
Research Article | DOI: https://doi.org/10.31579/2641-0419/045
1Department of Internal Medicine, Niger Delta University, Amassoma.
2University of Port Harcourt Teaching Hospital, Port Harcourt
*Corresponding Author: Edafe Emmanuel Auchi. Department of Internal Medicine, Niger Delta University, Amassoma.
Citation: Edafe Emmanuel Auchi, Odia .O. James, (2020) Long-term Home use of Dobutamine in end-stage Heart Failure in Nigeria: a case report and Review of literatures.. J. Clinical Cardiology and Cardiovascular Interventions, 4(6); Doi:10.31579/2641-0419/045
Copyright: © 2020 Edafe Emmanuel Auchi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 February 2020 | Accepted: 19 June 2020 | Published: 30 June 2020
Keywords: dobutamine, refractory heart failure, long term use, home.
Introduction: Dobutamine increases cardiac contractility and causes vasodilation with little change in heart rate. It has been used in management of acute heart failure. It has also been document for use in management of chronic heart failure. We reported 86 year old man with refractory heart on long term dobutamine.
Case Summary: A 86-year-old retired civil servant living with hypertension for 26 years, type 2 Diabetes Mellitus (T2DM) for 14 years and hyperlipidemia for 10 years. He was diagnosed with biventricular failure 4 ago and had cardiac resynchronization therapy (CRT-D) implanted 3 years ago. He presented to the emergency department with 3 weeks history of bilateral leg swelling, dyspnea, orthopnea, paroxysmal nocturnal dyspnea and oliguria. He has more than 12 repeated hospital admission for heart failure in the past 4 years despites CRT-D. He was noted to be anxious and diaphoretic with a respiratory rate of 36 breaths/minute, blood pressure of 84/52 mm Hg, heart rate 80 beats/minute. Peripheral pulses were threated and diminished in amplitude, and his hands and feet were cool and moist. A summation gallop was noted over the precordium. Fine crepitations were heard over the posterobasal regions of both lungs. The electrocardiogram showed a pacemaker rhythms. He was treated for NYHA class IV heart failure with digoxin, and dobutamine. He was discharged home on long term dobutamine infusion.
CONCLUSION: Home dobutamine is a simple and effective in term treatment for end-stage heart failure. Its widespread use may be restricted by cost and expertise considerations in Nigeria
Dobutamine increases cardiac contractility and causes vasodilation with little change in heart rate [1,2]. It is routinely administered for short periods to relieve exacerbations of congestive heart failure (CHF) in hospitalized patients [3-5]. Sustained effects have been seen with dobutamine infusions, although the known properties of the drug do not explain these effects [6,7]. Long-term dobutamine therapy could lessen the symptoms of CHF and improve exercise tolerance and cardiac function [2,4]. It could be used in patients with refractory heart failure and that awaiting heart transplantation. It also benefits patients with contra-indication to heart transplantation.[2,4] Because the therapy has not been shown to prolong survival in most patients, specific endpoints of therapy could be determined for each patient. Because it may cause sudden death, patients receiving this therapy must be carefully monitored. Long-term use of dobutamine infusion lessens the symptoms of CHF has not been shown to prolong survival but it reduces frequency of hospital admission.[4,5]
Outpatient dobutamine infusion for heart failure has not come into a routine practice and prescription in Nigeria medical practice. However, the world being a global village, many of our heart failure patients now travel oversea to seek more advanced medical care in other countries outside Nigeria. They return home after a brief stay of managing the acute condition in those hospitals. At home in Nigeria, they would present to the physicians for continue follow up. Hence we report this case with review of literature that been on long-term home use of dobutamine in end-stage heart failure from our facility outpatient department in Nigeria.
An 86-year-old retired civil servant who had been living with hypertension for 26 years, type 2 Diabetes Mellitus (T2DM) for 14 years and hyperlipidemia for 10 years. He was diagnosed with biventricular failure 4 ago and had cardiac resynchronization therapy (CRT-D) implanted 3 years ago in a hospital in the United States of America. He presented to the emergency department with 6 weeks history of recurrent bilateral leg swelling with associated dyspnea, orthopnea, paroxysmal nocturnal dyspnea and oliguria. He has more than 12 repeated hospital admission for heart failure in the past 4 years after the CRT-D. Hecontinued to be admitted every 2 to 3 with gross leg edema, acute pulmonary edema, hypotension andangina.
At the emergency room, he was noted to be anxious and diaphoretic with a respiratory rate of 36 breaths/minute, not pale, anicteric, no digital clubbing, and bilateral leg edema up to the mid-shin. The chest showed bilateral crepitation in both lung lungs zones. Pulse was 102 beats/minute (diminished in amplitude, and his hands and feet were cool and clammy), blood pressure of 84/50 mm Hg. His jugular venous pressure was elevated at 12 cm H2O. A summation gallop (S1,S2 and S3) was noted over the precordium. Finger and ear pulse oxygen saturation was 80% on room air and 96% on 4 L/min via nasal cannula. The serum sodium 124 mmol/l, potassium 3.9mmmol/l, urea 15 mmol/l (3.2-9mmol/l), creatine 350ɥmol/l. The electrocardiogram showed a pacemaker rhythm. The echocardiography showed an ejection fraction of 28%, dilated four chambers
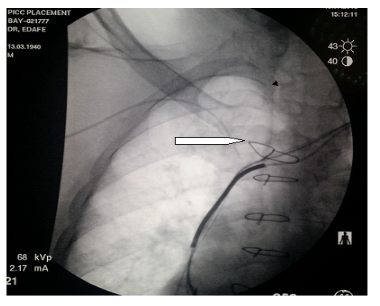
Dobutamine (8 mcg/kg/min), sub-cutaneous clexane (0.4mls), and digoxin (0.125 mg) daily were initially commenced. The blood pressure improved and sustained in the ranged of systolic (120-130mmHg) and diastolic (80-90mmHg) on dobutamine. Furosemide 80 mgtwice daily was added to the treatment when his blood pressure improved.Dobutamine was later maintained at a dose of 5 µg/kg/minute,with improvement in cardiac output and consequentdiuresis. Any attempt to wean him off dobutamine, his clinical condition worsened. He continued on infusion rate with the diluted drugin a dose of 2000 mg in 500 mls of 5% Dextrose water and run 125mls per day at a rate of 5 drops per minute from Moog Curlin infusion Pump (Curlin Medical) via a Bard pink peripheral venous line with an inline bacterial filter (Figures 1,2,3,4.5 ). He was discharged self-caring with help from his general practitioner and a nurse.



Two months later he was content with his quality of lifeand able to walk from a car and return to his usual business. He continued toreceive continuous dobutamine infusion for over 8
Months with no thrombotic infective complicationsof treatment with sustained clinical improvement. He has been carrying out his official and home function with no episodes of pulmonary edema or worsening of his heart failure. There has been improvement in exercise tolerance and quality of life, and freedom fromhospital admission.Functional improvement from NYHA 4 to 2 in four months.
The patient has been on home dobutamine infusion via a pink peripheral line inserted through the right basilic vein for 7 months. The peripheral pink link line was changed after 7 month and no complication noted. This home based dobutamine infusion continued till the 9th month when he stated having deterioration in heart failure back to stage 4 NYHA. This he battled with for another 3 month before he died of cardiopulmonary collapse.
Dobutamine is a member of the catecholamine family of adrenergic agents. It was formulated to augment ventricular systolic function (8-12). Dobutamine acts principally through stimulation of β1-adrenergic receptors with lesser stimulation of β2- and α-adrenergic receptors [10-11]. Therefore, dobutamine enhances ventricular contraction with little net direct effect on peripheral vasculature [10-11]. In the setting of human heart failure, the cardiac β1-adrenergic receptors are generally down regulated from chronic stimulation (elevated circulating catecholamines) or blocked by β1-selective adrenergic blockers; most of dobutamine’s hemodynamic effects are then most likely rendered through β2-adrenergic stimulation In states of ventricular systolic dysfunction, dobutamine increases contractility, stroke volume, and cardiac output [10-11,13].
In the clinical setting with reduced ventricular systolic function, filling pressures, reduced stroke volume and cardiac output, and systemic and organ hypoperfusion, dobutamine increases stroke volume, cardiac output, systemic pressure, and systemic and organ perfusion, and reduces ventricular filling pressures and systemic and pulmonic vascular resistances [10-11, 13-16]. Our patient was on Dobutamine to improve the contractility and renal perfusion. Proper dose selection and increamentation achieve these favorable responses without significantly increasing heart rate or provoking other adverse effects [13-14, 17-18]. Our patient has not reported any adverse effect of the Dobutamine. He continued till the 9th month at home before he symptoms started dederiotating. He finally passed from cardiopulmonary collapse. The relatively wide separation of positive inotropic and chronotropic effects is an ideal pharmacologic property of an agent intended for short-term therapy of systolic cardiac failure, but this wide separation cannot be maintained for dobutamine if the initial dose is too high [17-20].
Dobutamine also has a favorable effect on ventricular diastolic properties and on ventricular-vascular coupling by reducing aortic impedance [16]. As a positive inotropic agent, dobutamine increases myocardial oxygen consumption [14]. In human low-output cardiac failure, the patient substrate for dobutamine use, this agent increases enterohepatic, renal, and limb blood flow proportional to the augmentation in cardiac output [21-28]. Our patient had better renal perfusion with improvement in urine output, leg edema and reduced hospital admission.
At Ohio State University, long-term dobutamine therapy (typically 5.0-7.5 micrograms/kg/min infused continuously) is used in patients with refractory CHF and that awaiting heart transplantation [29]. Our patient had CRT-D implantation yet still having episodes of hospital admission for heart failure. This necessitates the use of dobutamine infusion. Because the therapy does not prolong survival in most patients, he has benefitted with no hospital admission in the past 8 months. Because it may cause sudden death, patients receiving this therapy must be carefully monitored. Long-term use of dobutamine infusion lessens the symptoms of CHF but does not prolong survival [24-27]. Our patient has been out of hospital admission since the commencement of dobutamine infusion.
The main argument against continuous homedobutamine infusion is financial. The drug alone in ourcase cost approximately 70 thousand naira per week, with othercharges for lines, 5%D/W and syringes plus a degree of homesupervision and maintenance of the line. Our patient was able to afford it. The pink peripheral line was changed in our facility under ultrasound guidiance and fluoroscopy in a procedure that lasted for 15 to 20 mines under local anaesthesia. Our patient was saved from protracted hospital hospitalization
Conclusion: Home dobutamine is a simple and effective in term treatment for end-stage heart failure. Its widespreaduse may be restricted by cost and expertise considerations in Nigeria.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
