
Research Article | DOI: https://doi.org/10.31579/2639-4162/233
1European Society for Environmental and Occupational Medicine, Berlin, Germany
2Environmental & Occupational Health, Drexel University School of Public Health, Philadelphia, PA, USA
*Corresponding Author: Xaver Baur, European Society for Environmental and Occupational Medicine, Berlin, Germany.
Citation: Xaver Baur and Arthur L. Frank, (2024), Lung Function Changes After Asbestos Exposure: Implications for Compensation, J. General Medicine and Clinical Practice, 7(18); DOI:10.31579/2639-4162/233
Copyright: 2024, Xaver Baur. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 October 2024 | Accepted: 14 October 2024 | Published: 21 October 2024
Keywords: older adults; risk factors; diseases in older adults
Previous asbestos workers with normal radiography, including chest CT scans, through a literature review have been shown to have significant changes in pulmonary function. This is seen for static and dynamic parameters as well as the transfer factor of the lung for carbon monoxide (TLCO). Much of the literature is of low sensitivity due to the cross-section rather than longitudinal data and selection bias. These effects are greater in those with asbestos-related pleural abnormalities or asbestosis or with both. Many studies document the synergistic effect of smoking with regard to pulmonary function changes, but even dust exposure alone can be seen to lead to changes with negative radiology. Unfortunately, more detailed and sensitive investigations such as longitudinal studies with measurements of TLCO, lung compliance and exercise testing by use of ergospirometry have been very rarely performed or are not available in the study group of interest. Our findings indicate that even sensitive chest CT scanning cannot provide exact lung function data and replace specific pulmonary functional tests. However, by support of AI CT scanning may become more useful for estimation of functional data in the future.
PFT pulmonary function test, CXR chest X ray (radiography), CT computed tomography, FVC forced vital capacity, FEV1 forced expiratory volume in 1 second, TLC total lung capacity, TLCO transfer factor of the lung for carbon monoxide (CO diffusion capacity), VA alveolar volume, TLCO/VA Krogh index
Long-term intensive inhalation of all kinds of inorganic dusts has been shown to cause impairment of lung function, i.e. restrictive and obstructive ventilation patterns (Begin, Ostiguy et al. 1993, Glencross, Weinberg et al. 1997, American Thoracic 2004, Wang, Yano et al. 2006, Dement, Welch et al. 2010, Dement, Welch et al. 2015, Collegium-Ramazzini 2016). This can be explained by the deposition of the more or less biopersistant materials in peripheral airways and in lung tissue associated with ongoing inflammatory and fibrogenic reactions. With regard to asbestos, it has to be noted that a cumulative dose of 1 fiber-year corresponds to an inhalative uptake of about 2 billion asbestos fibers. Using a sheep model Begin et al. (Begin, Masse et al. 1982) demonstrated that heavy asbestos exposure causes inflammatory and fibrotic changes in small airways. Correspondingly, histological investigations of lung tissue of chrysotile-exposed mine workers exhibited generalized fibrosis of small airways of workers which extended the effects of cigarette smoking (Wright and Churg 1985). There is a growing body of evidence that pulmonary function changes caused by inorganic materials including asbestos can occur even in the absence of radiographic changes. Without doubt, compensation has been denied to some because this finding has not been recognized. However, some (Schikowsky, Felten et al. 2017) have denied that lung function can be affected in the absence of radiographic changes, including from CT evaluation.
The latter authors stated: “…we found no significant association between lung function and asbestos exposure. Our results confirm the well-known correlation between lung function, smoking habits, and BMI.” (Schikowsky, Felten et al. 2018). Because this statement has the potential to a cause false understanding of prevention and compensation issues the aim of this work is to review the available relevant literature and thus the veracity of this conclusion.
A literature review and search using PubMed/Medline with the MESH term asbestos plus the terms pulmonary function testing, radiography, CT, computed tomography, and meta-analysis. We combined our literature search findings with data from a metaanalysis (Wilken, Velasco Garrido et al. 2011), literature searches and reviews undertaken in preparing the German guidelines for diagnostics and expert opinion of ARD in which one of the authors (XB) was involved, and a literature-based previous commentary (Baur, Manuwald et al. 2010, Baur and Wilken 2010, Baur, Clasen et al. 2011, Baur, Terracini et al. 2018, AWMF 2020).
A. individual lung function parameters in cross-sectional studies of asbestos workers without abnormal chest CT scans (in brackets: % predicted); values of metaanalysis by Wilken et al. 2011 are given in bold blue letters.
1.Vital capacity (VC or FVC)
Various cross-sectional studies show reduction of -1.2 to -11.2 % of predicted vital capacity in previously asbestos-exposed subjects; in detail: (Oldenburg, Degens et al. 2001) (mean 88.8 + 13.9%; s.)*; (Rui, De Zotti et al. 2004) (mean 96 %, s.)*; (Harkin, McGuinness et al. 1996) (mean 98 %, n.s.)*; (Begin, Ostiguy et al. 1993) with Pleura score of 0-5 (mean 93 %, s.)*; (Clark, Flynn et al. 2014) (mean 90,8 %, n.s.);(Clark, Flynn et al. 2017) at 60 years mean 94.0% and at 80 years mean 84.4%); (Park, Yates et al. 2015) (mean 98.8 %, n.s.); (Neri, Antonelli et al. 1994) with normal PFT selected (mean 96.5 %, n.s.); (Miller, Szeinuk et al. 2018) (mean 93,5 %, n.s.), Schikowsky et al. (Schikowsky, Felten et al. 2018) (mean 98.5 %, n.s.)Lopatin et al. (Lopatin, Tsay et al. 2016, Lopatin, Tsay et al. 2016) found that 75% of the asbestos study group with normal CT scans exhibited significantly reduced vital capacity values. In one publication (Preisser 2020) vital capacity corresponded to the outdated references from Quanjer et al. from 1983/1993 (Quanjer, Tammeling et al. 1993)) (mean 100.1%).
In two publications increased values of vital capacity were reported: (Begin, Filion et al. 1995) (mean 102 %, n.s.); (Van Cleemput, De Raeve et al. 2001) (mean 109.8, s.; the latter also used the outdated references from Quanjer et al. from 1983/1993 (Quanjer, Tammeling et al. 1993)).
*included in the metaanalysis of publications till 2010 by Wilken et al. (Wilken, Velasco Garrido et al. 2011) and in the review by Baur et al. (Baur, Terracini et al. 2018); overall, in the metaanalysis mean FVC was 97.1% (p=0.51).
1. Forced expiratory volume in one second (FEV1)
In most cross-sectional studies FEV1 was reported to be reduced, range -3 to -13 % predicted. In detail: (Oldenburg, Degens et al. 2001) (87%, s.)*; (Harkin, McGuinness et al. 1996) (mean 94 %, n.s.)*; (Begin, Ostiguy et al. 1993) with Pleura score of 0-5 (mean 96 %, n.s.)*; (Begin,
Filion et al. 1995) (mean 95 %, n.s.) *; (Clark, Flynn et al. 2014) (80.5%); (Clark, Flynn et al. 2017) at 60 years mean 93.1%and at 80 years mean 87 %); (Neri, Antonelli et al. 1994) with normal PFT selected (mean 94.7 %, n.s.); (Miller, Szeinuk et al. 2018) (mean (95,7 %, n.s.), Schikowsky et al. (Schikowsky, Felten et al. 2018) (mean 95.8 %, n.s.). (Park, Yates et al. 2015) (mean 90.4 %, n.s.). In two studies using outdated reference values increased FEV1 was reported (Van Cleemput, De Raeve et al. 2001, Rui, De Zotti et al. 2004)* (mean 103.8 %, 103 % respectively, both n.s.)*. Lopatin et al. (Lopatin, Tsay et al. 2016, Lopatin, Tsay et al. 2016) found that FEV1 is significantly reduced in 62% of these subjects.
*Included in the metaanalysis of publications until 2010 by Wilken et al. (Wilken, Velasco Garrido et al. 2011) and in the review by (Baur, Terracini et al. 2018); overall, in the metaanalysis mean FEV1 was 90.4 % (n.s.).
2. FEV1/FVC
This is given in only a few studies showing small reductions. In detail: (Park, Yates et al. 2015) (mean 70.8 %, s.); (Oldenburg, Degens et al. 2001) (mean 94.9 %; n.s.)*, (Neri, Antonelli et al. 1994) with normal PFT selected (mean 98.6 %, n.s.).
*included in review by (Baur, Manuwald et al. 2010) and in the metaanalysis of publications till 2010 by Wilken et al. (Wilken, Velasco Garrido et al. 2011) and in the review by (Baur, Terracini et al. 2018); overall, mean FEV1/FVC was 94.9 %, n.s.).
3. Transfer factor of the lung for carbon monoxide (TLCO)
In all but one study mean reduction from predicted values ranged from 2.8 - to - 9.2%. In detail: (Miller, Szeinuk et al. 2018) (mean 95,7 %, n.s.), (Park, Yates et al. 2015) (mean 87.6 %, n.s.); (Begin, Ostiguy et al. 1993) with Pleura score of 0-5 (mean 95%); (Van Cleemput, De Raeve et al. 2001) (mean 97.2%, n.s.); (Preisser 2020 ) (mean 79.7%); (Neri, Antonelli et al. 1994) normal PFT selected (mean 118.4 %, n.s.); (Clark, Flynn et al. 2014) (mean 97.1%, n.s.) (with TLCO/VA mean 98.8%), (Clark, Flynn et al. 2017) (at 60 years mean 98.9% and at 80 years mean 91.3 %). Interestingly, the study by (Schikowsky, Felten et al. 2018) reports increased TLCO/VA (mean 111.4 % (n.s.) but did not provide TLCO data.
4. Longitudinal studies and other lung function parameters
The longitudinal study in Libby vermiculite asbestos workers by (Clark, Flynn et al. 2017) showed decreases of adjusted FEV1, FVC, TLC and TLCO percent predicted means at 40, 60 and 80 years of age also in the group with normal CT scan (- 12.3%, - 13.2, - 15.3%, - 22.6 %). Appropriate results from exercise testing by use of ergospirometry or from lung compliance were not available.
A) Influence of underlying asbestosis or asbestos-related pleural disorders or confounding factors
1. Asbestosis and/or asbestos-related pleural disorders
The literature shows that lung function impairment is typically greater in previously asbestos- exposed subjects with evidence of underlying asbestosis and/or asbestos-related pleural disorders than in those without such radiologically identified changes (Kilburn and Warshaw 1991, Kilburn and Warshaw 1994, Algranti, Freitas et al. 2000, Algranti, Mendonca et al. 2001, Lebedova, Dlouha et al. 2003, Ameille, Letourneux et al. 2010, Wang, Wang et al. 2010, Wilken, Velasco Garrido et al. 2011, Algranti, Mendonca et al. 2013, Kopylev, Christensen et al. 2015, Clark, Flynn et al. 2017, Miller, Szeinuk et al. 2018).
2. Smoking
Smoking has been shown to be a complicating factor (Kilburn and Warshaw 1994, Bagatin, Neder et al. 2005, Abejie, Wang et al. 2010, Wilken, Velasco Garrido et al. 2011, Algranti, Mendonca et al. 2013, Yang, Yan et al. 2018).
3. BMI
Algranti et al. (Algranti, Mendonca et al. 2001) mentioned that obstructive ventilation patterns and shortness of breath of asbestos workers are significantly associated with body mass index. However, as shown by Salome et al. even in the extremely obese spirometric variables and TLCO are rarely below the normal range (Salome, King et al. 2010).
B) Combined findings of the literature search
We identified many studies with CT scans in asbestos workers looking at data only with those who had evidence of non-malignant disease and were not useful for this analysis.
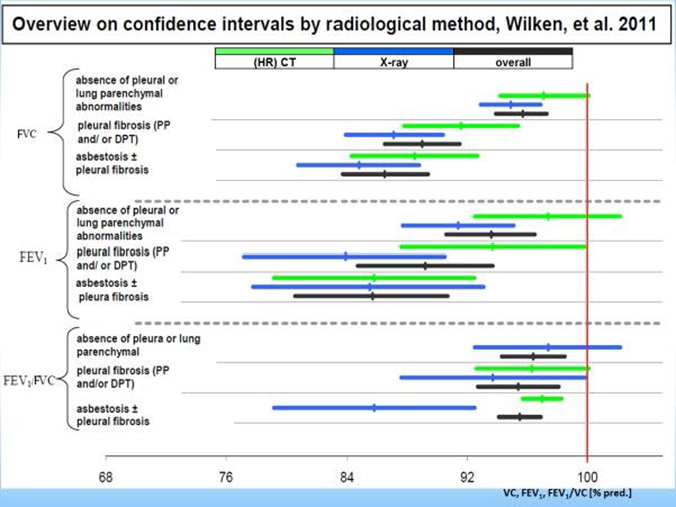
The scientific literature we could use documents that when sensitive CT is used to establish the presence or absence of underlying non-malignant disease, data shows that even those with negative CT scans still have pulmonary function impairment although these effects are lower than in those with asbestos-related pleural abnormalities or asbestosis or with both (Algranti, Freitas et al. 2000, Ameille, Letourneux et al. 2010, Wang, Wang et al. 2010, Algranti, Mendonca et al. 2013) (Kilburn and Warshaw 1991, Kilburn and Warshaw 1994, Algranti, Mendonca et al. 2001, Wilken, Velasco Garrido et al. 2011). This is especially documented in a meta-analysis (Fig.) and in the longitudinal study of workers exposed to Libby amphiboles in vermiculite who have decreases of pulmonary function values over time (Clark, Flynn et al. 2017).
Literature also shows that changes is typically greater with a history of smoking (Kilburn and Warshaw 1994, Bagatin, Neder et al. 2005, Abejie, Wang et al. 2010, Wilken, Velasco Garrido et al. 2011, Algranti, Mendonca et al. 2013, Yang, Yan et al. 2018).
B. individual lung function parameters in cross-sectional studies of asbestos workers without abnormal chest CT scans (in brackets: % predicted); values of metaanalysis by Wilken et al. 2011 are given in bold blue letters.
5. Vital capacity (VC or FVC)
Various cross-sectional studies show reduction of -1.2 to -11.2 % of predicted vital capacity in previously asbestos-exposed subjects; in detail: (Oldenburg, Degens et al. 2001) (mean 88.8 + 13.9%; s.)*; (Rui, De Zotti et al. 2004) (mean 96 %, s.)*; (Harkin, McGuinness et al. 1996) (mean 98 %, n.s.)*; (Begin, Ostiguy et al. 1993) with Pleura score of 0-5 (mean 93 %, s.)*; (Clark, Flynn et al. 2014) (mean 90,8 %, n.s.);(Clark, Flynn et al. 2017) at 60 years mean 94.0% and at 80 years mean 84.4%); (Park, Yates et al. 2015) (mean 98.8 %, n.s.); (Neri, Antonelli et al. 1994) with normal PFT selected (mean 96.5 %, n.s.); (Miller, Szeinuk et al. 2018) (mean 93,5 %, n.s.), Schikowsky et al. (Schikowsky, Felten et al. 2018) (mean 98.5 %, n.s.)Lopatin et al. (Lopatin, Tsay et al. 2016, Lopatin, Tsay et al. 2016) found that 75% of the asbestos study group with normal CT scans exhibited significantly reduced vital capacity values. In one publication (Preisser 2020 ) vital capacity corresponded to the outdated references from Quanjer et al. from 1983/1993 (Quanjer, Tammeling et al. 1993)) (mean 100.1%).
In two publications increased values of vital capacity were reported: (Begin, Filion et al. 1995) (mean 102 %, n.s.); (Van Cleemput, De Raeve et al. 2001) (mean 109.8, s.; the latter also used the outdated references from Quanjer et al. from 1983/1993 (Quanjer, Tammeling et al. 1993)).
*included in the metaanalysis of publications till 2010 by Wilken et al. (Wilken, Velasco Garrido et al. 2011) and in the review by Baur et al. (Baur, Terracini et al. 2018); overall, in the metaanalysis mean FVC was 97.1% (p=0.51).
6. Forced expiratory volume in one second (FEV1)
In most cross-sectional studies FEV1 was reported to be reduced, range -3 to -13 % predicted. In detail: (Oldenburg, Degens et al. 2001) (87%, s.)*; (Harkin, McGuinness et al. 1996) (mean 94
%, n.s.)*; (Begin, Ostiguy et al. 1993) with Pleura score of 0-5 (mean 96 %, n.s.)*; (Begin,
Filion et al. 1995) (mean 95 %, n.s.)*; (Clark, Flynn et al. 2014) (80.5% ); (Clark, Flynn et al. 2017) at 60 years mean 93.1%and at 80 years mean 87 %); (Neri, Antonelli et al. 1994) with normal PFT selected (mean 94.7 %, n.s.); (Miller, Szeinuk et al. 2018) (mean (95,7 %, n.s.), Schikowsky et al. (Schikowsky, Felten et al. 2018) (mean 95.8 %, n.s.). (Park, Yates et al. 2015) (mean 90.4 %, n.s.). In two studies using outdated reference values increased FEV1 was reported (Van Cleemput, De Raeve et al. 2001, Rui, De Zotti et al. 2004)* (mean 103.8 %, 103 % respectively, both n.s.)*. Lopatin et al. (Lopatin, Tsay et al. 2016, Lopatin, Tsay et al. 2016) found that FEV1 is significantly reduced in 62% of these subjects.
*Included in the metaanalysis of publications until 2010 by Wilken et al. (Wilken, Velasco Garrido et al. 2011) and in the review by (Baur, Terracini et al. 2018); overall, in the metaanalysis mean FEV1 was 90.4 % (n.s.).
7. FEV1/FVC
This is given in only a few studies showing small reductions. In detail: (Park, Yates et al. 2015) (mean 70.8 %, s.); (Oldenburg, Degens et al. 2001) (mean 94.9 %; n.s.)*, (Neri, Antonelli et al. 1994) with normal PFT selected (mean 98.6 %, n.s.).
*included in review by (Baur, Manuwald et al. 2010) and in the metaanalysis of publications till 2010 by Wilken et al. (Wilken, Velasco Garrido et al. 2011) and in the review by (Baur, Terracini et al. 2018); overall, mean FEV1/FVC was 94.9 %, n.s.).
8. Transfer factor of the lung for carbon monoxide (TLCO)
In all but one study mean reduction from predicted values ranged from 2.8 - to - 9.2%. In detail: (Miller, Szeinuk et al. 2018) (mean 95,7 %, n.s.), (Park, Yates et al. 2015) (mean 87.6 %, n.s.); (Begin, Ostiguy et al. 1993) with Pleura score of 0-5 (mean 95%); (Van Cleemput, De Raeve et al. 2001) (mean 97.2%, n.s.); (Preisser 2020 ) (mean 79.7%); (Neri, Antonelli et al. 1994) normal PFT selected (mean 118.4 %, n.s.); (Clark, Flynn et al. 2014) (mean 97.1%, n.s.) (with TLCO/VA mean 98.8%), (Clark, Flynn et al. 2017) (at 60 years mean 98.9% and at 80 years mean 91.3 %). Interestingly, the study by (Schikowsky, Felten et al. 2018) reports increased TLCO/VA (mean 111.4 % (n.s.) but did not provide TLCO data.
9. Longitudinal studies and other lung function parameters
The longitudinal study in Libby vermiculite asbestos workers by (Clark, Flynn et al. 2017) showed decreases of adjusted FEV1, FVC, TLC and TLCO percent predicted means at 40, 60 and 80 years of age also in the group with normal CT scan (- 12.3%, - 13.2, - 15.3%, - 22.6 %). Appropriate results from exercise testing by use of ergospirometry or from lung compliance were not available.
C) Influence of underlying asbestosis or asbestos-related pleural disorders or confounding factors
4. Asbestosis and/or asbestos-related pleural disorders
The literature shows that lung function impairment is typically greater in previously asbestos- exposed subjects with evidence of underlying asbestosis and/or asbestos-related pleural disorders than in those without such radiologically identified changes (Kilburn and Warshaw 1991, Kilburn and Warshaw 1994, Algranti, Freitas et al. 2000, Algranti, Mendonca et al. 2001, Lebedova, Dlouha et al. 2003, Ameille, Letourneux et al. 2010, Wang, Wang et al. 2010, Wilken, Velasco Garrido et al. 2011, Algranti, Mendonca et al. 2013, Kopylev, Christensen et al. 2015, Clark, Flynn et al. 2017, Miller, Szeinuk et al. 2018).
5. Smoking
Smoking has been shown to be a complicating factor (Kilburn and Warshaw 1994, Bagatin, Neder et al. 2005, Abejie, Wang et al. 2010, Wilken, Velasco Garrido et al. 2011, Algranti, Mendonca et al. 2013, Yang, Yan et al. 2018).
6. BMI
Algranti et al. (Algranti, Mendonca et al. 2001) mentioned that obstructive ventilation patterns and shortness of breath of asbestos workers are significantly associated with body mass index. However, as shown by Salome et al. even in the extremely obese spirometric variables and TLCO are rarely below the normal range (Salome, King et al. 2010).
A) Combined findings of the literature search
We identified many studies with CT scans in asbestos workers looking at data only with those who had evidence of non-malignant disease and were not useful for this analysis.
The scientific literature we could use documents that when sensitive CT is used to establish the presence or absence of underlying non-malignant disease, data shows that even those with negative CT scans still have pulmonary function impairment although these effects are lower than in those with asbestos-related pleural abnormalities or asbestosis or with both (Algranti, Freitas et al. 2000, Ameille, Letourneux et al. 2010, Wang, Wang et al. 2010, Algranti, Mendonca et al. 2013) (Kilburn and Warshaw 1991, Kilburn and Warshaw 1994, Algranti, Mendonca et al. 2001, Wilken, Velasco Garrido et al. 2011). This is especially documented in a meta-analysis (Fig.) and in the longitudinal study of workers exposed to Libby amphiboles in vermiculite who have decreases of pulmonary function values over time (Clark, Flynn et al. 2017).
Literature also shows that changes is typically greater with a history of smoking (Kilburn and Warshaw 1994, Bagatin, Neder et al. 2005, Abejie, Wang et al. 2010, Wilken, Velasco Garrido et al. 2011, Algranti, Mendonca et al. 2013, Yang, Yan et al. 2018).

Exposure to asbestos is well known to produce a wide variety of disorders, both non-malignant and malignant. Compensation issues vary around the world, as does access to other forms of legal redress.
As early as 1971 it was reported that previous asbestos workers have reduced pulmonary function values even in the absence of asbestosis (Jodoin, Gibbs et al. 1971). Our review confirms and broadens these initial findings showing decreases of spirometric and TLCO values not only in asbestos-exposed subjects with asbestosis or asbestos-associated pleural abnormalities but also in those with normal chest CT scans. This includes impairment of forced vital capacity (FVC) with some studies that are statistically significant (Oldenburg et al. 2001, Rui et al 2004, Begin et al. 1993, Harkin et al. 1996; Clark et al. 2014; Lopatin et al. 2016, Wilken et al. 2011). Also, there are many studies with changes in forced expiratory volume in 1 second (FEV1) (Oldenburg et al. 2001, Harkin et al. 1996, Begin et al.1993, Begin et al. 1995, Clark et al 2014, Lopatin et al 2016, Wilken et al 2011), and several of TLCO (Begin, Ostiguy et al. 1993, Van Cleemput, De Raeve et al. 2001, Clark, Flynn et al. 2014, Park, Yates et al. 2015, Miller, Szeinuk et al. 2018). Correspondingly, Lopatin et al. report that 75% of their subject group had decreased FVC values and 62% of them had decreased FEV1 values; in this publication no relationship with reference values is given. Studies not finding similar results are those of Rui et al. (Rui, De Zotti et al. 2004) for FEV1 and of van Cleemput et al. (Van Cleemput, De Raeve et al. 2001) for FVC and FEV1 [these authors applied questionable or outdated references from Quanjer et al. from 1983/1993 (Quanjer, Tammeling et al. 1993)], and of Schikowsky et al. (Schikowsky, Felten et al. 2018) for TLCO/VA.
CT scans are much more sensitive than CXR for the determination of morphological changes of the lungs and pleura due to asbestos and other harmful exposures (Neri, Antonelli et al. 1994, Preisser 2020). Nevertheless, as mentioned, when CT is used to establish the presence or absence of underlying non-malignant disease, data shows that those with negative CT scans one can still have pulmonary function changes (Wilken, Velasco Garrido et al. 2011). This indicates that CT scanning cannot provide detailed functional impairment insight. Copeley et al. (Copley, Wells et al. 2001) found that only 58 % and 57 % of TLC and TLCO variability of asbestos workers can be explained by combined CT morphological findings.
By referring to the questionable statement of Schikowsky et al. (Schikowsky,
Felten et al. 2017) indicating “the lung function parameters of FVC, FEV1, DLCO/VA, and airway resistance were significantly associated with the burden of smoking, BMI and years since end of exposure (only DLCO/VA). However, they were not affected by factors (e.g. cumulative exposure) or duration of asbestos exposure… We found no significant association between lung function and asbestos exposure” the aforementioned and further shortcomings (low statistical power, not considering individual available previous asbestos air concentrations and previous lung function data, citation of non-relevant references, obvious, but undeclared conflict of interest), were recently pinpointed (Baur, Terracini et al. 2018) and could not be clearly negated (Schikowsky, Felten et al. 2018).
It should be noted that the additive adverse effect of asbestos exposure to adverse smoking effect on lung function is well documented (Kilburn and Warshaw 1994, Bagatin, Neder et al. 2005, Abejie, Wang et al. 2010, Wilken, Velasco Garrido et al. 2011, Algranti, Mendonca et al. 2013, Yang, Yan et al. 2018) and that BMI has little or no influence on FVC, FEV1 and TLCO (Salome, King et al. 2010). As opposed to Schikowsky et al., there is convincing evidence that the dose of asbestos and duration of asbestos exposure is associated with functional impairment (Frank 1979, Begin, Ostiguy et al. 1993, Bagatin, Neder et al. 2005, Wang, Yano et al. 2006). In the more differentiating German guideline for expert opinion, diagnostics, and compensation of asbestos-related occupational diseases) it is mentioned: “According to experience with other inorganic dusts, several studies with chest x-rays indicate slight lung function limitations in groups exposed to asbestos that do not show any radiological changes (Miller et al. (Miller, Szeinuk et al. 2018) [63], and meta-analysis by Wilken et al. [118] …. A study based on X-ray [69]
(Bagatin, Neder et al. 2005) showed dependence of the FVC on the cumulative asbestos fiber dose…. Therefore, it has to be assumedthat the functional limitations in groups with normal chest x-rays cannot be fully explained by image morphology and that asbestos exposure can also be associated with slight functional limitations regardless of the radiological findings…. In CT studies, evidence of such functional limitations without asbestos-related changes in the CT can also be found in studies by Szeinuk et al. (Szeinuk, Noonan et al. 2017) and Lopatin et al. (Lopatin, Tsay et al. 2016, Lopatin, Tsay et al. 2016) (in the latter publication, heavy smokers exposed to asbestos were compared with and without CT changes) [80,81,103]. …However, overall, no or only very small, statistically insignificant changes in lung function are described when radiological findings did not show abnormalities” (cited references are (Ameille, Letourneux et al. 2010, Wilken, Velasco Garrido et al. 2011, Clark, Flynn et al. 2014, Lopatin, Tsay et al. 2016, Lopatin, Tsay et al. 2016, Szeinuk, Noonan et al. 2017, Schikowsky, Felten et al. 2018) 80, 81, 85, 86, 89, 102, 118).
It should be noted that the publications by Ameille et al. 2010 (Ref. 86) which is cited in the aforementioned guideline does not present relationship of chest CT scan findings and lung function parameters; thus, this work does not allow any conclusion regarding the question, whether the subjects’ lung function parameters differ from reference values. All the other cited publications show mild functional impairments as given above. Furthermore, various studies with similar effects (see Result section above) are not mentioned in this guideline and the severe limitations with underestimation of the effects of asbestos especially due to the healthy worker effect are not taken into consideration.
Interestingly, the Draft Opinion of The Advisory Committee on Safety and Health at Work to the European Union for an Update of Commission Recommendation (EU) 2022/2337 concerning the European schedule of occupational disease includes in the new list of occupational diseases among others (ovary cancer and larynx cancer due to asbestos) pleural plaques with functional impairment of the lungs as well as non-malignant pleural effusion caused by asbestos exposure (listed in Annex I). However, the mostly small impairments of routinely measured spirometric values of previous asbestos workers with normal chest CT scans do not fulfil occupational disease criteria of European countries, although a significant proportion of them suffer from chronic bronchitis, COPD, and/or shortness of breath during exercise, and in some of them a significant asbestos-related decline of FVC and FEV1 over time can be documented, i.e. of at least 20
It is clear from the scientific literature over many years that individuals exposed to asbestos, even with normal radiology, by either CXR or CT, can still be shown to have negative alterations in their pulmonary function test results that can be ascribed to their prior exposures. Obviously, these alterations are underestimated in most available studies due to the healthy worker effect and the consideration of only spirometric data which are of much lower sensitive than measurement of CO diffusing capacity (Garcia, Griffith et al. 1990, Baur and Wilken 2010, Preisser, Velasco Garrido et al. 2011, Miller, Szeinuk et al. 2018, Modi and Cascella 2020) or ergospiromtry parameters (Wasserman, Hansen et al. 2011). Many studies document the synergistic effect of smoking with regard to pulmonary function changes, but even dust exposure alone can be seen to lead to changes with negative radiology.
These facts have significant implications for individuals who may be denied compensation following asbestos exposure when their radiographic findings do not show evidence of non- malignant disease. In fairness to such individuals.
Conflict of interests
XB has performed medical expert opinions for various German social courts and statutory accident institutions. ALF regularly participates in asbestos-related medical-legal activities, primarily for plaintiffs.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
