
Case Report | DOI: https://doi.org/10.31579/2690-1897/130
1 Assistant Professor, Interventional Radiologist, Radiology Department, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia
2 Professor of Surgery, Upper GI Surgery Unit, General Surgery Division, Department of Surgery, King Saud University, Riyadh, Kingdom of Saudi Arabia
3 Minimally Invasive and Bariatric Surgery Fellow, Upper GI Surgery Unit, General Surgery Division, Department of Surgery, King Saud University, Riyadh, Kingdom of Saudi Arabia
4 General Surgery Resident, Upper GI Surgery Unit, General Surgery Division, Department of Surgery, King Saud University, Riyadh, Kingdom of Saudi Arabia
*Corresponding Author: Wadha AlOtaibi. General Surgery Resident, Upper GI Surgery Unit, General Surgery Division, Department of Surgery, King Saud University, Riyadh, Kingdom of Saudi Arabia.
Citation: Naif Alsaikhan, Mohammed Alnaami, Fahad Almadi, Wadha AlOtaibi. (2023), Management of a Late and Complex Leak after Sleeve Gastrectomy along with Endoluminal Stent Complications: Lessons Learned, J. Surgical Case Reports and Images, 6(1) DOI: 10.31579/2690-1897/130
Copyright: © 2023 Wadha AlOtaibi. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 October 2022 | Accepted: 29 October 2022 | Published: 06 January 2023
Keywords: sleeve gastrectomy; leak; stent; complications
Laparoscopic sleeve gastrectomy (LSG) is the most commonly performed bariatric procedure worldwide. The most serious complication is gastric leakage. We present a case of morbidly obese patient with multiple comorbidities who was complicated by late gastric leak due to persistent smoking and use of steroids for the treatment of bronchial asthma exacerbations. Due to the large leak size, he was managed initially by external drainage and endoluminal mega stent that was unfortunately complicated by esophageal perforation. Surgical closure of the esophageal perforation was successful to control sepsis from acute mediastinitis; however, it was reopened few days later but controlled externally with the chest tube. A conservative management approach was advised by a multidisciplinary committee conference, which was followed for many months without evidence of leaks closure. Subsequently, the gastric leak and esophageal perforation were successfully managed by the interventional radiology using internal drainage and septal occluder plug for the gastric leak and esophageal perforation respectively.
Laparoscopic sleeve gastrectomy (LSG) is the most commonly performed bariatric procedure worldwide. Although it has been widely adopted due to its simplicity and excellent weight reduction outcomes, it has a considerable risk of postoperative complications [1]. The most serious complication is gastric leakage, with an overall prevalence of 1%–5% for primary procedures [2,3], which can increase up to 10% for revisionary procedures [4]. Moreover, the incidence of complications increases several folds with the presence of associated risk factors, such as smoking, steroid use, immunosuppressive and biological agents, diabetes mellitus, and obstructive sleep apnea requiring perioperative positive ventilatory support [5,6]. Complications also imply a lengthy hospital stay with higher costs and an increase in morbidity and mortality rates [7,8].
Management of such complications has evolved with the growing experience in bariatric surgery along with other ancillary services. A highly specialized multidisciplinary approach, including experienced bariatric surgery, therapeutic endoscopy and interventional radiology services, adequate resources, and highly specialized bariatric centers are required to deal with difficult bariatric interventions and complications [9,10,11].
We report an unusual case of complex late gastric leak post-LSG complicated by stent esophageal perforation, with the lessons learned from the various disciplines’ management approaches.
A 37-year-old man who was living with severe obesity (BMI = 77.7 kg/m2) associated with backache and bilateral knee osteoarthritis, known asthmatic on regular low-dose prednisolone and salbutamol puffers, and had been a heavy smoker. Due to his severe obesity, the patient was offered single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) as a one- or two-stages procedure. The patient preferred the two-stages procedure (i.e. LSG then SADI at a later date). After adequate preoperative preparation and smoking cessation, he underwent an uneventful LSG on July 1, 2020. He was discharged the next day in good condition, visited the clinic once in the early postoperative period, but failed to return afterward. Almost one year later, he presented to another hospital with symptoms and signs of sepsis due to a significant gastric leak (Fig. 1).

Figure 1. Fluorography showing the significant gastric leak with a cavity
As that hospital lacked therapeutic endoscopy and interventional radiology facilities, he underwent exploratory laparoscopy, washout, and drainage. After a good recovery and stabilization, he was transferred to our facility. Initially, he was treated empirically with broad-spectrum antibiotics and antifungals, then placed on parental nutrition (PN). Computed tomography (CT) of the abdomen revealed a small residual collection at the leak site near the gastroesophageal junction (GEJ) that was drained externally under CT guidance using a pigtail catheter. The endoscopic assessment revealed a large hole at the staple line, just below the GEJ (Fig. 2). Given the size of the leak, a long covered endoluminal mega stent was placed. After a few days while on a liquid diet, the patient developed progressive hematemesis refractory to medical treatment. An emergent endoscopic assessment revealed pressure erosions of the esophageal mucosa from the stent.

Figure 2. Endoscopic assessment revealed a large hole at the staple line with a visible pigtail end at the collection site.
The bleeding was thereafter controlled after removal of the stent. The patient was kept nil per mouth (NPO) and put on a high-dose proton pump inhibitor (PPI). A few weeks later, another long covered endoluminal stent was placed to seal the gastric leak, but the patient developed severe chest pain and tachycardia afterward. Unfortunately, the gastrograffin swallow revealed an esophageal perforation at the upper edge of the stent that had eroded and perforated the esophagus at the mid-esophageal level (Fig. 3). The patient was taken to the operating room for emergency repair.
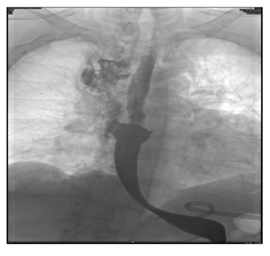
Figure 3. Fluorography showing the esophageal perforation site.
Thoracoscopic repair attempts failed due to excessive bleeding and poor visualization of the perforation. Open thoracotomy was then performed, followed by endoscopic removal of the stent, placement of a nasojejunal feeding tube under direct visualization, primary closure of the esophageal perforation using double-layer repair, and placement of the right chest tube. A few days later, contrast studies revealed dehiscence of the esophageal repair, with the esophageal contents leaking into the right chest tube with a persistent gastric leak through the percutaneous pigtail drainage. At this stage, a multidisciplinary conference was convened, and a decision was made to continue a conservative management approach only. He was kept on NPO and nasojejunal feeding alternating with PN for several months without noticeable improvement of both the esophageal and gastric leaks.
Later imaging showed migration of the abdominal pigtail catheter into the gastric lumen through the large gastric hole. Instead of repositioning of the drain, it was removed, and an internal drain (double J stent) was placed percutaneously, with one end looped in the stomach and the other kept unlooped to anchor it in place to avoid stent dislodgment. Fortunately, this was successful in managing the gastric leak internally. A few attempts to embolize the esophageal leak with coils and glue were unsuccessful, with the dislodgment of the coils shown in follow-up studies. Eventually, the esophageal leak was successfully embolized using a plug (type 2 Amplatzer, 8 mm) sealed with a cohesive agent (Figs. 4 and 5). After two weeks, follow-up contrast studies showed no leakage, neither from the esophagus nor from the gastric holes. The patient was placed on clear liquid and then advanced to a full liquid diet. The pleural drain was removed, and he was discharged home. He was then placed on a regular diet one month after hospital discharge without any issues. His second visit after 3 months to the clinic showed no clinical or biological evidences of sepsis or malnutrition. However, he was not walking well due the long hospital stays on bed. He was advised to go for intensive physical and functional rehabilitation at his hometown.

Figure 4. Amplatzer septal occluder device
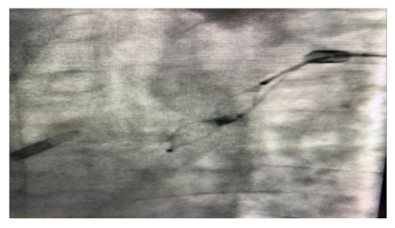
Figure 5. The septal occluder in place after deployment into the esophageal perforation.
Gastric leak after sleeve gastrectomy is associated with a significant morbidity and mortality rate of greater than 0.14% [12]. Leaks after LSG remain one of the most feared complications. They can present as acute (within 1–2 weeks), early (within 6 weeks), and late leaks (after 6 weeks) with a contained abscess and sepsis, as in our case [13]. The ideal intervention after a confirmed leak post-sleeve gastrectomy depends on the time of presentation and the available resources and expertise. Most authors recommend surgical intervention for acute leaks to control sepsis, with or without primary repair, abdominal washout, and adequate drainage [14]. Early leaks are usually contained; therefore, the best option is to drain the collection area and control the leak site by endoluminal stenting or double pigtail internal drainage, depending on the perforation size and available resources and expertise [15]. Late leaks, however, are more challenging due to the chronicity of the leak site and its refractory nature to most interventions. Our patient experienced a significant leak, with the opening size measuring about 2 cm in diameter almost one year after the primary procedure. Although the patient was managed well initially with laparoscopic surgical intervention, less invasive interventions, such as interventional radiological drainage and insertion of the endoluminal stent, could have been a better option.
Endoscopic placement of fully covered stents is a minimally invasive and effective alternative to surgery for managing leaks after bariatric surgery. The reported success rate of leak closure is about 88% [16]. However, stents are not that easily tolerated by patients and have well-known complications, such as strictures, erosions with bleeding, and perforations that can be very challenging to manage, as happened to our patient. Recently, the internal drainage of gastric leaks using double pigtail catheters has emerged as an excellent alternative to endoluminal stents, as they have a much lower complication rate, very well tolerated by patients, and success rates are as effective as endoluminal stents [17,18]. Internal drainage; however, is more successful for small leaks (< 1> 1 cm), as it cannot hold in place [16]. In retrospect, insertion of a percutaneous pigtail catheter for our patient could have been an ideal step to start with before stent insertion, as it was an unfortunate and unexpected complication of esophago-gastric stenting, causing a challenging perforation. Diagnosis of esophageal perforation can be difficult, mainly due to non-specific symptoms. The patient’s chest pain was initially thought to be procedure-related. Repeat contrast studies should be obtained whenever there is clinical suspicion, even in patients with negative initial imaging studies [19].
Esophageal perforations continue to report high morbidity and mortality rates of more than 29% [20]. More than half of the perforations are iatrogenic and are mostly related to endoscopic instrumentation used in the upper gastrointestinal tract [21,22]. The risk of perforation after endoscopic esophageal stent placement can reach up to 25% [22]. Timely diagnosis and appropriate treatment of esophageal perforation remain challenging but essential for such patients. Surgical repair of esophageal perforation is a life-saving intervention, especially when performed within 24 hours of the event [23].
Currently, endoscopic management of esophageal perforations is preferred over surgical intervention, especially for hemodynamically stable patients [24]. Success rates of endoscopic interventions vary according to the perforation site and size. If the perforation is in the upper third, stenting is not applicable, and clipping is more appropriate. However, clipping is only possible for small perforations < 2> 2 cm, clipping is not applicable, and stents can be utilized [25].
Nonoperative treatment is also possible for some patients with iatrogenic perforation without systemic symptoms of infection and compromised hemodynamics. In such cases, careful observation, NPO, and appropriate treatment with intravenous broad-spectrum antibiotics, PPIs, and nutritional support may be sufficient for successful treatment [25,26].
Radiologically-guided methods for fistula closure include placement of mechanical agents such as coils and plugs and liquid embolic agents such as tissue glue (n-butyl two cyanoacrylates) and (ethylene-vinyl alcohol copolymer based liquid embolic). Coils are excellent embolizing agents in blood vessels. However, in the GI tract, a more stable mechanical agent is needed to resist dislodgment by peristalsis. The type 2 Amplatzer plug was a logical choice in our case, as it provides marked stability with its double configuration. Additionally, adding a sealing agent was critical to occlude the spaces between the wire mesh. While plugs are, in general, more expensive than coils, their stability makes them an excellent option for occluding fistulous tracts [27]. These mechanical agents, as well as liquid embolic agents, can be delivered via small catheters that can be placed transnasally without anesthesia [28].
The management of late gastric leaks after sleeve gastrectomy is challenging and refractory to many interventions. Judgmental non-surgical approaches, whether interventional radiology (IR) and/or endoscopic management of such leaks, should be considered depending on availability of the expertise and equipment. Surgical interventions are considered the last approach if IR and endoscopic interventions are not applicable or failed to control the leak site.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
