
case report | DOI: https://doi.org/10.31579/2690-4861/447
*Corresponding Author: Ahmad Nassar, 23, Rue Georges Bizet. 75116 Paris, France.
Citation: Ahmad Nassar, (2024), Lower Limb Elephnatiasis Nostras Verrucosa: Excision with full thickness skin grafting with aid of dermal regeneration template, International Journal of Clinical Case Reports and Reviews, 18(3); DOI:10.31579/2690-4861/447
Copyright: © 2024, Ahmad Nassar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 April 2024 | Accepted: 09 May 2024 | Published: 09 July 2024
Keywords: ionizing radiation; radiation-induced eye impairment; radiotherapy; radiation incidents; post-irradiation eye reactions
Elephnatiasis Nostras Verrucosa (ENV) is a rare clinical condition, a progressively disfiguring disorder characterized by verrucous, nodules and cobblestone-like papules associated with non-pitting edema of the lower extremities. Histopathology is characterized by epidermal hyperkeratosis and dermal fibrosis.
We report the history of a 32-year-old man who presented with 5 years history of right lower limb edema covered by nodular and papular skin lesions. Proper investigations put the diagnosis of ENV. The patient was successfully treated by debridement followed by skin graft using the technique of dermal regeneration. Management of ENV remains challenging. In the absence of randomized controlled trials on the best modalities of treatment, it is important to report such rare cases and their treatment outcome.
Elephantiasis nostras verrucosa (ENV), a non-filarial obstruction of the lymphatic channels, is a debilitating complication of chronic lymphedema (1). Multiple factors such as surgery, tumor, scleroderma, radiation, trauma, recurrent soft tissue infections, obesity and congestive heart failure can lead to lymphatic obstruction (1, 2, 5). ENV is characterized by diffusely scattered, verrucous, cobblestone-like papules and nodules, associated with non-pitting edema of the lower extremities (3). The management of ENV is often challenging. There is no universal consensus for a defined treatment strategy. A different type of medical and surgical treatment procedures has been proposed (4).
A 32-y-old man, previously healthy, presented to outpatient clinic for a 5-year history of right lower limb edema followed by the appearance of multiple skin lesions on the right leg and right foot.
There is no skin pain or pruritus. He denied fever, chills, weight loss, gastro-intestinal or respiratory symptoms. No travel history to note. Past medical history was significant for complicated recurrent cellulitis that have been treated by debridement and skin autograft applications, while family history was insignificant. In our hospital, vital signs were within normal range.
Physical examination showed non-pitting right lower limb edema with multiple exophytic, mossy, cobblestone like papules and nodules covering the edematous skin (Figure 1,2).

Laboratory investigation revealed: erythrocyte sedimentation rate = 37 (NL<20 xss=removed xss=removed xss=removed>
Figure 1: crust and cobblestone-like papulonodules on the right leg and foot
Figure 2: foot deformities due to superimposed hyperkeratotic papulonodules with a verrucose or cobblestone-like appearance
Lower extremity MRI showed severe lobulated thickening of the skin and subcutaneous fat with diffuse stranding, decreased space between the anterior and posterior muscle compartments with moderate atrophy of the muscles were noted. These findings were compatible with the picture of chronic calcific fasciitis. In addition, lower extremity arterial Doppler
confirmed the absence of stenosis of femoral, anterior and posterior tibial arteries.
An incisional skin biopsy (figure 3) from lesion showed acanthosis and hyperkeratosis of the epidermis, associated with dermal hypertrophy with mild perivascular lymphocytic exudate concentrated around ectatic lymphatics (Figure 4,5).

Figure 3: incisional skin biopsy of the right leg.
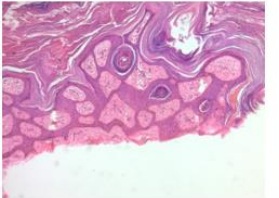
Figure 4: epidermal hyperplasia.
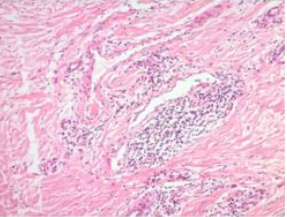
Figure 5: Dermal edema, lymphocyticin filtrate
Thus, we made the diagnosis of non-filarial ENV following recurrent soft tissue infections of the concerned area of the body.
The patient was hospitalized, several successive debridement procedures have been carried out. All the skin layers, from the legs to the dorsal side
of the foot including spaces between toes, were removed until the aponeurosis of the muscle. These procedures were followed by the application of a vaccum dressing to be changed every 5 days (figure 6).

Figure 6: after debridement and Vacuum Dressing
Figure 7: Application of Integra
Healthy granulation tissue was observed days later. Then, the patient was prepared for the dermal regeneration technique known as ‘’integra’’ (figure 7). It was carried out in 2 phases. Firstly, the integra template was applied circumferentially from the leg to the dorsal aspect of the foot. The first dressing change was made 5 days later, followed by changes twice a
week. After 3 weeks, the silicone layer of integra was removed and replaced successfully by a skin autograft from the thighs (figure 8).
The patient was observed after 1 month with acceptable result (Figure 9).
Eight months later, we observed a remission of the total skin treated by integra while there was a recurrence between the toes of the right foot not covered by this procedure (figure 10).

Figure 8: directly after skin graft from the Thigh.
Elephantiasis nostras verrucosa, a rare complication of chronic lymphedema, can lead to severe disfigurements of the affected body parts [5]. The exact incidence and prevalence is not determined. The lower extremities are most commonly affected but other localizations have been reported [3].
The exact pathogenesis underlying ENV remains unknown. Induction of fibroblast proliferation, disturbance of the local immune response and predominant TH-17 population were mentioned in the literature [7, 8]. Histopathology is marked by hyperkeratosis and papillomatosis of the epidermis associated with dermal or subcutaneous fibrosis giving a verrucous appearance [5,6]. Diagnosis is made clinically where Skin biopsy is indicated to rule out a malignant process [4]. Differential diagnosis of ENV may include filariasis, papillomatosis cutis carcinoides, lipodermatosclerosis, chromoblastomycosis and papular mucinosis [4]. Our patient has a unilateral presentation probably due to history of recurrent soft tissue infection. ENV is a difficult disorder to treat. Much of what is written is based on published case reports and case series. Extenuating lymphedema is of great significance in the initial management of patients [4]. Conservative measures including compression dressing and weight loss can in turn improve the skin surface [9]. Concerning the medical options, oral retinoids at daily dose of 0.6- 0.75 mg/kg for several weeks has been reported to be beneficial in the management of ENV [4]. Polat M et al. reported a case of a 64-year-old man with erythrodermic psoriasis and ENV in whom the lesions were cured almost completely after low dose acitretin treatment [10]. Topical retinoids and topical keratolytics were also given with low level of clinical evidence [4]. On the other hand, the role of antibacterial agents is not well established [10]. For resistant cases, surgical debridement may represent an applicable selection.
Some surgeons preferred the preparation of the skin by topical keratolytics to soften the surface prior to the operation [4]. Although the risk of recurrence is unrecognized since the underlying pathology was not specially managed. Recently, Sancho AQ et al described a case of ENV successfully treated with CO2 laser [7].
Our patient has already had operations based on debridement followed by skin grafting. However, recurrences were noted. For that, a multidisciplinary team bringing together grouping dermatological, vascular, orthopedic, and plastic surgery was held to discuss the best way to manage the situation of the patient. The decision regarding medical treatment composed of oral retinoids has been excluded given their side effects with the need for regular follow monitoring of the blood test. Also the local treatments and the laser therapy were suspended for their low level of evidence. Since the surgical treatment is effective. It represents a good option but with unknown risk of recurrence. The decision was to proceed with the use of dermal regeneration template. First introduced in 1981 by Burke and Yannas [13].
Basically, integra is a system consisting of two layers of skin regeneration. The outer layer, composed of thin silicon film, works as a barrier to cover the wound. And the inner layer, constructed of cross-linked collagen fibers, is the matrix to regenerate the dermal layer of the skin [13]. Once the dermal skin has been regenerated, the silicon layer is removed and replaced by a thin epidermal skin graft to achieve a full-thickness skin equivalent [12]. The new collagen is histologically indiscernible from normal dermal collagen [11]. Integra is available in large quantities. Also, the process is simple and reliable. It seems to represent a new alternative in reconstructive surgery [12]. Dantzer et al displayed a series of 31 patients who underwent artificial dermis, results were considered good in 28 cases after a period of 6 months to 4 years of follow-up [12]. Otherwise, the requirement of two operations, detachment of silicon layer, skin infections, disease recurrence and high price represent the disadvantages of integra [12,14]. To consider this technique more effective than debridement alone, we need comparative studies in the future. In our patient, no recurrence was detected in the area treated by integra followed by graft compared to the area treated only by graft To our knowledge, this is the first case of ENV treated by dermal regeneration template.
Elephantiasis nostras verrucosa is a progressively disfiguring disease. Management is challenging due the lack of randomized trials, we think that Dermal regeneration template gives good result for the healing of ENV. presentation of such cases may be helpful by sharing experience with different modalities of treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
