarbamazine. A confirmed case of TPE is treated with diethylcarbamazine (DEC) 100 mg 3 times day for 21 days.
A study of 1075 adult patients with severe asthma (GINA treatment: 4/5) of FASE-CPHG study classified as in two groups of patients (EOS- 500/EOS+ 575), based on blood eosinophil counts (cutoff value: 300 G/l). EOS- patients were also described according to their allergic profile based on skin allergy or allergen-specific immunoglobulin E (IgE) assays (cutoff value: 150 IU/mL). The proportion of patients with obesity (29%), allergen sensitization (57%), or ≥2 annual exacerbations in the last 12 months (68%) were similar in both groups. In terms of outcomes as compared with EOS+ patients, EOS- patients less frequently reported chronic rhinitis (41.1% vs 50.5%, p < 0 xss=removed xss=removed>
Recent developments and Recommendations:
1.Logarithm of Latest Approach Recommended to manage Asthma [1]:
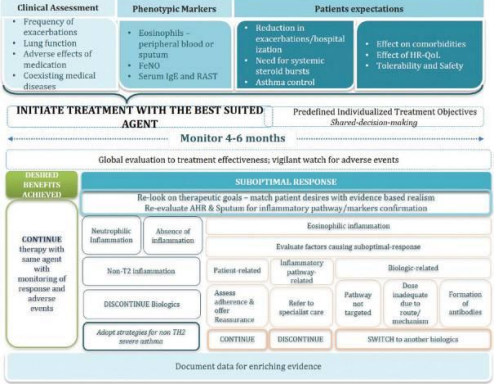
2023 GINA recommend clinical assessment of frequency of exacerbations, lung function, adverse reactions to medications and comorbidities if any. The biomarkers to be assessed include Eosinophils in peripheral blood smear or sputum, F3NO and Serum IgE and RAST. Based on these it is advised to initiate treatment with best suited therapies. After monitoring for 4-6 months if desired benefits are achieved one must continue the same treatment monitoring the response and adverse reactions if any. If the results are sub-optimal general practitioner must refer the case to specialist to evaluate causes of sub-optimal response, who tries to distinguish between inflammation i) either Eosinophilic, or ii) non-eosinophilic or iii) no inflammation at all. Based on the reasons for poor response specialist may suggest using or changing Biologicals or use monoclonal antibodies subject to affordability.
2.Adults & adolescents with poor sleep more likely to have asthma:
A study searched 214 studies of which 23 trials were finally included in the meta-analysis. Sleep disorders were assessed through questionnaires, interviews, or medical records. History of asthma and/or use of asthma medications was the basis for a diagnosis of asthma. Out of the 23 studies included, 18 were cross-sectional and five were cohort studies. The primary analysis revealed that sleep disorders were associated with a higher incidence of asthma with odds ratio (OR) of 1.38.
The risk of asthma was found to be increased when poor sleep quality and insufficient sleep duration were assessed with ORs of 1.10 and 1.20, respectively. When the association was examined according to age group, a higher incidence of asthma was found in adults (OR 1.36) and adolescents aged 12-18 years (OR 1.15). However, the association between sleep disorders and asthma was insignificant in children below 12 years of age (OR 1.13). The association was also nonsignificant (OR 1.16) when the family history of asthma was considered. Based on these findings, the primary care physician must enquire with the patients about sleep problems and interventions to improve sleep quality may help to control the symptoms of asthma like cough, wheeze, dyspnoea. This new study is published in BMJ Open Respiratory Research [11].
3. Improved Health Outcomes for Asthma Patients on Biologics Following Exacerbation
A study presented at the American College of Chest Physicians annual meeting revealed that biologics reduce the incidence of asthma exacerbation. In their analysis, the researchers reviewed retrospective data from 316 asthma patients treated with biologics and 9,645 treated with non-biologic therapy at a Midwest tertiary care teaching hospital between February 2018 and February 2023. In the biologics group, females constituted a higher percentage (69.7%) than non-biologics groups (63.8%). The findings showed that hospitalization rates were 0.9% in the biologics group during the study period, significantly lower than the 6.5% observed in the non-biologics group. Additionally, the biologics group had fewer ICU visits (0.3% vs. 1.8%) [13]. In India available biological are Omalizumab and Mepolizumab. Omalizumab is used in patients with moderate to severe allergic asthma irrespective of the eosinophilic status if an allergic phenotype is associated. Mepolizumab is indicated for severe eosinophilic asthma [12, 13].
4.Indirect Airway Hyperresponsiveness Test Enhances Asthma Control in Children
Indirect challenges cause the release of endogenous mediators that cause the airway smooth muscle to contract and the airways to narrow. Airway sensitivity to indirect challenges is reduced or even totally inhibited by treatment with inhaled corticosteroids (ICS), so a positive response to an indirect stimulus is believed to reflect active airway inflammation. The indirect challenges commonly used in pulmonary function laboratories include exercise, eucapnic voluntary hyperpnea, hypertonic (4.5%) saline, and mannitol. Exercise was the first test to be standardized and was used to identify exercise-induced bronchoconstriction (EIB). The inhibition of EIB in young children by sodium cromoglycate led to the concept that mast cells were important very early in the onset of asthma [10, 11].
5. Outcomes of Comorbid Asthma and Eosinophilic Esophagitis:
A retrospective cross-sectional study to characterize asthma in patients with/without eosinophilic esophagitis presented in the annual meeting of the American College of Chest Physicians 2023 reported that Patients who have asthma along with eosinophilic esophagitis are more likely to visit the hospital at a younger age compared to patients who only have eosinophilic esophagitis. This study showed that patients who have both asthma and eosinophilic esophagitis, present for admission at a younger age compared to patients who just had one of the two diseases suggesting that their concomitant presence may have an “additive effect” on the age of hospital presentation. The authors hypothesise that “multiple atopic processes working together to cause a stronger inflammatory response” may lead to patients seeking care at an earlier age. Clinicians treating patients with asthma or any other atopic disease, should bear in mind that the patient may have another such condition. Presence of two or more atopic conditions increase the likelihood of disease exacerbations necessitating hospital visits. Patients should also be educated about this, so that they can better monitor their symptoms and seek timely medical care, when needed [15].
Asthma is a common heterogeneous lung disease that affects people of all ages, characterized by chronic airway inflammation, diagnosed mostly by the history of shortness of breath, wheeze, cough, and chest tightness that vary over time and in intensity, with variable expiratory airflow limitation.
Lung function tests play a crucial role in evaluating asthma control and should be assessed at diagnosis, start of treatment, post 3-6 months of controller treatment and periodically thereafter.
The general approach to treatment of an acute asthma exacerbation consists of inhaled beta-agonist therapy - Albuterol), bronchodilators as well as systemic glucocorticoids in most patients.
Asthma medications in inhaled form are considered better as compared to systemic formulations (oral/IV) to improve clinical outcomes, as they work faster to improve the symptoms and are safer as compared to oral or IV route.
Initial treatment (beta-agonist therapy and oral glucocorticoids) of acute asthma exacerbations can be provided in the primary care setting or even at home.
Children with moderate-to-severe exacerbations require close observation for clinical deterioration, frequent treatments, and repeated evaluation, Therefore, it is better that, most children with moderate or severe asthma exacerbations be managed in an emergency inpatient setting.
Pharmacotherapy is only one aspect of asthma management, and a focus on a treatable traits approach might provide substantial benefits.
With the advent of Airsupra and Monoclonal antibodies, ongoing research is needed to improve understanding and simplify the practice in Asthma treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
