
Research Article | DOI: https://doi.org/10.31579/2690-4861/214
1 Pathologists , Department of Pathology, Chitwan Medical College and Teaching Hospital, Nepal.
*Corresponding Author: Sushna Maharjan, Chitwan Medical College and Teaching Hospital, Bharatpur, Nepal
Citation: Sushna Maharjan, Ranjita Singh, Prabha Panthi, Nirbija Dhakal, Sabin Ranabhat, et al. (2022). Liquid Based Pap Smears for Detection of Infective Organisms in a Tertiary Care Hospital. J. International Journal of Clinical Case Reports and Reviews. 11(3); DOI:10.31579/2690-4861/214
Copyright: © 2022 Sushna Maharjan, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2022 | Accepted: 18 April 2022 | Published: 14 June 2022
Keywords: bacterial vaginosis; cervico-vaginal infection; infective organisms; liquid-based pap smears; trichomonal vaginitis; vulvovaginal candidiasis
Background: Bacterial vaginosis (BV), vulvovaginal candidiasis (VVC) and trichomonal vaginitis (TV) are the most common etiologies of infective vaginitis. The Papanicolaou (Pap) smear is a standard screening test for cervical precancerous lesions that can also be useful to identify infective organisms. This study aimed to identify the causativeorganisms for cervico-vaginal infection in liquid-based Pap smears.
Methods: This study was a cross sectional study and included 370 liquid based Pap smears with infective organisms.
Results: The most prevalent cervico-vaginal infection was BV, which was detected in 259 (70%) of the cases, followed by VVC in 64 (17.3%) and TV in 25 (6.8%) cases.Women aged 30-39 years were mostlyaffected.
Conclusion: The present study shows the usefulness of cervical Pap smear in diagnosis of infective vaginitisother than epithelial cell abnormalities.
Bacterial vaginosis (BV), vulvovaginal candidiasis (VVC), trichomonal vaginitis (TV), Papanicolaou (Pap), BV-associated bacterium (BVAB), liquid-based cytology (LBC), the Bethesda System (TBS), Institutional Review Committee of Chitwan Medical College and Teaching Hospital (CMCIRC), statistical package for the social sciences (SPSS), Windows Microsoft Windows (MS-Windows)
Bacterial vaginosis (BV), vulvovaginal candidiasis (VVC) and trichomonal vaginitis (TV) are the most common etiologies of infective vaginitis, accounting for about 90% of cases [1]. A variety of possible microbial infections have been implicated in the disease process of BV, both individually and in combination. Gardnerella, Atopobium, Prevotella,Peptostreptococcus, Mobiluncus, Sneathia, Leptotrichia, Mycoplasma, and BV-associated bacterium 1 (BVAB1) to BVAB3 are among the probable agents [2]. TV is caused by the flagellate protozoan parasite Trichomonas vaginalis, which is sexually transmitted disease [3]. BV and TV frequently occur concurrently [4]. TV helps to create ananaerobicenvironment that favorsthe development of BV [5]. VVC is caused by the overgrowth of Candida albicans that is part of the vaginal flora [6]. VCC is thoughtto affect 75% of women at some point during their lives [7]. Other causes of infective vaginitisare Actinomyces, Chlamydiatrachomatis, Herpes SimplexVirus, Leptothrix vaginalis, Cytomegalovirus, Enterobius vermicularis, and Schistosoma [8].The Papanicolaou (Pap) smear is a standard screening test for cervical precancerous lesions. It is, nevertheless, useful for identifying infectious organisms [9]. Inflammatory Pap smear is the common diagnosis reportedas negative for intraepithelial lesion and mostly under-investigated because of non-specific inflammation. Thus, the proper guidelines to work up and follow up of the patients with inflammatory Pap smears are lacking. Pathologists should intensively look for infectious organisms in inflammatory Pap smears. The aim of the present study was to identify the causative organisms for cervico-vaginal infections in liquid-based Pap smears.
This study was a hospital-based cross sectional study conducted in Department of Pathology, ChitwanMedical College and Teaching Hospital, Chitwan from September 2021 to February 2022 and included 370 symptomatic and asymptomatic women screened with Pap smears. The symptomatic patients had complained of discharge per vaginum, painabdomen and abnormalbleeding. Pregnant women were excluded.Cervico-vaginal smears were collected for liquid-based cytologytechnique in Gynecology outpatient department by scraping cells from squamocolumnar junction using Rovex Cervex Cyto brush and the brush was dipped totally into a disposable liquid-based cytology (LBC) vial containing preservative fluid. The LBC vials were sent to Department of Pathology for cytological examination. The processing of samples and staining of smears was undertaken as per the prescribed protocol by BD SurePathTM method (LBC, BD Diagnostics, Becton,Dickinson and Company). The slides were analyzed by two consultant pathologists using an Olympus CX23 microscope and classified according to the Bethesda System (TBS) for ReportingCervical Cytology 2014. An informedverbal consent was obtained from all the patients included in the study. Ethical approval was taken from the Institutional Review Committee of Chitwan Medical College and Teaching Hospital (CMC-IRC). Data analysis was done by using the statistical package for the social sciences (SPSS) version20 for Windows Microsoft Windows(MS-Windows) (SPSS Inc.,Chicago, Illinois, the United States).
Diagnostic criteria for various infective organisms found in LBC Pap smear were as follows:
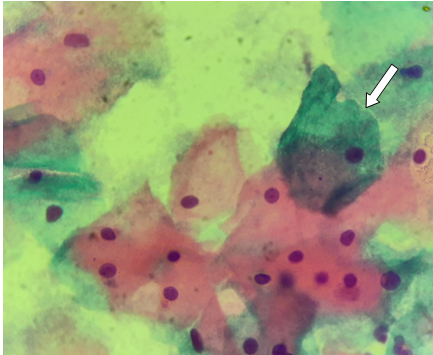
Bacterial vaginosis- presenceof clue cells (squamouscells covered by a layer of coccobacilli obscuring the cell membrane) and conspicuous absence of lactobacilli.
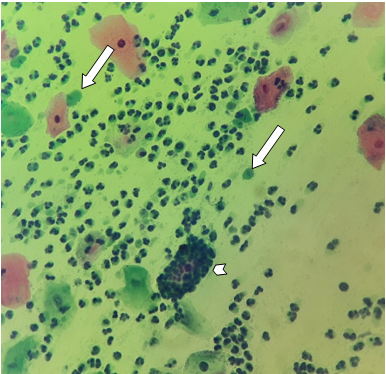
Vulvovaginal candidiasis- presence of pseudohyphae and/or buddingyeast forms.
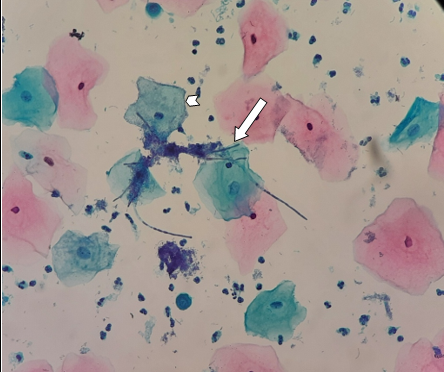
Trichomonal vaginitis- presenceof pear-shaped, oval, or round cyanophilic organisms; few associated background changes like mature squamous cells with small perinuclear halo and 3- dimensional clusters of neutrophils (polyballs or cannon balls). Leptothrix- segmented, lengthy, and filamentous organisms; may be seen in association with Trichomonas vaginalis.
During the study period,1117 LBC Pap smears were examined. Infectiveorganisms were found in 370 (33.1%) cases of the 1117 Pap smears examined (Table 1 and 2). The most common infection encountered was BV (Figure1) in 259 (70%) cases followed by VVC (Figure2) in 64 (17.3%) cases and trichomonal vaginitis (Figure 3) in 25 (6.8%) cases (Table 1). Co-infection with mixed organisms (BV and VVC, BV and TV, VVC and TV) was seen in 20 (5.4%) cases (Table 1).
The age of women in the present study ranged from 20 to 67 years.Women aged 30-39 years were commonly affected; comprising 140 (37.8%) cases (Table 2). Thelowest frequency was observed in the age group 60 years or above, constituting 13 (3.5%) cases (Table 2).

In sexually active women, vaginitis is one of the most frequent reproductive tract infections [10, 11]. Patients present clinically with abnormal vaginal discharge and irritation of vulva, vagina, or both [10, 12]. In Nepal, one in every three women requiresgynecological evaluation due to abnormal vaginal discharge [11]. In the current study, 33.1% of women had infective vaginitis either due single or mixed organisms. This finding is comparable to the reportsfrom Iran and Africa [13, 14]. However, the prevalence of infective vaginitis was extremely low among women in other study of Nepal [15]. Diversestudy populations, varyingclimate, socioeconomic, and cultural situations, different sensitivity of diagnostic tests,and the use of different diagnostic methods all contribute to these variations. Bacterial vaginosis was the most common type of infective vaginitis in the present study which is comparable to other reports [16-19]. When compared to prior other Nepalese research [16-19], we found a high prevalence of BV (70 %). Severalmicrobiological techniques are compared with Pap smear for diagnosing BV. Gram stain is used for microbiological examination to compare diagnostic accuracy to Pap stain. According to Tokyol et al. [20], Pap smear is not sensitive enoughfor BV screening when compared to microbiological results, but due of its high specificity, it may be an adequate diagnostic criteriawhen it is positive. VVC was the second most common infection, with 17.3% of women infected, which is lower than other Nepalese studies[17, 18]. Takei et al. stated that the liquid-based Pap smear was more sensitiveand specific for the identification of candida than other organisms (bacteria and Trichomonas vaginalis) due to the large size of candidain contrast to other organisms. The larger organism may not be removed during the liquid preparation process, resulting in an increase in the number of organismson the smear. Trichomonas vaginitis was diagnosed in 6.8% of women in the present study. However, the other study from neal detected no cases of TV [22]. The most common clinical feature in infected women is symptomatic vaginitis [22]. De Glehn et al. [23] discovered that TV infection was linked to the number of lifetime sex partners. The risk of transmission of HIV increases by 2-fold in the presence of TV, which is assumed to be due to local inflammation and disruption of the cervical epithelium.3 In the study performed by Aslan et al. [24], liquid-based Pap smears were found to be considerably more sensitive and specific than conventional Pap smearsin facilitating the identification of TV. The authors discovered that morphologic diagnosisof TV on LBC was extremely accurate,implying that patients may not need confirmation tests. Lara- Torre and Pinkerton observed that LBC smears have a sensitivity of 61.4 % and a specificity of 99.4 % for TV, and so the diagnosis of TV on the liquid- based preparations is more accurate and dependable, helping patients to be treatedwithout further testing [25].Leptothrix was discovered in 0.5 % of women in the present study. These segmented, lengthy, and filamentous organisms have a blue hue on Pap smears. The presence of Leptothrix is frequently relatedwith T. vaginalis[26]. A very few articles about this organism have been published so far. Furthermore, none of the papers published have evaluated the Pap smear'ssensitivity or specificity for this organism.In the current study, 5.4% of women had co-infection with mixed microbes. The most common mixed infection in our study was BV and VVC co-infection, which was detected in 2.4 % of cases. Similar result was obtained in other research of Nepal conducted by Bhargav et al. [18] Since two or more of these infections may coexist, the signs and symptoms may not necessarily be typical. There are conflicting findings that Candida albicansand BV have an inverseconnection. The environment of BV is assumed to be unsuitable for blastospore proliferation, hence fungal infection does not develop in the presence of BV [27].According to Souza et al. [28], the most prevalent bacterial flora associated with Candida spp. was lactobacilli (73.63%), followed by mixed flora (25.40 %), and rarely BV (0.73 %). However,other researchers have shown that women with VVC have concurrent BV infection similar to our findings [29, 30], indicating the assumption that Candida spp. and BV do not coexist or that Candida spp. grows only in a lactobacillary dominated flora with normal pH is untrue. Furthermore, Wei et al. [30] discovered that BV can coexist with blastospores (14.2%),compared to pseudohyphae in 35.4%, suggesting that pseudohyphae could cause a considerable alteration in bacterial flora. In a study by Pathak et al. [16], co-infection with BV and TV was discovered in only 2.8% of cases,which is similarto our findings (2.2%). According to a study published by Gatski et al. [31], BV and TV are the most prevalent infections diagnosed in HIV-positive women. Demirezen et al. and Heller at al. investigated the relationship of TV and BV on Pap smears [5, 32]. In their studies, 44.4% and 46.5% of TV-positive cases had BV, respectively. It has been proposed that TV elevates vaginal pH by lactobacilli phagocytosis [33], and this is the mechanism that helps BV to develop in the presence of TV. Similarly, Moodley et al. [27] have postulated that TV affectsvaginal flora, renderingwomen at risk for BV. This suggeststo an increased BV frequency in the presence of TV. In our analysis, vaginitis was most common in women aged 30-39 years (37.8%), with the highestnumber of patientshaving either single infection with BV and VVC or mixed infections. However, we observed TV most commonly in the women aged 40 to 49 years. In contradiction to our findings, Kumar et al. [9] discovered that the highestnumber of co- infection was found in the age group 41-50 years,whereas the maximum number of TV infection was identified in the age group 31-40 years. According to Bhargava et al. [18], women of reproductive age (20-29 years) had the highest number of vaginitis. The higher frequency of vaginitisin the 20-29 age range may be due to their high sexual exposureand, presumably, a higher tendency to change sexual partners in this age group.
Bacterial vaginosis is the most common infective vaginitis, followed by vulvovaginal candidiasis and trichomonal vaginitis. The women aged 30- 39 years are commonly affected. The present study shows the usefulness of cervical Pap smear in diagnosis of infective vaginitisother than epithelial cell abnormalities.
The smears which are negativefor intraepithelial lesion/malignancy with dense inflammation should be extensively evaluated to rule out infectious etiology as most of the time the infective organisms are obscured by inflammation. However, this problem has been lessened by liquid-based cytology, which removes background debris, hemorrhage, and significantly reduces inflammatory cells.
There are some limitations to this study. Since this was a hospital-based study, the sample size was relatively small and the participants did not represent a specific community. The time period of this study was also short. In addition, there are only a few past Nepalese research studies on the subject. To determine the true burden of infective vaginitis in Nepal, large-scale, multi-centric, and community-based investigations should be carriedout.
We appreciate the support of the technicians in our cytopathology department.
None
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
