
Research Article | DOI: https://doi.org/10.31579/2578-8965/205
1Department of Obstetrics & Gynaecology, AIIMS Jodhpur.India
2Additional Professor, Dept. of Obstetrics &Gynaecology, AIIMS Jodhpur. Rajasthan, India.
3Professor and Head, Dept. of Obstetrics &Gynaecology, AIIMS Jodhpur.
*Corresponding Author: Manu Goyal, Additional Professor, Department. of Obstetrics &Gynaecology, AIIMS Jodhpur. Rajasthan, India.
Citation: Shafak Bhandari, Manu Goyal, Pratibha Singh, (2024), Male Infertility – An Overview of Management, J. Obstetrics Gynecology and Reproductive Sciences, 8(3) DOI:10.31579/2578-8965/205
Copyright: © 2024, Manu Goyal. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 February 2024 | Accepted: 29 February 2024 | Published: 07 March 2024
Keywords: follicular output rate; fort; fsh; controlled ovarian hyperstimulation / ivf-et
Male factor infertility is responsible for about 2/5th cases undergoing IVF.1,2 An exponential rise in male infertility is being driven by constantly shifting societal ideals, career demands, widespread obesity, associated stress and delayed parenthood.2,3 Semen analysis is the keystone in evaluating male fertility with WHO guidelines providing the basis for procedural standardization and reference values worldwide. They have been time and again revised since 19801,2 However, documented evidence emphasis the need of comprehensive history, physical and genital examination and hormonal analysis for complete management. FSH, LH, prolactin and testosterone are the key hormones required in evaluating between different etio-pathological categories of male infertility which are hypo gonadotrophic hypogonadism, primary testicular failure, obstructive and unexplained causes 3,4,5 Categorization of cases helps in delineating the specific management and further medical or surgical treatment required. Over the years, the role of IUI has reduced to couples with moral, ethical, physical and financial issues to IVF/ICSI.3,5 Male infertility treatment has been revolutionized by ICSI. Advancements as surgical sperm retrieval in form of PESA, TESA, MESE and TESE has allowed azoospermic men the opportunity of biological paternity. For men with complete spermatogenesis failure, only treatment option is insemination with donor sperms or adoption. 3,5,6
Infertility is defined as the “inability to achieve spontaneous pregnancy within one year of regular unprotected sexual intercourse”.1 Infertility solely due to male factor is responsible in 20-30percent cases and as contributory factor in additional 30percent of cases.1,2
Causes of male infertility can be broadly subdivided into 4 categories3,4,5
1.Hypogonadotropic hypogonadism
2.Obstructive causes
3.Primary testicular failure
4.Unexplained causes
Hypogonadotropic hypogonadism
Hypogonadotropic hypogonadism constitutes hypothalamic pituitary dysfunction, accounting upto 2percent cases.3 Causes include Idiopathic isolated gonadotrophin deficiency, Kallman’s syndrome, Single gene mutation (involving the GnRH receptors, FSHB, LHB or transcription factors involved in pituitary development), Hypothalamic and pituitary tumours (macroadenoma, craniopharyngioma) , Infiltrative diseases (sarcoidosis, histiocytosis, transfusion siderosis), Hyperprolactinemia, Drugs (GnRH analogs, opiates, oestrogen, glucocorticoids), Critical illness of injury, Chronic illness, malnutrition, Infection (eg-meningitis), Obesity. These causes are frequently correctable3,5,6,7
Obstructive causes
Obstructive causes are sperm transport mechanism failure and constitute 10–20percent cases3,4 The causes are epididymal obstruction or dysfunction, congenital bilateral absence of vas deferens, Vasectomy, Infections causing obstruction of vas deferens (eg-tuberculosis, gonorrhoea, Chlamydia), Young syndrome, Kartagener syndrome (primary cilia dyskinesia), Ejaculatory dysfunction (eg-spinal cord disease, anatomic dysfunction). They constitute frequently correctable conditions3,6
Primary testicular failure
Primary testicular failure is characterized by gonadal failure and accompanies testicular atrophy. Observed in 30-40percent total cases and 25percent are due to genetic causes3,5 Common disorders are Klienfelter’s syndrome, Y chromosome deletions, Single gene mutation and polymorphism (eg-Involving androgen, estrogen or FSH receptor), Cryptorchidism, Vasucular causes - Varicoceles, torsion, Infections (eg-viral orchitis, leprosy, tuberculosis), Drugs (eg-alkylating agents, alcohol, antiandrogens, cimetidine), Radiation, Environmental gonadotoxins (eg-heat, smoking), Chronic illness (renal insufficiency, cirrhosis, cancer, sickle cell disease, amyloidosis, vasulitis) Most of these causes are irreversible4,6
However, 40-50percent cases have unexplained or idiopathic causes [3,4]
Unexplained causes
In case of male infertility, points to emphasise are personal history, clinical examination, semen analysis and hormonal tests- FSH, LH, Testosterone, Prolactin. More detailed testing in form of genetic tests and sperm function tests may be necessary depending upon these initial results1,2,3
History
Age is usually not a significant factor till 45 years. There is increased risk of autism, schizophrenia, bipolar disorders in offspring beyond 50 years.
Occupation is important as certain chemical and radiation exposure is harmful.
General wellbeing of the patient is important. Stress on diabetes, anosmia, respiratory issues, galactorrhea.
Smoking, alcohol and drugs as anabolic steroids, chemotherapy, recreational drugs (marijuana) affect sperm quality and quantity
Past history involving infections (Mumps, STDs, prostatitis) , groin trauma, surgeries for hernia, hydrocele, cryptorchidism, vasectomy
Developmental growth pertaining to onset of puberty should be enquired. Sexual history and history pertaining to androgen deficiency are crucial. Ask regrading libido, sexual intercourse frequency, previous conceptions, previous fertility treatment,ejaculation problems, shaving frequency, loss of body hair or muscle mass, breast tissue development, voice change
Family history of hereditary disorders
Relevant history of female partner is equally important3,6,7
General, physical and genital examination
Look for built of the patient. Healthy male endocrine pattern can be identified on basis of low-pitched voice, male pattern, distribution and amount of axillary hair, pubic hair and beard. Consistently high-pitched voice, gynaecomastia and reduced masculine muscle mass are indicators of hypogonadism prior to puberty3,6,7
Local examination of male genitalia involving testis and scrotum is done. Testis are measured for their volume and consistency. Testicular volume is measured with Prader orchidometer, which is twelve numbered wooden or plastic beads string ranging in size from 1-25ml.Testicular growth indicates pubertal development. Volume less than4 ml -prepubertals, 4–15 ml peri-pubertals and 12–25 ml adults. Hard consistency signifies malignancies while soft consistency shows loss of germinal tissue. Inspect scrotum for scars of previous surgeries, palpate for any masses, varicocele and palpable epididymis. Varicocele is confirmed performing Valsalva manoeuvre. Normal adult penile length is 10-17 cm. Examine for presence of hernias and signs of STDs3,6,8
Klinefelter's syndrome is suggested by small testes, phallus and prostate, sparse hair, unusually lengthy limbs and legs and delayed epiphyseal closure3,7,8
Semen Analysis: It holds an undisputable key role in diagnostic process of male infertility. Terminology associated with semen analysis are in Table [11,2,5,6]
| Normozoospermia | All semen parameters normal |
| Oligozoospermia | Reduced sperm numbers Mild to moderate: 5-15 million/mL Severe: less than 5 million/mL |
| Asthenozoospermia | Reduced sperm motility |
| Teratozoospermia | Increased abnormal forms of sperms |
| Oligoasthenoteratozoospermia | Sperm variables all subnormal |
| Azoospermia | No sperms in semen |
| Aspermia (anejaculation) | No ejaculate (ejaculation failure) |
| Leucocytospermia | Increased white cells in semen (>1 x 10*6) |
| Necrozoospermia | All sperms are non-viable or non-motile |
Table 1: Semen analysis terminology
| Semen parameter | Normal value |
| Semen Volume (ml) | 1.4 (1.3-1.5) |
| Total sperm number (106 per ejaculate) | 39 (35-40) |
| Total motility (%) | 42 (40-43) |
| Progressive motility (%) | 30 (29-31) |
| Non progressive motility (%) | 1 (1-1) |
| Immotile sperms (%) | 20 (19-20) |
| Vitality (%) | 54 (50-56) |
Table 2: Normal semen parameters
Indian research reports 22.4- 64.2percent prevalence of deranged semen parameters amongst infertile couples. Azoospermia accounts for 1percentof all men and 15-20percentof infertile men. [3,5,10] Semen is tested after 3-5 days of abstinence. A single semen analysis has false positive rate of 10percent while two tests will falsely identify only 2percent men as having abnormal semen parameters. Ideally repeat sampling is done after 3 months. However, it can be scheduled earlier at 6-8 weeks if the delay is causing undue anxiety to patient. Repeat analysis in case of azoospermia should be performed in 2–4 weeks. [1,2,10]
Hormone analysis
FSH, LH, prolactin and testosterone are the key hormones required in evaluating between different aetio-pathological categories of male infertility [3,4]
| Endocrinology | Semen Analysis | Testicular Examination | Likely diagnosis |
Elevated FSH, Normal to high LH, Low to normal testosterone | Normal volume, Severe Oligozoopermia/ Azoospermia | Low to normal volume testis, soft consistency, usually palpable vas, +/-varicocele | Hypergonadotrophic hypogonadism |
Low FSH Low LH Low testosterone Hyperprolactinemia +/- | Severe Oligozoopermia/ Azoospermia | Low volume testis, firm consistency, usually palpable vas | Hyogonadotrophic hypogonadism |
Normal FSH Normal LH Normal testosterone | Low volume, Severe Oligozoopermia/ Azoospermia | Nearly normal testis volume Dilatation of epididymis +/- non palpable vas | Obstructive pathology Retrograde ejaculation Idiopathic male infertility |
Low FSH Low LH Normal testosterone | Normal volume, Oligozoopermia/ Azoospermia | Normal volume testis | Illicit drug abuse, Exogenous testosterone |
Table 2: summarizes the patient endocrine profile and its correlation with semen analysis and testicular examination and likely diagnosis.
Single raised FSH value holds more significance than LH value due to its longer half-life. Morning testosterone sample is preferred due to diurnal variations.Total circulatory testosterone level is dependent on sex hormone binding globulin (SHBG). Disorders such as Hyperthyroidism, liver disease and oestrogen excess have increased SHBG resulting in total circulatory testosterone values to be within normal limit. However, obesity, hypothyroidism, Type 2 diabetes and acromegaly have low SHBG, so falsely sub-normal total testosterone levels. In spite of low production of testosterone 40percentof Klienfelter’s patients may be tested to have normal range testosterone levels due to increased SHBG levels following androgen excess. [3,4,11,12]
Imaging: Routine scrotal and testicular ultrasonography is not advised.Indications include inconclusive diagnosis or clinically palpable pathology.[3,13] It helps improving detection of scrotal pathologies and information on testicular volume. Varicocele (most common), hydrocele, epididymal cyst and spermatocele are common pathologies diagnosed. [3,4,10] Suspected cases of obstructive azoospermia with palpable vas deferens calls for trans-rectal USG. Renal imaging is advised when either unilateral or bilateral vas deferens is absent (10-25percent renal agenesis). Cranial MRI is suggested for patients with hyperprolactinemia or with presence of visual symptoms. [5,13]
Genetic testing: There is 15 times higher chances of detecting chromosomal anomalies in severe male infertility compared to fertile males, signifying genetic screening in specific patients.14Genetic counselling is done for conditions with autosomal dominant inheritance pattern. Fundamental genetic tests recommended are Karyotype, Y micro-deletions (Azoospermia factor- AZF deletions) and cystic fibrosis trans-membrane conductance regulator (CFTR), if sperm concentration less than 5 million/ml [3,4]
Offer karyotype and Screening of Y chromosome microdeletion to men with non-obstructive azoospermia or severe oligospermia who are candidates for IVF with ICSI.3 Chromosomal abnormalities by peripheral karyotype testing are present in about 7percent infertile, 5percent oligospermic and 15 % azoospermic men.4 Genetic testing to diagnose FSH receptor defect and other spermatozoa epigenetic are currently used in research settings only. The most common numeric chromosomal anomaly encountered among infertile men is Kleinfelter’s syndrome affecting 1 in 600 males and accounting 14% of azoospermic cases.14 AZFa, AZFb, AZFc deletions are identified in 10percent,12percent and 2percent of oligospermic men. AZFc deletions accounts for 80% of these mutations whereas AFZa leads to complete testicular germ cell atrophy. [4,5] Prior to surgical sperm retrieval in these individuals, genetic counselling should be prioritized due to possible risk of passing on these genetic abnormalities to offsprings. These microdeletions will, through ICSI, be transmitted to sons who most probably will be infertile as well. However, ICSI children are too young to evaluate their fertility status.3,14 Upto 95percent men with clinically manifested cystic fibrosis are infertile and congenital bilateral absence of vas deferens (CBAVD) is most common underlying cause with mutations in CFTR gene. It should be presumed that CBAVD patients have mutations, so testing for carrier status in female partners should be done.[3,4,14]
Sperm function tests: help in assessing functional characteristics including sperm motility, hyperactivation, mucus penetration, zona interaction and acrosomal reaction. They are based on sperm proteomics, metabolomics, mitochondrial metabolism and signalling system essential for fertilisation. They are not used in daily practice. The common ones are Cap-score assay, sperm capacitation index, zona-free hamster oocyte penetration assay, CatSper expression testing. [4,5,6,10]
Testicular biopsy: for diagnosis in infertile males is not recommended. It can be taken in setting of surgical sperm retrieval sent for histopathological examination to evaluate spermatogenic capacity of testis. [3,4,12]
Management
Lifestyle factors
Vaginal intercourse every alternate day maximises odds of natural conception and should be recommended, as timed intercourse may be emotionally stressful. Stress can be a contributing factor to male subfertility.14 Early recognition and providing psycho-therapy is useful. Healthy diet rich in carbohydrates, fibre, folate, lycopene,fruits and vegetables with lesser fats is useful. Excessive alcohol consumption is damaging to semen quality but 3 to 4 units per day are unlikely to have adverse effect.4,5 Association between caffeinated beverages and male sub-fertility has not been proven. Although there is debate on the benefits of wearing loose-fitting underwear to increase fertility, elevated scrotal temperature is linked to inferior semen parameters.3,6,14
Obesity deteriorates semen quality by lowering testosterone levels. Studies inform that males with BMI > 30kg/m2 take longer to conceive. Improved semen scores were found in physically active men with who exercised 3-4 hours/week. [5,14]
Hypogonadotropic hypogonadic infertility
Gonadotrophins:Use Human chorionic gonadotrophin (hCG) or Pulsatile gonadotrophin-releasing hormone (GnRH) for 3-6 months followed by combination of FSH and LH to initiate spermatogenesis by stimulating Leydig cells for normalisation of intra-testicular testosterone. During treatment, measure testosterone levels every 1-2 months, target level 400-900ng/dL. The best response is seen in individuals with post-pubertal onset of gonadotrophin deficiency and testicular volume >8mL. They have good outcomes resulting in normalization of testicular function in 80percent with 50percent–70percentpregnancy rates. Start with hCG alone, in case of failed response, combined treatment with hCG + hMG or pure FSH (75-150 IU three times weekly) is advised. [4,7,11,12]
Hyperprolactinoma is a treatable cause and usually responds to bromocriptine or cabergoline.7,12 Gonadotrophins, bromocriptine, SERMs (clomiphene citrate and tamoxifen) do not confer benefit in unexplained male sub-fertility.3,11 Exogenous steroids should be stopped. After stopping testosterone use, azoospermia recovers to concentration of 6.5 million/mL after 4.5 months. Men with testosterone use < 1>
Eugondaotrophic hypogonadism: It is characterized by severe oligospermia, low serum testosterone levels and abnormally low serum testosterone/estradiol ratio. Aromataze inhibitor named Testolactone 50-100 mg twice daily or anastozole 1 mg daily is advised. [4,5,6]
Hypergonadotrohpic hypogonadism: No use of medical management. Preliminary genetic evaluation is advised. For men with complete spermatogenesis failure, only treatment option is insemination with donor sperms or adoption. [4,6,7,15]
In patients with retrograde ejaculation, Alpha agonist increasing bladder sympathetic tone, Anti-cholinergics inhibiting para-sympathetic stimulation are recommended. Imipramine is most commonly used. As second line of management, penile electro-vibration and recovery of sperms from buffered urine can be attempted. Success rate of medical therapy for retrograde ejaculation is 50% while that for anejaculation is poor. Surgical sperm retrieval is the final resort if these modalities fail. [3,6,15,16]
In Leucocytospermia with Leukocytes>1 × 106/ml of semen, send semen for culture and sensitivity testing and treat accordingly particularly if it is associated with identified infection. [4,15,16]
There is no proven medical treatment for idiopathic male infertility. Androgen therapy may be advised for stimulating spermatogenesis. Use of exogeneous FSH has conflicting results. Empirical treatment with either clomiphene citrate (25 mg daily 3-6 months) or tamoxifen (20 mg daily) are commonly offered to stimulate increased pituitary gonadotrophin secretion and spermatogenesis.3,4,15
Surgical options
Reconstructive surgery-Corrective surgical procedures including vasovasostomy and vasoepididymostomy are preferred over surgical sperm retrieval for vasectomy reversal given better pregnancy outcomes and cost benefits. Usually, pregnancy happens 24 months after reversal. Reversal results are predisposed by vasectomy site, interval between vasectomy and reversal and surgeon expertise. Within 3 years high patency rates upto 97percent and 75percentpregnancy rates have been reported while corresponding figures drop to 80percent and 55percentafter 3 years.3,4 Consider ART in couples who fail to conceive 12-18 months following vasectomy reversal. Though antisperm antibodies are seen in 60percent patients, they donot affect fecundability. Periodic semen analysis can identify re-obstruction in 3percent to 21percent cases post-surgery, depending on which segment were re-anastomosed.5,15 In cases with persistent azoospermia for 6 months post reversal, ICSI is preferred over repeat surgical reversal as the patency rates drop to 75percent and pregnancy rates fall to 43percent. consider ICSI.4 Favourable outcomes are less reported in cases with infections leading to obstruction. In such cases, cryopreservation of sperms for ART is recommended to alleviate the need of future surgical procedures. Such situations demand sperm cryopreservation for use in ART in order to reduce need for additional surgeries.3,17 Reconstructive surgery in CABVD is not indicated as major portion of vas deferens is developmentally lacking, making SSR the only viable option for this condition. [15,17]
Surgical Sperm Retrieval
The term refers to a group of surgical procedures used to give azoospermic men the opportunity to become biological fathers by obtaining sperm via ICSI.18The indications for SSR are as follow-
• To provide sperms for ICSI in azoospermic men.
• In obstructive azoospermia, by recovering sperms from epididymis. Percutaneous procedures have high success rates of 95-100percent
• In non-obstructive and idiopathic azoospermia, sperms are retrieved from testis directly. The success rate of SSR is 45-55percent4,15,17,18
Sperms obtained are managed by fresh approach or frozen approach. In fresh approach, SSR is planned along with oocyte retrieval. In frozen approach, SSR is scheduled before ICSI treatment with aim to cryopreserve sperms and to be used at later date. Both methods report similar fertilization and pregnancy rates. Frozen approach is preferred particularly in non-obstructive azoospermia. Repeat SSR is advised after 3-6 months to allow adequate healing. [3,4,18]
SSR procedures 4,17
Open surgical procedures:requires operating microscope and General or regional anaesthesia
Microsurgical epididymal sperm aspiration (MESA)Testicular sperm extraction (TESE)
Percutaneous procedures: requires local anaesthesia.Percutaneous epidydimal sperm aspiration (PESA)Percutaneous sperm fine needle aspiration (TESA), also known as fine needle aspiration (FNA)
These procedures are diagrammatically depicted in Figure 1.
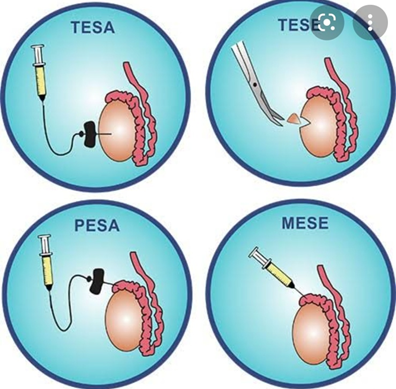
Figure 1: Surgical Sperm Retrieval procedures.
Augments to ICSI
Failed fertilization occurs in 2-5% of ICSI cycles.19A sperm-specific protein is injected into oocyte during early stages of fertilisation process. This causes intracellular Ca+2 oscillations within oocyte, leading to its activation. Based on this theory, calcium ionophores have been used in lab conditions to enhance fertilization by artificially facilitating oocyte activation in PLC zeta deficiency sperm. In asthenozoospermic patients, improved sperm motility with theophylline or pentoxifylline treatment has been shown to improve implantation, fertilisation and clinical pregnancy rates. [3,19]
Donor Sperm
Using donor sperms is usually a difficult decision for the couple. They are advised for azoospermic men with failed corrective surgery/SSR, for patients with Severe sexual or ejaculatory dysfunction refractory to medical treatment, in cases with severe azoospermia with recurrent fertilisation failure or poor embryo development, when there is risk of inheriting genetic anomaly through male gamete or because of financial implications of assisted reproduction. [3,4,20]
Sperm donors are rigorously screened for STDs and genetic conditions. Before employing the sperms for any treatment, semen sample is quarantined for minimum six months if serology has been the only testing method employed, or at least for three months if nucleic acid amplification testing has been carried out in addition to serology testing. [3,4,19,20]
Proper treatment and counselling of patient and the couple are must in addition to good clinical practice before, during and after ART in cases of male infertility. The goal is informing the patient related risks, improving success rate of ART treatment and avoiding birth of children with severe genetic disease.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
