
Research Article | DOI: https://doi.org/10.31579/2768-2757/085
1 Emergency Department, UKRIDA Hospital, Jakarta, Indonesia, 11510.
2 Department of Internal Medicine, UKRIDA Hospital, Jakarta, Indonesia, 11510.
3 Department of Surgery, UKRIDA Hospital, Jakarta, Indonesia, 11510.
*Corresponding Author: Geresu Gebeyehu, Addis Ababa University, Addis Ababa, Ethiopia.
Citation: Geresu Gebeyehu, Gutu Leta, Selamawit shiferaw, (2023), Magnitude and Associated Factors of Intraoperative Hyperglycemia among Orthopedics Surgical Patients. A Cross-Sectional Study, Journal of Clinical Surgery and Research, 4(4); DOI:10.31579/2768-2757/085
Copyright: 2023, Geresu Gebeyehu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2023 | Accepted: 24 June 2023 | Published: 04 July 2023
Keywords: magnitude; intraoperative hyperglycemia; orthopedic surgery; associated factors
Background: Intraoperative hyperglycemia is a common problem among patients undergoing orthopedic surgery. Its incidence varies from country to country and not clearly studied in developing countries.
Method: Multi-center cross-sectional study was conducted on eligible adult elective patients who underwent orthopedic surgical procedures. The participants were selected using a systematic random sampling technique. Data was collected on basic characteristics, medical and surgical history. On the arrival of patients to the OR, blood glucose was measured and recorded and repeated after administering anesthesia. The data was analyzed using descriptive statistics and bivariate and multivariate logistic regression. P<0.05 was considered as statistically significant.
Results: Intraoperative hyperglycemia was observed in 20.4% of patients. Hypothermia (AOR:2.45;95% CI:0.97-6.27, p=0.05), infused dextrose iv fluids (AOR:2.94;95% CI:1.64-5.16, p=0.05), blood transfusion (AOR:6.64;95% CI:2.92-15.08, p=0.00) and history of hypertension (AOR:2.19;95% CI:1.23-3.71, p=0.01) were factors identified to be associated with intraoperative hyperglycemia.
Conclusions: This study showed the magnitude of intraoperative hyperglycemia was high. Anesthetists should identify all risk factors preoperatively and make appropriate adjustments for patient care. Hypertension should be optimized, refrain from routine administering of dextrose IV fluids, and unnecessary transfusions, as well as monitor patients’ body temperature.
The number of orthopedic surgical approaches is growing in older individual in whom the magnitude of diabetic disease is dramatically alarming currently [1]. Acute hyperglycemia, which occurs after traumatic injury, has also obtained a lot of attention; because trauma induces the release of stress hormone, mostly mediated by glucagon, leading to an increase in oxidative stress and insulin resistance, finally hyperglycemia occurs [2]. It was well known that poor perioperative glycemic management were associated with negative outcomes encompassing impaired wound healing, hardware or implant failure, extended threat of surgical site infections, and pseudarthrosis for the duration of orthopedic surgical procedures [3]. The American Diabetes Association estimates that 12–25% of hospitalized personnel have diabetes mellitus (DM). With the growing occurrence of diabetic suffererspresentingfor surgical process and the elevated threat of headaches related to diabetes mellitus, suitable perioperative evaluation and control are imperative [4]. It wasreported that 10 to 20% of orthopedic surgery patients were diagnosed with diabetes. Corsino and colleagues in their study reported that 22 to 46% of non-critically ill patients faced hyperglycemia with or without a history of diabetes and Umpierrez et al. also estimated hyperglycemia in 32 to 38% of hospitalized individuals in community health facilities [5, 6]. Kwon et al reported that non-diabetic patients who encountered perioperative hyperglycemia had nearly twice the risk of infection, reoperative intervention, and in-hospital death when compared with known diabetic patients [7]. Another study conducted by Meltem T. et al. reported that in-hospital hyperglycemia is an important clinical indicator, carrying a higher 1- and 5-year mortality risk than those who have previous history of diabetes [8]. It was reported in the past that transient hyperglycemia among patients in critical condition is without adverse outcome, even imagining that it is beneficial; but several studies showed that there is clear mortality and morbidity advantages from strict glycemic control of glucose level with insulin therapy in critically sick ICU individuals without considering diabetic or non-diabetic status of the patients [9]. Reports came out by Gerard M. et al speculating that the health professionals’ attitude to screen out, monitor, and follow perioperative blood glucose, and start therapy for hyperglycemia is not much enough and neglected unless subject has history of diabetes mellitus [10]. Even though, the number of individuals requiring advanced technologies and procedures are increasing in orthopedics unit [11] but, evidence regarding magnitude and associated factors of intraoperative hyperglycemia for adult patients who underwent orthopedic surgery does not exist in developing nations including our country Ethiopia. This study was aimed at determining the magnitude and associated factors of hyperglycemia in elective non-diabetic adult orthopedic patients in public tertiary hospitals in Ethiopia.
1.1 conceptual framework
The conceptual framework prepared based on the literatures reviewed for the evidences in this study. (Figure. 1)
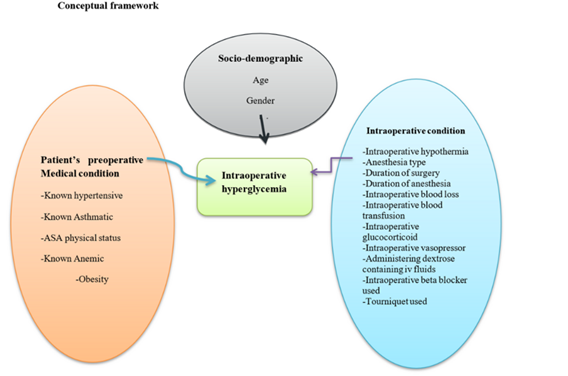
Figure 1: Conceptual framework indicating factors affecting intraoperative hyperglycemia for adult patients undergoing elective orthopedic surgical procedures at tertiary hospitals, Addis Ababa, Ethiopia2022.
2.1 Study design and setting, period, and population
A multicenter cross-sectional study was conducted at selected public hospitals in Addis Ababa from January 01 to April 01, 2022. The source population was all adult orthopedic surgical patients admitted to public hospitals in Addis Ababa. The study population was all eligible adult orthopedic surgical patients during the study period. All ASA I and II, and aged above 18 years old were included into this study. Patients with a history of diabetes mellitus, confirmed pregnancy and taking steroid therapy were excluded.
2.2 Sample size determination
The sample size was determined using the single population proportion for the first objective, which is the magnitude of intraoperative hyperglycemia in non-diabetic adult patients who underwent elective orthopedic surgical procedures. Since there was no related study conducted in the study area, we used P = 0.5 for calculation to get the maximum sample size, 95% level of significance, 5% margin of error, and 10% for incomplete or as contingency data will be used as parameters.
n = 384
By using correction, the formula for finite population, since source populations were less than 10,000
nf = n/ (1 + n/N), N = 506…. Correction formula for population less than 10,000.
Nf = n/1 + n/N = 384/ (1 + 384/506) = 218. By Adding 10% contingency for non-response rate(i.e., 218 + 22 = 240). As a result, a total of 240 adult major elective orthopedic surgery patients were included in this study.
Nf = Final sample size,
n = sample size,
N = total number of adult patients who underwent elective orthopedic surgery
2.3 Sampling techniques and procedures
Systematic random sampling technique was used. The study settings have been selected randomly from Addis Ababa governmental city hospitals. We included every second adult patient underwent elective orthopedics surgery during the study period. Patients’ capillary blood glucose was measured immediately after the patient arrived the operation theater and then continued from induction of anesthesia and every hour up to the end of the surgery.
2.4 Operational Definitions
Preoperative
The time that extends from the decision to have surgery to induction of anesthesia [12].
Intraoperative
The period that extends from induction of anesthesia until the patient is transported to PACU [13].
Perioperative
the period comprises all three periods (preoperative, intraoperative and postoperative) [6].
Hypothermia
Core body temperature below 36 degrees Celsius [14].
MINS (Myocardial injury in non-diabetic surgery): Factors unique to hyperglycemia conditions that increase atherosclerotic plaque formation and thrombosis, thereby contributing to myocardial infarction [15].
SIH (Stress induced hyperglycemia): Stress hyperglycemia or hospital-related hyperglycemia as any blood glucose concentration > 7.8 mmol/l (140 mg/dl) without evidence of previous diabetes [16].
2.5 Data collection tool and procedures
Data was gatheredusingpretested questionnaires. Training was provided for all data collectors on data collection procedures in each of the study settings. The data collection tool included socio-demographic, medical history and intraoperative clinicalconditions and anesthetic agents. Sociodemographic and medical history were obtained from the patients charts on the immediate arrival of patients into the OR, and regarding intraoperative blood glucose, and anesthetic and surgical dataduring the intraoperative period were recorded from anesthesia charts during anesthetic induction and every one-hour interval until surgery ends.
2.6 Data quality control
To assure the quality of data, training on the objectives and relevance of the study and brief orientations on the assessment tools were provided for data collectors. The questionnaires were pretested on 5% of the study population at ALERT hospital.
2.7 Data processing and analysis
The collected data was coded, cleaned, retrieved, and entered in to SPSS for analysis. Descriptive statistics were used to analyze sociodemographic characteristics. Bivariate and multivariable regression analysis were performed to assess the association between dependent and independent variables.Odds ratios with 95% CI were used to determine the degree of association between dependent and independent variables. In multivariable regression analysis, variables with a p-valueof < 0.05 were considered as statistically significant. The results were presented using words, tables, and figures.
3.1 Socio-demographic characteristics of study participants
240 elective major orthopedic adult patients were included in the study with a 100% response rate. (Table 1)
| Variables | Category | Frequency | Percentage (%) | |
|---|---|---|---|---|
| Gender | Male | 196 | 81.7 | |
| Female | 44 | 18.3 | ||
| Age | 18–40 | 178 | 74.2 | |
| 41–60 | 51 | 21.3 | ||
| > 60 | 11 | 4.6 | ||
| ASA status | ASA I | 190 | 79.2 | |
| ASA II | 39 | 16.3 | ||
| ASA III | 11 | 4.6 | ||
| BMI | < 18.5 | 30 | 12.3 | |
| 18.5–24.9 | 193 | 80.4 | ||
| 25-29.9 | 12 | 5.0 | ||
| > 30 | 5 | 2.1 | ||
| Co-existing diseases | History of Hypertension | Yes | 21 | 8.8 |
| No | 219 | 92.2 | ||
| History of Anemia | Yes | 56 | 23.3 | |
| No | 184 | 76.7 | ||
| History of sepsis | Yes | 36 | 15.0 | |
| No | 204 | 85.0 | ||
Table 1: Socio-demographic and preoperative clinical characteristics of elective orthopedics surgery patients at tertiary public hospitals, Addis Ababa, Ethiopia 2022.
3.2 Anesthetic and surgical characteristics of patients
Intraoperative anesthetic and surgical characteristics were analyzed and the findings were presented below. (Table 2)
| Variables | Category | Frequency | Percentage (%) |
|---|---|---|---|
| Anesthesia type | General | 32 | 13.3 |
| Spinal | 183 | 76.3 | |
| Combined | 15 | 10.4 | |
| Surgery time | ≤ 60min | 38 | 15.9 |
| > 60 min | 202 | 84.1 | |
| Tourniquet used | Yes | 24 | 10.0 |
| No | 216 | 90.0 | |
| Steroids used | Yes | 41 | 17.1 |
| No | 11 | 4.6 | |
| Vasopressors used | Yes | 29 | 12.1 |
| No | 13 | 5.4 | |
| Dextrose IV fluids | Yes | 29 | 12.1 |
| No | 211 | 87.9 | |
| Blood transfusion | Yes | 31 | 12.9 |
| No | 209 | 87.1 | |
| Blood loss | ≤ 300ml | 138 | 57.5 |
| > 300ml | 102 | 42.5 | |
| Hypothermia | Yes | 22 | 9.2 |
| No | 218 | 90.8 |
Table 2: Anesthetic and surgical characteristics of elective orthopedics surgery patients at tertiary public hospitals, Addis Ababa, Ethiopia2022.
3.3 Magnitude of Intraoperative hyperglycemia in patients undergoing orthopedics surgery
Intra-operative hyperglycemia report was displayed below. (Figure. 2)

Figure 2: the magnitude of intraoperative hyperglycemia in orthopedic surgical patients at public hospitals, Addis Ababa, Ethiopia, 2022.
3.4 Factors associated with Intraoperative hyperglycemia
Both bivariate and multivariate analysis were conducted to determine the association between the outcome variable and the independent variables and the strength of associations and the findings displayed in Table 3.
| Variables | categories | Intraoperative Hyperglycemia | COR,95%CI | AOR,95%CI | P-value | |
| Yes | No | |||||
| Gender | Male | 34 | 162 | 0.40;0.23–0.89 | 0.42;0.20-.84 | 0.54 |
| Female | 15 | 29 | I | |||
| Age | 18–40 | 32 | 146 | I | ||
| 41–60 | 16 | 35 | 4.57;0.54–38.18 | 0.48;0.0.24–0.97 | 0.16 | |
| > 60 | 1 | 10 | 0.21;0.03–1.86 | 0.16;0.15-0,17 | 0.17 | |
| ASA status | ASAI | 34 | 163 | 0.10;0.06–0.19 | 0.58;0.15–2.30 | 0.32 |
| ASAII | 12 | 20 | 0.34;0.15–0.78 | 0.49;0.23–1.08 | 0.1 | |
| ASAIII | 3 | 8 | I | |||
| No | 34 | 164 | I | |||
| Anesthesia type | General | 7 | 25 | 3.25;0.25–18.77 | 0.97;0.35–2.69 | 0.188 |
| Spinal | 34 | 149 | 3.68;0.75–18.07 | 1.32;0.67–4.5 | 0.19 | |
| combined | 8 | 17 | I | |||
| History of hypertension | Yes | 12 | 19 | 2.94;1.3–6.60 | 2.19;1.23–3.71 | 0.01** |
| No | 37 | 172 | I | |||
| Preoperative sepsis | Yes | 14 | 22 | 0.19;0.16–0.64 | 2.27;1.36–3.77 | 0.18 |
| No | 35 | 169 | I | |||
| Duration of surgery | ≤ 60 min | 13 | 29 | I | ||
| > 60 min | 36 | 162 | 1.5;0.73–3.09 | 1.70;099-2.92 | 0.28 | |
| Tourniquet used | Yes | 5 | 19 | 2.12;1.23–4.12 | 1.02;.45-2.33 | 0.12 |
| No | 44 | 172 | I | |||
| Dextrose infusion | Yes | 7 | 6 | 5.14;1.64–18.08 | 2.94;1.64–5.16 | 0.05** |
| No | 42 | 185 | I | |||
| Intraoperative hypothermia | Yes | 8 | 14 | 2.47;0.01–0.25 | 2.45;0.97–6.27 | 0.05** |
| No | 41 | 177 | I | |||
| Blood transfusion | Yes | 16 | 13 | 0.32;0.20–0.42 | 6.64;2.92–15.08 | 0.00** |
| No | 33 | 178 | I | |||
| ** = statistically significant, COR = crude odds ratio, CI = confidence interval, AOR = adjusted odds ratio, I = reference | ||||||
Table 3: Associated factors of intraoperative hyperglycemia of elective orthopedics surgery patients at tertiary public hospitals, Addis Ababa, Ethiopia2022.
Hyperglycemia is a common response to intraoperative stress of surgery and critical illnesses, and associated with poor outcomes in critically ill patients regardless of their diabetic status. It has been studied that the degree of rise of blood sugar levels due to surgical stress in controlled diabetics is less significant as compared to non-diabetics [17]. In our study, 20.4% of the study participants that underwent elective orthopedic surgery became hyperglycemic intraoperatively. This result is higher than that of a retrospective cohort study done by Mark P. et al.to evaluate the association between SIH and incident diabetes in survivors of critical illness [18]. Another cross‑sectional observational study done on 536 non-diabetic patients presented to the Intensive Care Unit (ICU) at Gandhi Medical College and allied Hamidia Hospital, Bhopal, between March, 2015, and May, 2015 identified 20.33%of participants developed stress hyperglycemia [19]. The result of our study was supported by the findings of the above study. However, the finding of our study was smaller than the result of the observational study reported by Cornelia K. et al. where they reported 52.9% of intraoperative hyperglycemia out of 87 participants aged 65 years old and above [20]. This may be due to their inclusion of only geriatric patients in their study subjects. An observational prospective study conducted at New Jersey Medical School, University of Medicine and Dentistry of New Jersey, USA, on 295 patients aged 18–80 years undergoing elective non-cardiac surgery reported the findings higher (49%) than the finding of this study [21]. The reason for this difference might be their inclusion of all non -cardiac surgery and hyperglycemia definitions they used (> 126 mg/dl). Furthermore, the magnitude in this study was lower than the findings of a prospective observational study conducted on 191 patients who underwent primary hip and knee replacement, in which 40% of subjects developed hyperglycemia and 48 of them 25% of developed severe hyperglycemia [22]. The possible cause of these variations might be due to the exclusion of known diabetic patients from our study participants. Patients with a history of hypertension were 2.19 times more likely to develop intraoperative hyperglycemia than normotensive individuals. This finding was in line with the Canadian Journal of Cardiology 2018 which stated that patients with hypertension often exhibit insulin resistance and are at greater risk of diabetes developing than are normotensive individuals [23]. Exaggerated catecholamine responseand consequent insulin resistance could be the probable reason for this. In this study, patients who took intraoperative IV infusion of dextrose fluids were 2.94 times more likely to be hyperglycemic. This was supported by the findings of the study conducted by SaringCarinkul and Kotrawera in 2009, which found a progressive increase in blood glucose levels in patients receiving 5
This study found the magnitude of intraoperative hyperglycemia was high. History of hypertension (AOR: 2.19, 95% CI: 1.23–3.71), Intraoperative hypothermia (AOR: 2.45; 95% CI: 0.97–6.27), intraoperative dextrose fluid infusion (AOR = 2.94; 95% CI; 1.64–5.16), Intraoperative blood transfusion (AOR: 6.64, 95% CI: 2.92–15.08) (p = 0.00) were factors identified factors with significant association. The anesthetists and perioperative team should give attention to the identified factors and take necessary remedies to respective factors. This manuscript was prepared from the academic research conducted at Addis Ababa University and deposited in the repository by Gutu Leta and Geresu Gebeyehu in 2022 [26].
Abbreviations
AaBET- Addis Ababa Burn, Emergency and Trauma
ASA- American Society of Anesthesiologists
AMI- Acute Myocardial Infarction
CBG- Capillary Blood Glucose
FMOH- Federal Ministry of Healthy
SIH- stress-induced hyperglycemia
Ethics approval and consent
Ethical clearance was received from Addis Ababa University IRB and Addis Ababa City Administration Health Bureau as well as informed verbal consent was secured from the study participants. Confidentiality was assured throughout the study.
Funding information: Financial support for this study was obtained from Addis Ababa University
Authors' contributions
All authors took part in an inception, design, analysis, interpretation, and drafting of the thesis manuscript. Moreover, all authors read and approved the revised manuscript for publication.
Availability of data and materials
The data will be available from the corresponding author up on reasonable request.
Competing interest: The authors state that there is no competing interest in this work.
Acknowledgments
The authors would like to thank Addis Ababa University for giving an ethical clearance and the study participants for participation. We also thank the study hospitals for accepting to conduct the study. Our special gratitude also goes to the study subjects for accepting and taking consent to conduct this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
