
Research Article | DOI: https://doi.org/10.31579/2641-0419/217
1 Cardiology Department , Alazhar University hospitals , Cairo, 11675, Egypt
2 Pulmonology Department , Alazhar University hospitals, Cairo, 11675, Egypt
*Corresponding Author: Abdulaziz Aboshahba, Cardiology department, Faculty of Medicine, Alazhar University, Cairo. Egypt.
Citation: Natalia L. Mercado., Mariano Rubio., Martín Cisneros., Santiago Trejo; Maximiliano Giraudo. (2021) Lung Ultrasound B-lines as a Surrogate marker for high Left Ventricular Diastolic Pressures; a bed-side Diagnostic tool. J. Clinical Cardiology and Cardiovascular Interventions, 4(18); DOI:10.31579/2641-0419/217
Copyright: © 2021 Abdulaziz Aboshahba, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 August 2021 | Accepted: 15 September 2021 | Published: 21 December 2021
Keywords: LUS; B-lines; E/e`
Background: We studied the diagnostic accuracy of B-lines (comet-tail sign) on bedside lung US, NT-proBNP, E/e` on ECHO in differentiation of the causes of acute dyspnea in the emergency setting. Major advantages include bedside availability, no radiation, high feasibility and reproducibility, and cost efficiency.
Methods: Our prospective study was performed at the alazhar university hospital, Cairo, Egypt, between July 2019 and March 2020. All patients underwent lung ultrasound examinations, along with TTE, laboratory testing, including rapid NT-proBNP testing.
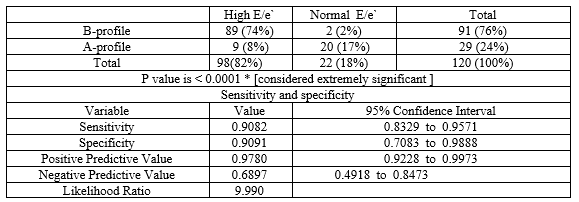
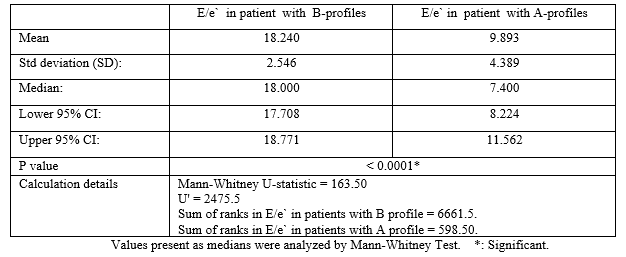
Results: The median E/e’ levels in patients with B-profile were 18, compared with a median of 7.4 in the subjects with A-profile (P =< 0.0001 CI = -9.649 to -7.044). It was found that the sensitivity and the specificity of detecting B-profile on ultrasound is high when E/e’ > 15.5 (95.0% and 83.0% consecutively), which concluded the high correlation between finding B profile on U/S chest and elevated left ventricle filling pressure in a patient presenting with picture of suggestive of heart failure
Conclusion: Chest ultrasound can be used as screening test for the evaluation of patients with suspicion of heart failure with excellent sensitivity and good specificity.


Acute pulmonary edema is a common problem facing emergency department (ED) physicians, and a percentage of these patients are admitted to the coronary care unit (CCU). The diagnosis of acute pulmonary edema remains a challenge for the following reasons: the presentation could be in combination with other diseases, such as chronic obstructive airway disease; and these diseases may have a presentation that is similar to that of acute pulmonary edema [1].
Cardiologists and intensivists commonly assess the heart using echocardiography. To save time, an extended evaluation could be performed using the same probe to complete the evaluation without changing the probe. Chest ultrasound is used to detect subpleural interstitial edema lines (B-lines) and pleural effusion [1]. A B-line is a discrete, laser-like, vertical, hyperechoic image that arises from the pleural line. The B-lines are useful for the diffrential diagnosis of cardiogenic versus non-cardiogenic dyspnea [2].
The assessment of left ventricle diastolic function and filing pressures is of paramount clinical importance to distinguish heart failure (especially heart failure with preserved ejection fraction- (HFPEF)) from other diseases such as pulmonary disease resulting in acute dyspnea. The ratio of E/e’ is used to estimate left ventricle filing pressure (LVFP) and its use is recommended by the American Society of Echocardiography (ASE) and European Society of Cardiology (ESC) for evaluating diastolic dysfunction (DD) and HFpEF [3 ,4].
The assay for plasma ProBNP is a useful test for the evaluation of patients with dyspnea, and it is particularly useful as a component of the evaluation of a suspected heart failure when the diagnosis is uncertain [5].
Recommended cut-off values for the diagnosis of acute HF using NT-proBNP vary substantially. NT-proBNP is renally cleared; therefore, serum levels are affected by age-related declines in renal function. Januzzi et al 2018 showed that age-based NT-proBNP cut-points remain useful for the diagnosis of acute HF and improve diagnostic accuracy compared to any single age-independent cutoff. As rule-in criteria, age-stratified cutoff levels of NT-proBNP for diagnosis of HF were as follows: 450 pg/mL for age <50>75 [ specificity 75.0% ] . As a rule-out criterion, NT-proBNP was excellent at ruling out HF when the level was < 300> 75 years of age. In these cases, other diagnostic tools must be used to diagnose or exclude acute HF. [6]
The aim of our study was to determine the relationship between the B profile on chest ultrasound chest (bilateral comet-tail sign = multiple vertical B lines, referred to as "lung rockets") and E/e’ ratio on Spectral tissue Doppler echocardiography in patients presented with the suspicion of acute pulmonary edema.
Study design
This study was a prospective, observational study in in emergency department (ED) of patients presented with acute dyspnea suspicious of acute pulmonary oedema
Study Population and setting:
This study was include 120 patients presented with acute dyspnea in Alazhar University hospital ED and CCU
Enrollment or Eligibility criteria:
Patients were selected according to the following:
All patients will be subjected to the followings:-
[1] Ethical considerations including Written Informed consent about the type of the study
The study protocol was approved by our local ethics committee.
[2] History taking and physical examination ( Baseline demographic and clinical data )
[3] NT- Pro BNP
[4] Thoracic Ultrasound
Protocol:
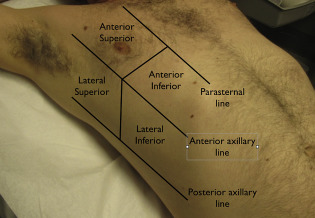
A positive zone is defined by ≥ 3 B-lines in the same zone that can be seen at any moment during a respiratory cycle. Adapted from John J. Eicken, et al.2013 [11]
Measurements:
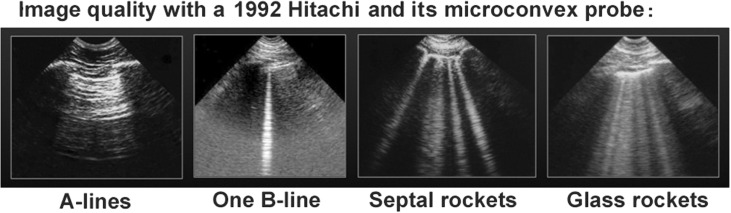
B lines are hyperechoic (white), vertical lines that originate from the pleural line. The appear as “comet tails” and move with lung sliding during inspiration and expiration.
[From Lichtenstein DA et al. The Comet-tail artifact: An Ultrasound Sign of Alevolar-Interstitial Syndrome. Am J Respir Crit Care Med 1997; 156: 1640-1646] [12].

[5] Echocardiography:
Statistical Data analysis:
One hundred and twenty patients (M/F=56/64) with Acute dyspnea referred to our ER and CCU , in Alazhar university hospitals were included in this study.
Baseline demographic & clinical characteristics and Chest ultrasound profiles
Age: The mean age was 67.1 years, with a range of 41 to 94 years;
Sex: 56 (46.7%) of the subjects were males.
Risk Factors: 59 patients (49.17 %) were diabetics, 71 patients (59.167 %) were hypertensives, 43 patient (35.83 %) were smokers , 53 patients (44.16 %) had dyslipidemia , 63 patients (52.5 %) had angina , 60 patients (50 %) had MI, 18 patient (15 %) had CABG , 25 patients (20.83 %) have AF .
Clinical findings: 91 patients (75.8 %) had B- profile and hemodynamic pulmonary edema. The remaining 29 patients (24.2 %) of had A- profile.


There was no statistically significant difference in B-&A-profiles in relation to baseline demographic and risk factors as regard age, sex, diabetes, hypertension, smoking , dyslipidemia, and Angina, whereas B-profiles were more prevalent among patient with prior MI, prior CABG and AF . Also B- profiles were more prevalent in patient with signs of right- and left-sided heart failure (with P-value =0.0001).
Echocardiography and Chest ultrasound profiles
Tissue Doppler echocardiography (E/e` ratio): 17 patients had normal E/e’ (<8>. The statistical analysis revealed that A-profile was present in all patients with normal E/e’ratio (E/e’ of <8> The median of E/e’ levels in patients with B-profile was 18, compared with a median of 7.4 in the subjects with A-profile (P =< 0 xss=removed>
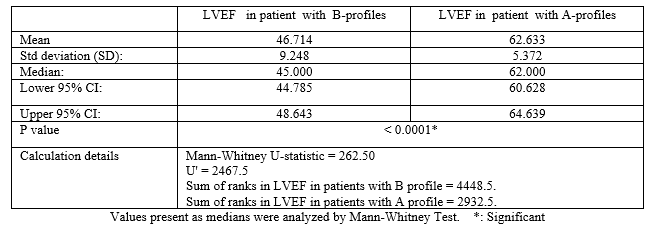
Systolic function (LVEF): The systolic function in the patient with a B-profile was below 50% in 77% of the patient and normal in 23% of the patient. The patient with an A-profile had a systolic function > 55%.

NT Pro-BNP and Chest ultrasound profiles
A-profile was present in all patients with NT-ProBNP <400>
B-profile was present in all patients with NT-ProBNP positive as rule-in HF criterion (>450 pg/mL for age <50> 900 pg/mL for ages 50–75& > 1800 pg/mL for age >75)

B-profile Sensitivity and specificity [Receiver-operating characteristics (ROC) curve]
Based on the threshold level of NT Pro-BNP of 398 and significant elevated E/e’ (>15.5), the sensitivity of detecting B-profile on ultrasound was 95.0%, and the specificity was 83.4%. The positive predictive value of the B-profile was 94.7%, and the negative predictive value was 85.2%.


Acute dyspnea is one of the most common conditions faced in emergency care settings. Accurate diagnosis and treatment are of primary importance, because misdiagnosis can result in deleterious consequences for patients. Timely differentiation of HF from other causes of acute dyspnea may be difficult. Physical examination, chest radiography, electrocardiography, and standard biological tests often fail to accurately differentiate HF from pulmonary causes of dyspnea [17,18,19].
The clinical diagnosis of acute heart failure (HF) syndromes is challenging in the emergency care setting [20]. Steg PG et al, in the landmark “Breathing not Properly Multinational” study, the Framingham score was reported to be 85% sensitive and 58% specific for the clinical diagnosis of congestive HF in a large, unselected patient population presenting with acute dyspnea [21]. Therefore, additional diagnostic methods are required in this clinical setting to accurately establish the diagnosis of acute congestive HF
Rapid NT-proBNP testing, has been validated as a powerful and cost-effctive diagnostic marker of congestive HF [22], and is extensively utilized as the first-line diagnostic complement to clinical and radiographic data in in emergency care settings.
Transthoracic lung ultrasound Detection of B-profile is highly sensitive and specific for elevated NT-proBNP, which helps in diagnosing pulmonary edema. Performing chest ultrasound could be part of the echocardiography evaluation in patients with acute dyspnea [23].
The reliability of transthoracic lung ultrasound in differentiating acute dyspnea has been confirmed in some previous studies by Lichtenstein et al. [3,12], Cardinale et al [24] and Volpicelli et al. [25]. The study by Lichtenstein et al 1997 was performed in the ICU setting on critically ill patients showed a sensitivity of 93.4% and a specificity of 93.0%, together with a feasibility of 99% [12]. The study by Volpicelli et al 2006 was performed in the ED and showed similar results (sensitivity 85.7%, specificity 97.7%, feasibility 98.3%, interobserver variability 4.9%) [25]. The comet-tail sign (B lines) has been proposed as a simple, non-time-consuming sonographic sign of pulmonary congestion and can be obtained at bedside (also with portable echocardiographic equipment) [26]. Agricolla et al. [27] studied the diagnostic accuracy of lung ultrasound in diagnosing intersitial pulmonary edema and found significant positive linear correlations between comet-tail signs and chest radiography, wedge pressure and extravascular lung water quantified by the indicator dilution method. Liteplo et al.[28] reported that lung ultrasound could be used alone or could provide additional predictive power to NT-proBNP in the immediate evaluation of dyspneic patients presenting to the emergency department.
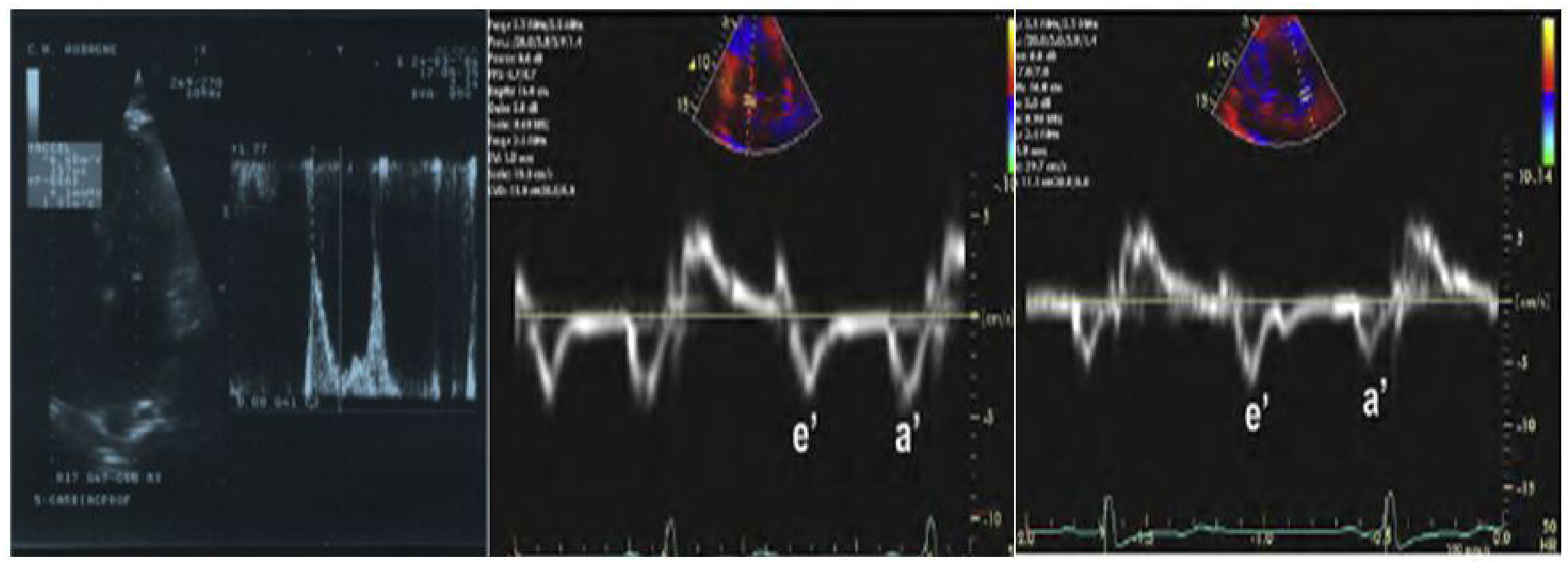
Tissue Doppler echocardiography
The tissue Doppler (E/e`) ratio (a mean of the values obtained at the septum and the lateral wall) is a valuable tool for non-invasive determination of LV diastolic pressures. This ratio is related to pulmonary capillary wedge pressure, so it can be used to identify patients with elevated pulmonary capillary wedge pressure (defined as > 15 mmHg) accurately [29].
The usefulness of bed-side tissue Doppler echocardiography as well as its incremental role over the clinical judgment and BNP testing in the emergency diagnosis of acute HFpEF in patients hospitalized for acute severe dyspnea is well documented and confirmed; this noninvasive method was found to be accurate, even among patients with inconclusive BNP levels (100–400 pg/ml) or arrhythmia [30,31]. The diagnostic accuracy of E/e’ was similar to BNP regardless of LV ejection fraction; furthermore, these 2 methods were able to provide independent diagnostic information, supporting their complementary role in this setting. [32]
Measurement of mitral valve inflow and mitral annular velocity allows the intensivist to identify an elevated or normal left atrial pressure (LAP) in some cases, but may yield an indeterminate result. The ultrasonographer is then required to make a series of echocardiography measurements. Given the time constraints and difficult imaging conditions in the ICU, these are not practical for the frontline intensivist to perform. Instead, lung ultrasonography may be incorporated into the study to estimate LAP. While some data suggest an association between B-line number and right-sided pressures, other did not find a relationship with left-sided pressures as estimated by the PCWP [33]. Agricola et al. studied 20 patients (mean LVEF 64%) before and after cardiac surgery and did see positive correlations between B-lines on lung ultrasound in 28 chest zones and PCWP (r = 0.48) [27]. A study of 72 patients (mean LVEF 41%) undergoing stress echocardiography in which PCWP was estimated echocardiographically by tissue Doppler also found positive correlations between estimated PCWP and B-lines (r = 0.69) [34]. The discrepancy in results between these studies could be due to diffrent size and type of study populations, the fact that there might be an association between B-lines and PCWP, but only in patients with acute decompensated heart failure [33].
In our study the median E/e’ levels in patients with B-profile were 18, compared with a median of 7.4 in the subjects with A-profile (P =< 0 xss=removed>
It was found that the sensitivity and the specificity of detecting B-profile on ultrasound is high when E/e’ > 15.5 (95.0% and 83.0% consecutively), which concluded the high correlation between finding B profile on U/S chest and elevated left ventricle filing pressure in a patient presenting with picture of suggestive of heart failure .
Also it was noticed that most patients with A profile had normal E/e’ ratio.
A study by Zouheir Bitar et al.[1] suggest that the median E/e’ levels in patients with B-profie were 20.8, compared with a median of 8.2 in the subjects with A-profile. It was found that the sensitivity and the specificity of detecting B-profile on ultrasound is high when E/e’ > 15 (95.0% and 92.0% consecutively), which concluded the high correlation between finding B profile on U/S chest and elevated left ventricle filing pressure in a patient presenting with picture of suggestive of heart failure .
The limitations of our study include;
From present study we concluded that:
Chest ultrasound can be used as screening test for the evaluation of patients with suspicion of heart failure with excellent sensitivity and good specificity.The B-line assessment on chest ultrasound is use ful in assessing left-sided filing pressures, so this tool should be considered in a multi-parametric approach of patients with HF. The simplicity of chest ultrasound allows the use of a hand-held device to quickly, easily and adequately evaluate LV filling pressure.
B-lines are an efficient marker of elevated LVFP. Consequently, they should be more frequently implemented in the assessment of LV diastolic function and LVFP. Their implementation could moreover be extremely easy in routine practice, either prior to or immediately after transthoracic echocardiography, and could be completed within less than 3 minutes.
In addition, because of the portability of recently introduced hand-held devices, LUS could further be easily performed throughout the course of in-hospital management or in the outpatient setting. We do believe, as other authors [35, 36, 37], that LUS is more accurate than lung auscultation [38,39] and should thus be routinely performed in patients with HF as an extension of clinical examination.
Lung US enables the clinician to more quickly identify and initiate treatment for the potentially life-threatening causes of acute dyspnea without the need for patient transportation to the radiology suite. Additionally, lung US can repeatedly be implemented to assess clinical changes without concern for repeated radiation exposure and is cost-effective given its ability to decrease the need for additional radiological and laboratory testing to confirm a suspected diagnosis.
I would like to express my deepest gratitude to all staff members of cardiology and pulmonology departments , faculty of medicne, Alazhar university, cairo, Egypt .
AUROC: Area under the receiver-operating curve
BNP: Brain natriuretic peptide
CHF: Congestive heart failure
CI: Confidence interval
COPD: Chronic obstructive pulmonary disease
CVP: Central venous pressure
HF: Heart failure
LR+: Positive likelihood ratio
LR-: Negative likelihood ratio
NPV: Negative predictive value
NT-proBNP: N-terminal pro-brain natriuretic peptide
PPV: Positive predictive value.
Dr. Almarghany and Dr Moaz have nothing to disclose.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
