
Case-Report | DOI: https://doi.org/10.31579/2641-0419/106
*Corresponding Author: Saima Karim, DO Metro Health Medical Center 2500 Metro Health Drive Cleveland, OH 44109
Citation: Saima Karim., Roy Arjoon., B. Julie He., Lynda Rosenfeld., Paras Bhatt., (2020) Lyme Carditis Presenting as Sinus Node Dysfunction and Accelerated Junctional Rhythm. J. Clinical Cardiology and Cardiovascular Interventions, 3(12); Doi:10.31579/2641-0419/106
Copyright: © 2020 Saima Karim, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 November 2020 | Accepted: 20 November 2020 | Published: 25 November 2020
Keywords: atrio ventricular; lyme carditis; lyme disease
Lyme disease can have cardiac involvement and can subsequently present with various types of atrio ventricular (AV) block. Sinus node dysfunction (SND) and accelerated junctional rhythm are highlighted in this case as an uncommon presentation for Lyme Carditis. This case highlights the importance of having a high index of suspicion for cardiac involvement with Lyme disease when atypical arrhythmias are present.
Short title: Sinus Node Dysfunction with Lyme Disease
Cardiac involvement in Lyme disease, the most common vector-borne illness in the United States and Europe, usually presents as various degrees of atrioventricular (AV) block (1-3). We present a case of sinus node dysfunction (SND) and accelerated junctional rhythm to emphasize the importance of thinking about this diagnosis in the setting of rhythm disorders other than AV block in appropriate patients.
Case Report:
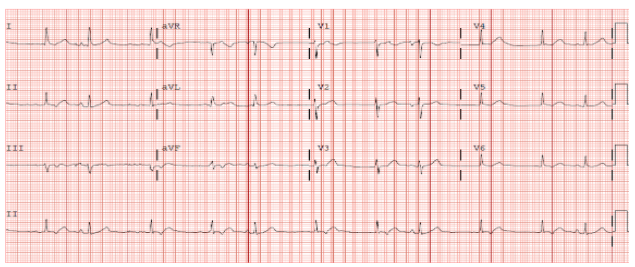
A fifty four year old female with a past medical history of diabetes mellitus, Graves disease treated with tapazole, asthma, hyperlipidemia and obesity presented with the new onset dyspnea on exertion. ECG on presentation showed an accelerated junctional rhythm with retrograde P waves causing enterance block into the sinus node with occasional sinus versus premature atrial complexes with normal AV conduction time (Figure 1).
Cardiac monitoring demonstrated sinus rhythm versus ectopic atrial rhythm followed by a significant pause and then a junctional escape rhythm (Figure 2).

The primary pause was 7.2 seconds with a junctional escape complex, but the overall sinus pause was 10.4 seconds (including the secondary pause of 3.2 seconds).
The patient had gone camping one and half weeks prior to admission. She was not aware of any insect bites but developed progressively worsening dyspnea on walking 100 feet a few days later leading her to present to the Emergency Department. She did describe a rash on her left shoulder and abdomen. She denied any edema, chest pain or lightheadedness.
On presentation, her vital signs were stable with a heart rate of 62 beats per minute. Her physical examination revealed tachypnea, bibasilar rales, an irregular rhythm, and a bullseye rash on her lower abdomen. Laboratory evaluation included a normal basic metabolic panel and complete blood count, but an elevated BNP (3740 pg/ml) and CRP (10 mg/L). A transthoracic echocardiogram demonstrated a left ventricular ejection fraction of 68% with mild mitral and aortic regurgitation. A contrast CT scan to rule out a pulmonary embolism and she was admitted to the medical service.
Given her history and presentation, B burgdorferi IgM and IgG antibodies were obtained (positive). A western blot showed the B burgdorferi antibody to be 7.51 Lyme Index. She remained on telemetry with daily ECGs and intravenous ceftriaxone was initiated. Within 24 hours of initiation of antibiotics she had intermittent competing junctional rhythm with retrograde conduction and a higher frequency of premature atrial or sinus complexes with normal anterograde AV conduction (Figure 3). At 48 hours, there were more conducted sinus or premature atrial complexes with normal AV conduction with competing junctional beats. At 72 hours, sinus rhythm was predominant. By the fourth day of antibiotic therapy, sinus rhythm with normal conduction overtook the junctional rhythm (Figure 3).

She had no further sinus pauses. On follow up, the patient continued to have sinus rhythm with no further dyspnea on exertion or signs of sinus node dysfunction on ECG.
Discussion:
While cardiac manifestations of Lyme disease including conduction system defects such as AV nodal block, bundle branch block, intraventricular conduction defects, as well as supraventricular arrhythmias and ventricular arrhythmias are well known, sinus node dysfunction with an accelerated junctional rhythm and normal AV conduction is a rarely described phenomenon that has only been highlighted in case reports. The abnormalities of Lyme disease are self-limited and thought to be directly related to the inflammatory response to spirochetes within the cardiac tissue. (1, 2, 4-9) In the United States the causative agent is the spirochete Borrelia burgdoferi and in Europe, it may be caused by various spirochetes, including B. afzelii, B. garinii, B. burgdorferi, and other related species [2]. Clinical manifestations of Lyme disease include erythema migrans, arthritis, neuritis, and carditis. Lyme carditis typically occurs weeks to months after the onset of the pathognomic erythema migrans rash during the early disseminated stage of the disease. Between 1% and 10% of patients with untreated Lyme disease in the United States develop carditis; however, the incidence in Europe appears lower at 0.3% to 4% [3].
A literature search reveals only 3 prior case reports of acute sinus node dysfunction in a setting of confirmed Lyme disease, 1 in the United States and 2 in Europe. [6-8]. While the patient above recovered from sinus node dysfunction and accelerated junctional rhythm with antibiotic therapy, a European case report has shown the need for a pacemaker in a 42 year man who was suspected to have infection by B burgdorferi. [8] Another European case report did demonstrate recovery of sinus node function that presented as sinus arrest after treatment with antibiotic for presumed Lyme disease. [6] A North American case report did demonstrate sinus pauses that improved with intravenous ceftriaxone, but the hospital course was protracted lasting 14 days with persistent first degree AV block at the time of discharge. [7] While the incidence of sinus node dysfunction in Lyme disease appears to be relatively low, its recognition is important in the optimal management of the patient. Akin to the therapy for AV nodal conduction problems in Lyme disease, sinus node dysfunction also seems to respond well to antibiotic therapy as was demonstrated in this case. The simultaneous presence of accelerated junctional rhythm is consistent with inflammation of AV node and provides another clue to the diagnosis.
Given the paucity of cases of sinus node dysfunction, especially with accelerated junctional rhythm in the setting of Lyme disease, we present this case to enhance the overall understanding of various presentations of Lyme carditis.
Conclusion:
Accurate diagnosis and monitoring of the clinical progression of sinus node dysfunction in the setting of Lyme carditis is essential given the likelihood of recovery with conservative management with antibiotics and observation, even if temporary pacemaker is required. Permanent pacemaker placement should be delayed to allow recovery even if active fixation permanent pacing lead, with an externalized pacemaker that can be reused is needed [7-8, 10]. When comparing case reports, it is also very important to assess levels of block as our patient had normal AV conduction with every atrial premature complex or with a sinus beat that intermittently manifested two days after starting therapy. The accelerated junctional rhythm was felt to be due to inflammation of the AV node due to Lyme carditis. Our patient recovered quickly and was only kept in the hospital for 4 days until the junctional escape rhythm was overtaken by the recovered sinus node. However, other case reports have shown persistent AV block despite antibiotic therapy without need for a pacemaker [8].
Conflict of Interest Disclosures:
Dr. Rosenfeld: Fellowship support from: Boston Scientific, Medtronic, and St Jude Medical
Dr. Bhatt: Honoraria: St. Jude Medical, Biotronik, Zoll
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
