
Review Article | DOI: https://doi.org/10.31579/2578-8868/297
Dept of Pathology, Torrance Memorial Medical Center, 3330 Lomita Blvd, Torrance, CA 90505.
*Corresponding Author: Patrick W. Chambers, Dept of Pathology, Torrance Memorial Medical Center, 3330 Lomita Blvd, Torrance, CA 90505.
Citation: Patrick W. Chambers, (2024), Long Covid, the Gut, and Autoimmune Skin Diseases: A Novel Therapeutic Approach, J. Neuroscience and Neurological Surgery, 15(1); DOI:10.31579/2578-8868/297
Copyright: © 2024, Patrick W. Chambers. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 04 January 2024 | Accepted: 22 January 2024 | Published: 29 January 2024
Keywords: IFN-γ; γδ T cells; microbiome; d-mannose; TNF-α
The dermatological manifestations of Long Covid (LC) have languished in the shadows of chronic fatigue and brain fog. Yet they are all linked by gut dysbiosis and the cytokine triad of TNF-α, IL-1β, and IL-6. The gut microbiome common not only to LC, psoriasis, AA, and vitiligo but also to neurodegenerative disease has been recently described. This gut microbiome induces an altered tryptophan metabolism linked to autoimmune disease. SARS CoV2, Mycobacteria, and many intestinal parasites protectively upregulate IFN-γ (less Covid in BCG and in subSaharan Africa), triggering the characteristic altered tryptophan metabolism and curtailing synthesis of serotonin and melatonin. Chronic inflammation due to persistent spike protein S exhausts IFN-γ and leads to gut dysbiosis and autoimmune risk. Butyrate immunomodulates IFN-γ and TGF-β, which counterbalance each other (reciprocal relationship). Low IFN-γ (LC) translates to high TGF-β (organ fibrosis). This review suggests that an etiologic prebiotic (d-mannose)/probiotic (lactobacilli, bifidobacteria)/postbiotic (butyrate) approach to autoimmune skin disease that improves intestinal barrier integrity and that suppresses the triad of TNF-α, IL-6, and IL-1β may enhance or even eliminate the traditional immunotherapy of targeted monoclonal antibodies, Janus kinase inhibitors, and steroids. Health benefits of this approach extend well beyond suppression of autoimmune skin disease. Societal benefits include relief to those most affected - women (LC), especially of color (AA, psoriasis, vitiligo).
LC is considered by many to be primarily an autoimmune disease [1]. A German study that followed over half a million patients post Covid-19 reported new onset autoimmune disease in almost 50% [2]. According to the NIH, there are more than 80 different autoimmune diseases. Three of the top ten involve skin disorders - psoriasis (3%), AA (2%), and vitiligo (1%). Two others, pemphigus vulgaris and bullous pemphigoid, have also been reported in those with LC [3,4,5,6].Autoimmune disease risk has traditionally been ascribed to genetic and environmental factors. However, the contributory role of the gut microbiome is rapidly establishing a legitimate challenge to this paradigm. The realm of therapeutic approaches to preventing and treating autoimmune disease has expanded with this recognition. Yet many practicing dermatologists are either unaware of recent therapeutic breakthroughs or fearful of deviating from the designated menu of tailored immunotherapies, e.g., steroids, cytokine monoclonal antibodies, Janus kinase inhibitors. These are not without significant side effects. A gut microbiome approach not only skirts this downside issue but is also much more comprehensive, offering benefits well beyond the integumentary system, e.g., improves diabetes, obesity, lung disease, and some tumors [7], not to mention Alzheimer’s disease(AD) [8,9]. Furthermore, this approach to healthcare puts control back into the hands of the highly motivated patient at less expense and greater convenience.
1. LC, Gut Dysbiosis, and Autoimmune Disease
A decreased CD4+/CD8+ T cell ratio, as seen in AIDS, indicates impaired immune function. An increased ratio, as seen in Covid-19, indicates an overactive immune system. Although impaired CD4+ T cell function in autoimmune disease has been known for decades, CD8+ T cells have recently been identified as key epigenetic contributors, e.g., DNA methylation, in maintaining self recognition [10]. The loss of CD8+ T cells in LC appears integral to its autoimmune categorization. Autoimmune risk is directly proportional to both Covid 19 severity and age [11]. Leaky gut syndrome aka dysbiosis is associated with autoimmune disease [12,13,14] and is linked to LC [15,16]. Gut dysbiosis has been associated with other viral infections linked to subsequent autoimmune disease, e.g., EBV [17]. Leaky gut syndrome stimulates autoimmune pathogenesis. Probiotics containing lactobacilli and bifidobacteria suppress autoimmune risk [18].
2. Gut Microbiome of LC, AA, Psoriasis, Vitiligo
Firmicutes and Bacteroidetes are two dominant phyla that together comprise 90% of the total gut microbiota. The F/B ratio is recognized as an important index of gut microbiota health[19] and is widely accepted as having an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiotic. The former is usually observed with obesity and the latter with inflammatory bowel disease (IBD) [20]. But the real measure of a healthy gut microbiome is an abundance of butyrate producing bacteria [21].The gut microbiome in LC features increased F/B, decreased butyrate producing bacteria, and low biodiversity [22,23]. In AA the F/B ratio is increased [24] and butyrate decreased [25]. The F/B in the gut microbiome of psoriasis is also increased [26] with less biodiversity [27]and decreased butyrate producing bacteria [28]. The gut microbiome of vitiligo also features an increased F/B ratio (twice that of healthy controls) [29] and decreased butyrate[30].Decreased butyrate producing bacteria have also been reported in pemphigus vulgaris31 and bullous pemphigoid [32].The increased F/B ratio in the gut microbiome of these three autoimmune skin disorders may be due in part to obesity, which is a risk factor for AA33, psoriasis34, and vitiligo [35].Obesity is also a risk factor for LC [36]. The adipokines associated with obesity reflect the same cytokine triad signature (TNF-α, IL-6, IL-1β) seen in autoimmune skin disease [37]. This links the high F/B ratio, low butyrate, low biodiversity in the gut microbiomes that characterize these autoimmune skin disorders and obesity with the cytokine triad they frequently exhibit [38,39].
3. The triad of TNF-α, IL-6, and IL-1β in Covid-19, LC, AA, psoriasis, vitiligo, autoimmune disease, cancer, and dementia.
TNF-α, IL-1β, and IL-6 are premiere cytokines linked to autoimmune disease [40]. TNF-α upregulates IL-1β [41] and IL-6[42]. Two other cytokines frequently accompany the triad - IL-17 and IFN-γ. IL-17 can induce the triad (TNFα, IL-6, and IL-1β) [43] and in turn can be induced by the triad [44]. Viruses and fungi, especially Candida, are potent inducers of IFN-γ[45,46,47]. IFN-γ is especially effective against fungi [48] and viruses [49]. Intermediate levels of IFN-γ (20-150 pg/mL) appear to be beneficial50 and may reflect a healthy gut microbiome [51,52], while exhausted levels (<20>150 pg/mL) (hospitalization) appear to be unfavorable [53].Females exhibit more robust T cell activation than males [54] and produce higher levels of interferon [55]. Furthermore, estrogen promotes Candida overgrowth56, which fosters gut dysbiosis [57]. This may explain why 80% of autoimmune disease is seen in females and why LC is encountered more frequently in females. The triad of TNFα, IL-1β, and IL-6 is central to Covid-1958 and LC59,60. This triad of TNF-α, IL-6, and IL-1β is a hallmark of autoimmune disease [61,62], cancer [63,64] and dementia [65]. Furthermore, an increased risk of AD is linked with psoriasis66, AA [67], and vitiligo68. AD is also tightly linked to the triad of TNF-α, IL-6, and IL-1β69.
4. Prevention and Therapy
A. D-mannoseD-mannose preserves intestinal barrier integrity by blocking TNF-α [70]. D-mannose can also suppress IL-1β71, IL-672, and IL-1773.The presence of CD147 (the falciparum antigen) on the spike protein S of SARS CoV2 was initially reported in late 2020[74]. Several articles challenging their report have been discredited [75]. The immune dysfunction in Covid-19 cannot be explained in the absence of CD147 on the spike protein S. The surface expression of CD147 v ACE2 on CD4+ and CD8+ T cells is overwhelming. This is important, as the immune dysfunction subsequent to the SARS CoV2 induced loss of CD 147+ CD8+ T cells (increased CD4+/CD8+) impacts cytokines prominent in LC.There are two kinds of T cells - αβ T cells and γδ T cells. The majority are αβ (95% of circulating T cells and 80% of tissue T cells). All αβ T cells express surface CD147. γδ T cells do not [76]. When CD147+ T cells decrease (AIDS, Covid-19), absolute numbers of CD147- γδ T cells increase [77]. This means secretion of more TNF-α, IL-17, and especially IFN-γ [77,78]. Persistent spike protein S (LC) triggers consumption of CD147+ CD8+ T cells with a consequent increase in IFN-γ producing γδ T cells.TNF-α inhibits mannosidase [79], thereby limiting mannose trimming of glycans in the Golgi and increasing oligomannose glycans. Oligomannose glycan shields induced by TNF-α also activate pathogenic γδ T cells to secrete IL-17[80]. Epidermal γδ T cells are upregulated in AA81, psoriasis [73], and vitiligo [82,83].The estrogen driven [55] increase in type I interferons (α and β) induces additional STAT dependent IFN-γ secretion that drives the altered tryptophan metabolism until IFN-γ production in the face of persistent spike protein S84 is exhausted (see figure 1). The TNF-α and γδ T cell [80] driven IL-17 completes a vicious loop with TNF-α and the triad. By suppressing TNF-α producing T cells and IL-17 producing epidermal γδ T cells d-mannose does double duty in suppressing autoimmune skin disease risk.D-mannose is considered a prebiotic, because consuming it stimulates the growth of good microbiota. Probiotic capsules contain “good” microbiota, e.g., bifidobacteria and lactobacilli. D-mannose may be especially helpful in preventing gut dysbiosis [85,86], tightly linked to autoimmune disease. D-mannose has proven efficacy against autoimmune disease, e.g., T1DM [87], rheumatoid arthritis, and lupus [88]. This prebiotic/probiotic approach is complemented by the postbiotic butyrate.
B.Butyrate
Butyrate is considered a postbiotic because it is produced by gut microbiota. Short chain fatty acids, especially butyrate, suppress IDO and increase serotonin (see figure 1) [89,90]The altered tryptophan metabolism seen in Covid-19 and LC [91] is due to the shift of tryptophan metabolism from serotonin synthesis to the kynurenine pathway [92] (see figure 1).
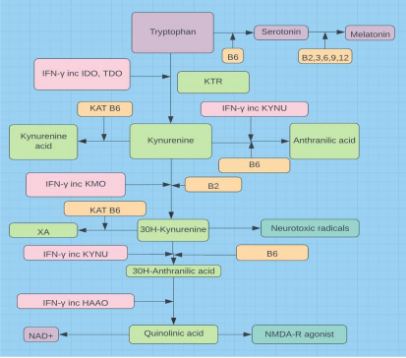
Figure 1: Roles and relationships of the major players in the altered metabolism of tryptophan, essential to gut dysbiosis, Covid-19, LC, autoimmune disease, AD, and cancer risks. As mitochondrial dysfunction mounts, tryptophan metabolism pivots from serotonin synthesis to the kynurenine pathway and NAD+ synthesis to counter the loss of ATP production.
This shift is also linked to intestinal dysbiosis and increased risk of autoimmune disease [93](see figure 2). The magnitude of the shift is inversely proportional to the CD8+ T cell count (T cell lymphopenia=>increased dysbiosis) and autoimmune risk [94]. The kynurenine-to-tryptophan ratio is also directly predictive of Covid severity [95], AD[96], and cancer risk[97].Butyrate immunomodulates IFN-γ [98] and TGF-β [99]. Low IFN-γ [100] and elevated TGF-β [101,102] are directly responsible for the autoimmunity and organ fibrosis encountered in LC. Depressed butyrate has also been directly linked to decreased CRC[103] and down regulation of estrogen receptor positive breast cancers [104]. The butyrate induced increase in serotonin is manifest in the hippocampus, forestalling dementia and AD [105]. Fungi, especially Candida, have been implicated in AD [106] and serotonin actively attenuates pathogenic yeast [107], as does butyrate [108]. AD related amyloid beta bodies are well described in the hippocampus and amyloid beta bodies are linked to Candida [109,110]. Butyrate also increases transcription of the vitamin D receptor gene111 and vitamin D promotes butyrate producing gut bacteria [112].

Figure 2. Figure discloses the healthful benefits (green) of a prebiotic, probiotic, postbiotic, vitamin D, and magnesium approach. Triad=TNF-α, IL-6, IL-1β, CRC=colorectal cancer, NF-kB=nuclear factor kappa B. Estrogen promotes Candida overgrowth 56. Not shown ⬇butyrate => ⬇IFN-gamma => ⬆TGF-beta => organ fibrosis.
B. Vitamin D
Vitamin D deficiency is linked with LC [113] and is prevalent in autoimmune disease[114,115]. Vitamin D downregulates NF-Κb [116], a pro inflammatory cytokine linked to overproduction of the triad. It also suppresses almost all cytokines associated with psoriasis and psoriatic arthritis (see figures 3 and 4).

Figure 3. Figure discloses a wide range of commercial products targeting cytokines and receptors that promote psoriasis, Crohn’s, RA, MS [117].

Figure 4. Figure discloses that all the immunotherapies involving psoriasis and other autoimmune diseases in figure 2 and more are covered by vitamin D [118].
C. Magnesium and B Vitamins
Magnesium is a vital cofactor required for the synthesis of both the storage and active forms of vitamin D. Many of the symptoms of LC are associated with hypomagnesemia [119].
Deficiency is linked with immune dysfunction and risk of autoimmune disease [120].
The growing recognition of differential methylation of DNA in the pathogenesis of autoimmune disease [121,122,123] and the linkage between autoimmune disease and elevated Hcy [124,125] raises the specter of increased autoimmune disease in those with MTHFR (methylenetetrahydrofolate reductase) variants afflicted with LC. Indeed a recent meta analysis demonstrated a direct connection between MTHFR 677 C/T and 1298 A/C polymorphisms and increased risk of autoimmune disease [126]. According to the CDC, more than half of Americans have at least one MTHFR polymorphism. MTHFR polymorphisms are associated with AA [127], psoriasis [128], and vitiligo [129]. Elevated Hcy is also associated with psoriasis [130] and vitiligo [131,132]. The vital role of magnesium and B vitamin sufficiency in minimizing the deleterious effects of MTHFR polymorphisms is seen in figure 5. They enhance both the recycling and the degradation of homocysteine. Glutathione is the “master“ antioxidant.

Figure 5. MTHFR is the rate limiting step. Magnesium is a required cofactor or ATP conjugate and B2,3,6,9,12 are required cofactors for many involved enzymes.
In the most recent reviews on treatment for AA [133], psoriasis [134], and vitiligo [135]TNF-α, IL-6, IL-1β, and IFN-γ have been targets of immunotherapy. These targets may be more comprehensively addressed without toxic side effects by addressing the gut dysbiosis associated with these autoimmune diseases. A regimen of prebiotics, probiotics, postbiotics, vitamin D, and magnesium is at the top of this approach (see figure 2). This novel therapeutic approach to autoimmune skin diseases outlined in this review is in part theoretical and awaits an appropriately structured randomized controlled trial on the efficacy of d-mannose and butyrate in this regard. It may enhance or possibly replace immunotherapy in some who are so afflicted. Relief would flow to women (LC/T1DM87/other autoimmune diseases), especially those of color (AA [136], psoriasis [137], vitiligo [138], AD [139], T2DM [140]).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
