
Review Article | DOI: https://doi.org/10.31579/2641-0419/043
*Corresponding Author: Maria Luz Gunturiz A., Public Health Research Division, National Institute of Health. Avenue Street 26 No 51-20 CAN, Bogotá, D.C., Colombia.
Citation: Maria Luz Gunturiz A. (2020) Main cardiovascular manifestations induced by coronaviruses: about the new virus 2019-CoV. Journal of Clinical Cardiology and Cardiovascular Interventions, 3(6): Doi: 10.31579/2641-0419/043
Copyright: © 2020 Maria Luz Gunturiz A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 March 2020 | Accepted: 01 April 2020 | Published: 06 April 2020
Keywords: Coronavirus, cardiovascular disease, respiratory infections, cardiovascular complications.
Chronic diseases are the cause of the highest mortality worldwide. Its prevalence is increasing, especially in middle- and low-income countries, in populations with a longer life expectancy that have adopted, among others, healthier lifestyles and diets. On the other hand, there are no therapeutic strategies focused exclusively on this population when they occur. respiratory virus epidemics such as coronaviruses.
This review presents evidence that shows the main cardiovascular manifestations associated with infection by respiratory viruses and especially by coronaviruses.
The epidemics of severe acute respiratory infections (IRAG) are a threat to global health, with significant morbidity and mortality rates, over the past two decades.
Coronaviruses are enveloped nonsegmented positive-sense RNA viruses that belong to the Coronaviridae family. and the order Nidovirales. It has been described that they are distributed broadly among humans, other mammals, and birds and that cause respiratory, enteric, hepatic, and neurologic diseases [1-3].
Six coronavirus species are known to cause human disease: four viruses (229E, OC43, NL63, and HKU1) are prevalent and typically cause common cold symptoms in immunocompetent individuals [4, 5]. The two other strains, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV) are zoonotic in origin and have been linked to sometimes fatal illness [5, 6].
SARS-CoV was the causal agent of the severe acute respiratory syndrome outbreaks in 2002 and 2003 in Guangdong Province, China [7-9] and MERS-CoV was the pathogen responsible for severe respiratory disease outbreaks in 2012 in the Middle East [10].
Coronavirus infections are generally mild, but two epidemics caused by coronavirus have been reported: SARS-CoV was the causal agent of the severe acute respiratory syndrome outbreaks in 2002 and 2003 in Guangdong Province, China [1, 7-9, 11] and the MERS-CoV that was the pathogen responsible for severe respiratory disease outbreaks in 2012 in the Middle East [10, 12] that caused more than 10,000 cases, with 10% mortality rates for SARS-CoV and 37% for MERS-CoV [1,13,14].
Given the high prevalence and wide distribution of coronaviruses, the large genetic diversity and frequent recombination of their genomes, and increasing human–animal interface activities, novel coronaviruses are likely to emerge periodically in humans owing to frequent cross-species infections and occasional spillover events [1,6,15].
In December 2019, some cases of pneumonia caused by a new coronavirus, called 2019-CoV or Wuhan coronavirus, were reported for the first time because it is this city where the first cases were detected [14].
In the last decade, in addition to epidemics caused by other respiratory viruses, three major epidemic outbreaks caused by coronaviruses have been described.
The first one, caused by the SARS-CoV that caused a severe respiratory syndrome known as SARS (Severe Acute Respiratory Syndrome) that appeared in 2002 in China, and affected more than 8,000 people in 30 countries and caused 700 deaths with a mortality rate of 10.6%) [7].
In 2012, the MERS-CoV that causes the Middle East respiratory syndrome, which is why it was called MERS (Middle East Respiratory Syndrome) with more than 2400 cases detected and more than 800 deaths in 26 countries, reaching a mortality of 35%, although the vast majority of reported cases originated in the Arabian Peninsula [10, 16,-18].
The recently described in Wuhan, known as 2019-CoV that has animal origin, has been transmitted to man, and from person to person, with more than 134.000 cases (on March 12, 2020) and an approximate mortality of 7%, since its appearance 3 months ago [1, 19-21].
Because of its importance, it is worth mentioning the Influenza A (H1N1) virus that has been classified as a public health problem for humans. Since the 2009 pandemic, H1N1 flu has caused approximately 284,500 deaths, directly from respiratory infections and indirectly from secondary cardiovascular diseases associated with bacterial infections [22-25].
Main symptoms and clinical manifestations in new coronavirus infection
All these viruses are directed to the respiratory tract and share many similar clinical symptoms, the most common being fever, cough, dyspnea, myalgia or fatigue, shortness of breath and sore throat always followed by gastrointestinal symptoms such as nausea, vomiting and diarrhea [22-26-28]. These respiratory diseases often present complications such as pneumonia, acute respiratory distress syndrome, organ failure and even death and mainly affect the respiratory system with organ failure, followed by the renal and cardiovascular systems [24, 25].
It is estimated that the infection has an incubation period of 2 to 14 days with potential for asymptomatic transmission, unlike the involvement of SARS. Due to clinical manifestations, it may be like other viral infections such as influenza and deceased patients have presented severe pulmonary diseases such as pneumonia with respiratory failure. However, other symptoms and complications related to infection with this coronavirus are still unknown, as well as the involvement of organs and tissues other than those of the respiratory system [1, 19-21].
The new coronavirus affects men, women, and children just as often. However, the consequences are very different, depending on age, sex and previous illnesses.
With the new coronavirus, the elderly is most at risk. The mortality rate increases exponentially from the age of 65, approximately. In China, for example, the mortality rate of infected people who are up to 40 years old is 0.2%, but among those who are 70 and 79 years old, it increases to 8%, while from the 80s years, increases to 14.8% [1, 19].
Instead, people between 21 years and 50 years are mainly infected with H1N1 with an average age of 40 years [23-25].
Involvement of coronaviruses with cardiovascular complications
To date, there are no studies that report the presence of cardiovascular complications caused by coronaviruses in general, nor by 2019-nCoV specifically. Huang et al [1] reported 12% of acute heart involvement in 41 patients with a confirmed diagnosis of Wuhan coronavirus infection, all hospitalized with pneumonia, one third of whom were admitted to the intensive care unit. Cardiac involvement was diagnosed if new electrocardiographic or echocardiographic abnormalities were present and all of them presented troponin elevation. All patients were treated with antibiotics, antivirals, corticosteroids and according to their evolution invasive mechanical ventilation.
Most of the available information on cardiac involvement due to coronavirus comes primarily from reports of isolated cases of other coronaviruses, Yu et al [29], published a study evaluating cardiovascular complications based on clinical and radiological detection in 121 cases of SARS, without systematically using the electrocardiogram, echocardiogram, Holter or other cardiovascular examinations, so there could be a underreporting of the cardiovascular condition [29-31].
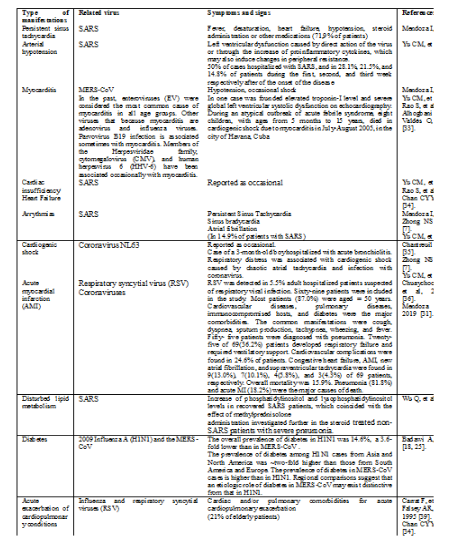
According to all these reports, the main cardiovascular manifestations induced by coronaviruses, respiratory and syncytial viruses are persistent sinus tachycardia, myocarditis, hypotension, cardiac insufficiency, arrythmias, cardiogenic shock and acute infarct of the myocardium.
The table 1 summarizes the main symptoms and signs at the cardiovascular level as a result of virus infection.
Although SARS-CoV survivors benefited from clinical treatments that targeted the virus and inflammation, the recovered patients in the current study continued to experience a poor quality of life 12 years after their infections. Patients had experienced various diseases, including lung susceptibility to infections, tumors, cardiovascular disorders, and abnormal glucose metabolism. As compared to healthy controls, metabolomic analyses identified significant differences in the serum metabolomes of SARS survivors [37].
Respiratory virus (RV) infections have been implicated in acute exacerbation of cardiopulmonary conditions. Influenza and respiratory syncytial viruses (RSV) were diagnosed in 21% of elderly patients with underlying cardiac and/or pulmonary comorbidities hospitalized for acute cardiopulmonary exacerbations [34, 38-40].
Coronavirus infection of the Middle East respiratory syndrome (MERS-CoV) is associated with serious life-threatening diseases and reports a mortality rate of approximately 35%, particularly in patients with underlying comorbidities. A systematic analysis of 637 cases of MERS-CoV suggests that diabetes and hypertension are equally prevalent in approximately 50% of patients. Heart disease is present in 30% and obesity in 16% of cases. These conditions regulate the synthesis of proinflammatory cytokines and impair the host's innate and humoral immune systems. In conclusion, protection against MERS-CoV and other respiratory infections can be improved if public health vaccination strategies are adapted to target people with chronic disorders [18, 25].
In a recent study, it was observed that, compared with subjects without comorbidities, severe pandemic influenza occurred significantly more frequently in those individuals who were obese and in those who suffered from cardiovascular disease, hypertension and neuromuscular diseases. It has also been observed that chronic conditions that influence the severity of MERS-CoV such as diabetes, hypertension, obesity and cardiovascular disease / coronary artery disease, have similar effects on other respiratory diseases such as influenza and influenza A H1N1. In contrast, the prevalence of comorbidities such as immunodeficiency and HIV has been low in severe cases of MERS-CoV compared, for example, with their rates in severe cases of influenza A H1N1 [18, 25].
Pathologies related to the metabolic syndrome, such as diabetes, hypertension, CAD/ CVD and obesity, together with their predisposing conditions, can be etiologically implicated to the pathogenesis of MERS-CoV. It has been described that these disorders negatively regulate the key mediators of the host's innate immune response to pathogenesis. Specifically, diabetes, hyperglycemia and insulinopenia attenuate the synthesis of proinflammatory cytokines such as gamma interferon (IFN-γ) and interleukins (IL) to functionally affect the innate and humoral immune systems of the host. Chronic diseases share several common characteristics with infectious disorders and their complications, such as endothelial dysfunction, proinflammatory status and attenuation of the innate immune response [18, 25, 41-44]. Cytokine overload related to the change from Th1 to Th2 in severe viral infection when accompanied by cytokine synthesis that arises from metabolic diseases, can be detrimental to the endothelium and lead to a series of subsequent complications [18, 25, 42]. The potential role of altered innate immunity and the change in the Th1 response for microbicidal action of IFN-γ to Th2 (IL-4, -5, -10 and -13 anti-inflammatory) in relating metabolic diseases with severe viral presentation may also be supported by the high prevalence of allergy observed in fatal viral infections and eosinophilic responses in other infections [45, 46]. In addition, metabolic disorders impair macrophage and lymphocyte functions with a subsequent reduced immune response status, which can make individuals more susceptible to complications of infectious diseases. Additionally, glycosylated hemoglobin levels (HbA1c) ≥ 9% have been associated with a 60% increase in the risk of hospitalization and severity related to pneumonia [47, 48] with a variation in OR for severe MERS-CoV between 7.2 and 15.7 in diabetic subjects [26-28, 49, 50].
Diabetes is one of the known documented contributing host-related risk factors in both H1N1 and MERS-CoV severe cases and associated with RV infections in general and is frequent in individuals developing fatal disease complications [23, 24, 27, 28, 25, 51]. This data may suggest an etiological relationship between diabetes and acute viral respiratory infections, as its related conditions downregulate the innate and humoral immune systems by reducing the function of T cells and neutrophils. On the other hand, hyperglycemia impairs critical components of innate immunity in vitro, such as chemotaxis, phagocytosis, and the bactericidal activity of neutrophils and macrophages and lead to secondary infections [25, 52-54].
The direct influence of diabetes or other cardiovascular and metabolic diseases, on acute respiratory infections still needs more research to estimate the frequency in severe viral conditions and to clarify the etiologic role in disease severity [25, 54].
Main clinical features of patients infected with 2019-nCoV
Huang C et al reported that 41 patients admitted to the hospital in January were confirmed as positive for 2019-nCoV. These authors mentioned that most of the infected patients were men (30/41 [73%]); less than half had underlying diseases (13 [32%]), including diabetes (8 [20%]), hypertension (6 [15%]), and cardiovascular disease (6 [15%]). The median age was 49.0 years. Common symptoms at disease onset were fever (40/41 [98%]), cough (31 [76%]), and myalgia or fatigue (18 [44%]); less common symptoms were sputum production (11/39 [28%]), headache (3/38 [8%]), hemoptysis (2/39 [5%]), and diarrhea (1/38 [3%]). Dyspnea developed in 22 (55%) of 40 patients (mean time from disease onset to dyspnea 8 · 0 days ). 26 (63%) of 41 patients had lymphopenia. All 41 patients had pneumonia with abnormal findings on chest CT. Complications included acute respiratory distress syndrome (12 [29%]), ARNaemia (six [15%]), acute heart damage (5 [12%]), and secondary infection (4 [10%]). 13 (32%) patients were admitted to an ICU and six (15%) died. Compared with non-ICU patients, ICU patients had higher plasma levels of IL2, IL7, IL10, GSCF, IP10, MCP1, MIP1A, and TNFα. [1].
On the other hand, Yang J et al carried out a meta-analysis study to assess the prevalence of comorbidities in the 2019-nCoV infection patients and the risk of underlying diseases in severe patients compared to non-severe patients [55].
They reported, "Eight studies were included in the meta-analysis, including 46248 infected patients. The result showed the most prevalent clinical symptom was fever (91 ± 3, 95% CI 86-97%), followed by cough (67 ± 7 , 95% CI 59-76%), fatigue (51 ± 0, 95% CI 34-68%) and dyspnea (30 ± 4, 95% CI 21-40%). The most prevalent comorbidity were hypertension (17 ± 7, 95% CI 14-22%) and diabetes (8 ± 6, 95% CI 6-11%), followed by cardiovascular diseases (5 ± 4, 95% CI 4-7%) and respiratory system disease (2 ± 0 , 95% CI 1-3%). Compared with the non-severe patient, the pooled odds ratio of hypertension, respiratory system disease, cardiovascular disease in severe patients were (OR 2.36, 95% CI: 1.46-3.83), (OR 2.46, 95% CI: 1.76-3.44) and (OR 3.42, 95% CI: 1.88-6.22) respectively " [55].
Use of Angiotensin-Converting Enzyme Inhibitors (ACEI) or Angiotensin Receptor Blockers (ARBs) in Infection with 2019-nCoV
According to initial reports from China, and subsequent evidence that high blood pressure may be associated with an increased risk of mortality in hospitalized subjects infected with 2019-nCoV, hypotheses have been put forward suggesting possible adverse effects of ACEI or ARBs. It has been especially suggested that these commonly used drugs may increase both the risk of infection and the severity of SARS-CoV2 or 2019-nCoV [56, 57].
The concern of patients using these drugs and their treating doctors arises from the observation that, similar to the coronavirus that causes SARS, the 2019-nCoV virus binds to a specific enzyme called ACE2 to infect cells, and ACE2 levels increase after treatment with ACEI and ARB [56-58].
Speculation about the safety of ACEI or ARB treatment in relation to 2019-nCoV does not have a strong scientific basis or supporting evidence. In fact, there is evidence from animal studies that these drugs may be quite protective against serious lung complications in patients with 2019-nCoV infection, but to date there are no human data [56-60].
Other studies have suggested that ACE-1 inhibitors, such as enalapril and ramipril, and angiotensin receptor antagonists ARB, such as candesartan and valsartan, may be effective in preventing and treating the effects of the 2019-nCoV coronavirus [56].
Recently, three clinical trials using ACEI treatment have been recorded. The first one aims to know the clinical differences between patients with hypertension with and without ACEI treatment when they suffered with the 2019-nCoV infections in China. The second of them supports the use of the recombinant human angiotensin converting enzyme 2 (rhACE2) as a treatment for patients with COVID-19 and the third corresponds to a clinical study to evaluate the effects of ACEI/BRA on the infection of new pneumonia by coronavirus (2019-nCoV) [56].
But what are the 2019-nCoV mechanisms to infect cells?
As indicated above, coronaviruses are single-stranded RNA viruses, approximately 120 nanometers in diameter, made up of surface glycoproteins that allow coronaviruses to enter host cells. These glycoproteins also give it that characteristic corona structure of these viruses.
These glycoproteins have two subunits; S1 that binds to receptors on the cell surface; and S2, which fuses with the cell membrane. In the host, a transmembrane serine protease (TMPRSS2), promotes the entry of SARS-Cov into cells by two separate mechanisms. After the S1 subunit binds to the ACE-2 enzyme on the cell membrane surface, TMPRSS2 activates glycoproteins and cleaves ACE-2. Likewise, TMPRSS2 also acts on the S2 subunit causing an irreversible conformational change, activating it and facilitating the fusion of the virus to the cell membrane, with which the virus enters the cell [56, 57].
Both the SARS-CoV-1 and SARS-CoV-2 viruses (with an approximate structural identity of 80%), enter the host cells taking advantage of the action of the angiotensin-converting enzyme, ACE-2, which is expressed in the membranes of many cells in the body, including pulmonary alveolar epithelial cells.
Accordingly, reducing ACE-2 activity in cell membranes could theoretically reduce the ability of SARS-CoV-2 to penetrate cells. However, ACEI, such as enalapril and ramipril, used to treat hypertension and heart failure, do not inhibit ACE-2 [56-58].
It is well described that ACE inhibition increases the concentration of circulating angiotensin I, which could be converted to angiotensin [56].
The presence of a higher amount of angiotensin I, due to ACE-1 inhibition, could tend to up regulate ACE-2. Moreover, in experimental animals, ACE-1 inhibitors and ARBs increase cardiac ACE-2 activity and it is unclear whether such up regulation would be appropriate or not. Increased production of angiotensin from angiotensin II under the action of ACE-2, despite reduced production of angiotensin could lead to increased anti-inflammatory activity, partly mediated by inhibition of COX-2 synthesis, and some protection against lung damage caused by the virus. However, since ACE inhibitors lower angiotensin II concentrations, it is unlikely to be a large effect. Moreover, increased anti-inflammatory activity (by administration of an NSAID or corticosteroids), may not be advantageous and could be harmful in virus infections [56, 59].
So what to do with patients suffering from high blood pressure and chronic heart disease and COVID-19 infection?
It is relevant to mention that patients with severe hypertension or chronic heart failure can worsen rapidly if the drugs that act on the renin-angiotensin system are discontinued, so it is recommended that patients who are taking ACE-1 inhibitors or ARB continue taking their medications and following the instructions of the American College of Cardiology who have stated that "in the event that patients with cardiovascular disease are diagnosed with 2019-nCoV, individualized treatment decisions should be made according to hemodynamic status and clinical presentation of each patient". On the other hand, the Hypertension Council of the European Society of Cardiology has described that there is still insufficient evidence to support a harmful effect of ACE-1 inhibitors and ARBs in the context of the pandemic outbreak of 2019-nCoV; and it is not possible to indicate that the expected benefits are greater than the potential harm in infected patients, therefore it is not prudent to institute any pharmacological therapy based on an unproven hypothesis [56-60].
It is necessary to wait for the results of the clinical studies that are being carried out, in order to have scientific evidence that can suggest whether or not to use conventional ACE-1 or ARB inhibitors to treat 2019-nCoV.
At the cardiac level, pre-existing conditions such as ischemic heart disease, hypertension, diabetes mellitus, hyperlipidemia, obesity and cardiac arrhythmias, among others, increase the complications and prevalence of infections caused by viruses and there is still ignorance about the medium and long-term effects of these respiratory infections in patients with the aforementioned pathologies and about which other organs and tissues besides the lungs and upper respiratory tract are being colonized the new coronavirus 2019-nCoV .
To date, it is unknown if there are more than two circulating coronaviruses in the countries affected by this epidemic, making therapeutic strategies, including the development of vaccines, more difficult, making it necessary to strengthen prevention measures and to have available Rapid, precise and specific diagnostic tests that allow confirming cases in a very short time, avoiding massive contagion of the population.
Finally, it is important to mention that in times where dengue serotypes, H1N1 and other seasonal influences circulate, as well as other respiratory viruses, with symptoms similar to those of the new coronavirus, it may be possible that their detection is underestimated or masked by these diseases, therefore surveillance of this event must be intensified and patients with cardiovascular diseases monitored.
Data from the start of the pandemic allow to infer that indeed patients with diabetes, high blood pressure and cardiovascular disease have a very high risk of having serious complications if they become infected with the 2019-nCoV, so a very rigorous clinical follow-up must be done to prevent die from such complications.
The author wishes to acknowledge the financial support provided by the National Institute of Health of Colombia.
The following abbreviations are used in this manuscript
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
