
case report | DOI: https://doi.org/10.31579/2690-1897/186
1Surgical Fellow Department of Cardiothoracic Surgery Allegheny General Hospital USA.
2Surgical Resident Department of General Surgery Lehigh Valley Health Network USA.
3Surgical Resident Department of General Surgery Lehigh Valley Health Network USA.
4Division of Surgical Oncology Lehigh Valley Health Network USA.
*Corresponding Author: Aryan Meknat, Surgical Fellow Department of Cardiothoracic Surgery Allegheny General Hospital USA.
Citation: Aryan Meknat, Samuel Yellin, Jasmine Hwang, Aaron Blackham, Jeffrey Brodsky, (2024), Management of Acute COVID-19 and Multi-system Organ Failure in a Post-operative Esophagogastrectomy Patient, J, Surgical Case Reports and Images, 7(3); DOI:10.31579/2690-1897/186
Copyright: © 2024, Aryan Meknat. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2024 | Accepted: 18 April 2024 | Published: 26 April 2024
Keywords: COVID-19; esophagectomy; post-operative period
Esophagogastrectomy is the cornerstone of curative treatment for esophageal cancer. Peri-operative COVID-19 infection has been shown to be an independent predictor of surgical mortality. A 65-year-old male ex-smoker who had been vaccinated for COVID-19 presented with Barrett’s esophagus with high grade dysplasia and well-differentiated adenocarcinoma of the distal esophagus. With no evidence of metastatic disease, he underwent upfront open Ivor-Lewis esophagogastrectomy. Post-operative extubation was unsuccessful. A COVID-19 test was positive. He developed multi-system organ failure, requiring continuous renal replacement therapy and tracheostomy. He was treated with steroids and remdesivir. He was discharged to inpatient rehabilitation after decannulation. Despite his critical illness, COVID-19 infection, steroid treatment, and smoking history, multiple imaging studies did not demonstrate an anastomotic leak. Despite evidence to suggest a significantly higher mortality in patients who develop COVID-19 in the post-operative period, our patient did not succumb to his critical condition in this period.
Management of esophageal cancer requires a multi-disciplinary approach, often requiring neoadjuvant and/or adjuvant therapy. When feasible, an esophagogastrectomy is the cornerstone of curative treatment for patients with esophageal or gastro-esophageal junction cancer. Based on data from the Society of Thoracic Surgery General Thoracic Database, the overall anastomotic leak rate for esophagogastrectomy is reported as 10.9% [1]. Well known factors that contribute to the development of an anastomotic leak include: obesity, chronic steroid use, diabetes, renal insufficiency, tobacco use, and procedure duration greater than five hours [1].
There is concern that the COVID-19 pandemic impacted prognosis of cancer patients due to delays in treatment, and increased susceptibility to infection given their immunocompromised state. Peri-operative COVID-19 infection has been shown to be an independent predictor of surgical mortality [2]. Bhanghu, et al [2]. reported that COVID-19 infection was associated with a 30-day mortality rate of 23.7% and a pulmonary complication rate of 50.9%. Given the relatively high incidence of pulmonary complications following esophagectomy, patients who also develop COVID-19 infection during the perioperative period would be at particularly high risk of complications.
We report the case of a middle-aged man who underwent an open Ivor-Lewis esophagogastrectomy for a distal esophageal adenocarcinoma who subsequently developed COVID pneumonia and multi-system organ failure. Consent was obtained from the patient for submission of this case report.
A 65-year-old male with a history of obesity, diabetes mellitus type 2, depression, COPD on home oxygen, sleep apnea and 30-pack-years smoking history presented with Barrett’s esophagus with high grade dysplasia and well-differentiated adenocarcinoma of the distal esophagus following an EGD for dysphagia (Figure 1). There was no radiologic evidence of regional or distant metastases on pre-operative PET scan (Figure 2). Due to the patient’s chronic pulmonary disease and home oxygen use, upfront surgical resection was recommended to avoid further pulmonary dysfunction potentially caused by neoadjuvant chemoradiation. The patient had received two doses of the COVID-19 Moderna vaccine.

Figure 1: EGD image of tumor – revealing a mucosal lesion with underlying high-grade dysplasia and well-differentiated adenocarcinoma of the distal esophagus
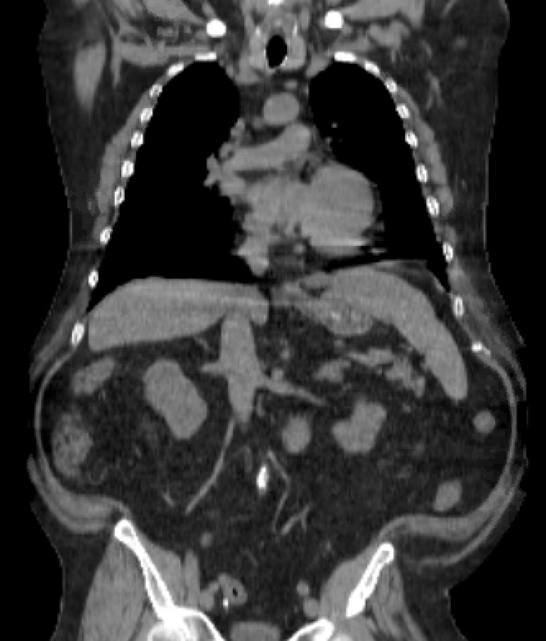
Figure 2: Representative image of pre-operative PET-CT scan demonstrating gastroesophageal junction mass without PET avidity. No metastatic disease was identified on pre-operative PET-CT imaging.
After pre-operative medical optimization, the patient underwent an open Ivor-Lewis esophagogastrectomy and placement of a feeding jejunostomy. The patient failed immediate post-op extubation due to hypercapnic respiratory failure and was subsequently re-intubated. The patient was transferred to the surgical intensive care unit, where a COVID-19 test revealed an active infection. Within 48 hours, the patient developed oliguric acute kidney injury, requiring continuous renal replacement therapy, and hemodynamic instability, requiring vasopressor support. The patient spent seven weeks in the ICU with labile hemodynamics, slow ventilator weaning, and poor neurologic status. His COVID pneumonia was treated with a 10-day course of dexamethasone 6mg daily and 5-day course of remdesivir 100mg daily. His respiratory failure was supported by prone positioning and permissive hypercapnia. He eventually required tracheostomy.
He was ultimately weaned from the ventilator and transitioned to intermittent hemodialysis. He regained renal function and had his tracheostomy decannulated. He was discharged to inpatient rehabilitation on post operative day 55. Throughout his admission, he had multiple Chest CT scans and esophagrams which indicated there was no anastomotic leak to explain the source of his sepsis and multisystem organ failure (Figure 3).

Figure 3: Post-operative CT scan during period of active COVID-19 infection with ongoing steroid and antiviral treatment demonstrating gastric conduit without evidence of intrathoracic leak.
The incidence of breakthrough COVID-19 infections is still an area of concern and investigation. Patients with active malignancy and those in the perioperative setting remain particularly vulnerable. Providers must be well-versed in managing both routine post-operative concerns following major oncologic resections, and potential complicating factors related to acute COVID-19 infections. A large study of patients from Veterans Affairs hospitals demonstrated that those who developed COVID-19 in the post-operative period had significantly higher rates of 30-day pulmonary complications, major complications or any complication [3]. Patients who have surgery within 4 weeks of COVID-19 infection have 208% higher risk of developing postoperative respiratory failure [4]. At 8 weeks following COVID-19 infection, the risk of postoperative respiratory failure returns to the same as pre-COVID-19 levels [4].
A major component of the treatment for severe COVID-19 infection, in addition to lung-protective ventilation strategies and antiviral therapies, is steroids. Steroids have been shown to lead to delayed wound healing, thus impeding the ability of the individual to heal an enteric anastomosis1. As a result of infection with COVID-19, many patients who become critically ill also develop acute renal failure. Renal failure also has an association with the generation of an anastomotic leak after esophagectomy [1].
This patient managed to survive post-operative COVID-19 infection, in spite of evidence that suggests a significantly higher mortality in patients undergoing elective cancer surgery who develop COVID-19 within 30 days of surgery.
The authors received no financial support for the research, authorship, and/or publication of this article.
The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
