
Case Report | DOI: https://doi.org/10.31579/2578-8949/027
*Corresponding Author: Ramachandran Rajagopal MD, Dept of Dermatology, Thumbay Hospital Dubai , United Arab Emirates.
Citation: Ramachandran Rajagopal MD , Ankur Malik MD , Balasaheb Kale DNB, Haripriya Pasala DGO. Linear IgA bullous dermatosis probably induced by pesticide. J. Dermatology and Dermatitis, DOI: 10.31579/2578-8949/027
Copyright: © 2018, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 February 2018 | Accepted: 14 March 2018 | Published: 20 March 2018
Keywords: Linear IgA bullous dermatosis (LABD), Vesiculobullous disorder, Cypermethrin, pesticide
A 31 year old lady presented with sudden onset mucosal erosions and multiple small vesicular lesions over trunk and fever which initially resembled varicella. However the lesions progressed to bullae with severe oral erosions, swelling of the mouth and involvement of upper and lower limbs over next five days. There was history of exposure to pesticide spray at the house two days prior to onset of lesions.
Skin biopsy and Direct Immunofluorescence revealed subepidermal blister with neutrophils and strongly positive IgA at dermoepidermal junction. A diagnosis of Linear IgA bullous dermatosis (Adult type) was made and patient rapidly responded to steroids. The case is reported for its rarity in adults and for the trigger in this case being possibly pesticide.
Linear immunoglobulin A (IgA) bullous dermatosis (LABD) is a rare autoimmune vesiculobullous disease with an incidence of 0.2 to 2.3 cases per million-population per year [1].
LABD has two clinical variants. In children, the disease is better known as chronic bullous disease of childhood (CBDC) with an average presentation occurring around 4.5 years [2]. In adults, two peaks are identified—teenage years and the sixties [3].
Induced LABD has been mostly due to drugs like vancomycin, Nonsteroidal anti-inflammatory drugs (NSAIDs), penicillins,cephalosporins, and angiotensin-converting-enzyme (ACE) inhibitors [4]. A case of LABD induced in a 31 year old lady by exposure to pesticide is reported.
A 31 year old lady presented with sudden onset of fever, severe oral ulceration and multiple blistering lesions over face and both upper and lower limbs of one week duration. Symptoms started two days after being exposed to cypermethrin pesticide spray in the house. She had slept in the house for four hours shortly after the pesticide spray had been completed. She had no preceding history of blistering disorders or similar disorders in the family. She was a mother of two children born normally and did not have any rash during pregnancy. She denied taking any drugs in recent past for any illness. She did not volunteer any hypersensitivity in the past towards insect repellents or environmental allergens. There was no history of permethrin spray done in the living areas previously.
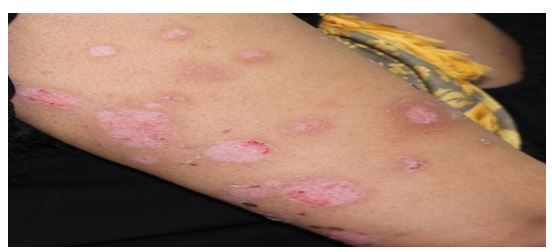
Dermatological examination revealed a febrile patient with multiple vesicles on upper part of back and upper arms and painful erosion of oral mucosa. At this point a provisional diagnosis of Varicella was considered and patient was advised oral antivirals. Three days later patient had developed multiple new vesicles around the mouth with swelling of face and lips and older vesicles over the upper back and arms had enlarged to become intact and tense bullae (Figures 1 & 2) with some areas resembling “cluster of jewels”. Blisters were painful and surrounding skin was inflamed. Redness and grittiness of both eyes were present. There was no scalp involvement, erosions, denudation or bleeding from the lesions. Nikolsky sign and bulla spread sign were negative.

Skin biopsy was sent for histopathology and direct immunofluorescence (DIF) with provisional diagnosis of Linear IgA bullous dermatosis. Treatment was started with parenteral steroids, as dapsone, the drug of choice in this condition was not readily available. Inj Hydrocortisone 100 mg 8 hrly IV was given for the first 48 hrs and then switched over to oral Prednisolone 60 mg daily for a week, tapering to 40mg for another week and then by 10mg every week. There was immediate response to steroids and the patient improved in 48 hours. She was then given oral steroids which were gradually tapered over 5 weeks. Lesions on skin and mucosa completely healed (Fig 6). There was no relapse during tapering the steroids or thereafter till date
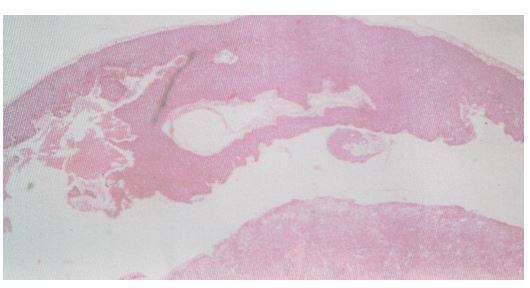
Histopathology confirmed the diagnosis of Linear IgA bullous dermatosis. It showed subepidermal blister filled with neutrophils (Figure 3)
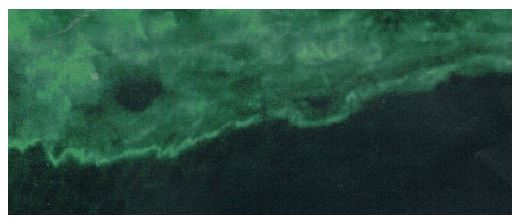
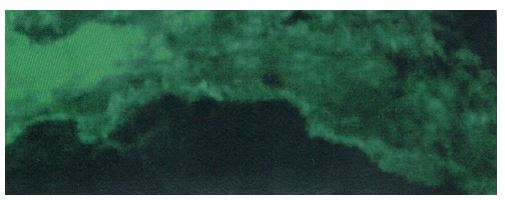
and strongly positive band of IgA in dermoepidermal junction on DIF (Figure 4). In addition to IgA, moderate positive DIF for IgG was also found at dermoepidermal junction (Figure 5). DIF was negative for IgM, C3, C1Q and fibrinogen.
The case is being reported for its rarity as incidence from various countries have ranged from 0.5 to 2.3 cases per million individuals per year [3]. It is slightly more common in China, Malaysia, Thailand and Sri Lanka. LABD usually occurs in children and when it rarely occurs in adults the patients affected are either in their teens or over 60 year of age. Age may vary in induced cases as this one. The patient was an Indian and belonged to the state of Tamil Nadu in South India.
Most cases in literature where pesticides have induced an autoimmune bullous disorder relate to pemphigus vulgaris .Diazinon spray and other organophosphates have been implicated causing pemphigus [6]. Occupational exposure to pesticides was significantly higher in patients with pemphigus (14.8%) than in controls (5.4%) [8]. LABD has been documented to be caused by contact with sodium hypochlorite [7]. Recent international survey has demonstrated that exposure to pesticides is actually associated with an increased risk of pemphigus by causing accumulation of acetylcholine at cholinergic receptors. Organophosphate pesticides, which are cholinesterase inhibitors,could favour the development, of acantholytic lesions, accounting for the direct association between exposure to pesticides and pemphigus [9]. Cypermethrin however is not an organophosphate compound and LABD is not an acantholytic disorder.
LABD triggered by cypermethrin, a pyrethroid, has not been reported till date to best of knowledge of the author. However the fact that pesticides trigger immune system malfunction in some way has been reported in cases of pemphigus [9].A similar malfunction could occur in genetically predisposed individuals who develop LABD on exposure to pesticide.
Clinical diagnosis is a challenge as it can resemble infectious disorders like varicella in early stages and other vesiculobullous disorders in late stages. Successful outcome of this disabling rare disorder depends on accurate diagnosis which is supported by skin biopsy findings. The gold standard for establishing a diagnosis of LABD is DIF. In DIF, there are linear deposits of IgA along the basement membrane at the DEJ. There may also rarely be coexistence of IgG, IgM, and C3.2 Both IgA and IgG were positive in the present case though IgA was strongly positive.
LABD has been reported in association with systemic diseases, such as autoimmune diseases like ulcerative colitis, Crohn’s disease, rheumatoid arthritis, psoriasis, and SLE [1]. There was no evidence of any of these in present case although she will be followed up for them. It may be unlikely to have such associations in induced cases of LABD.
The first line treatment for this condition is Dapsone, an immunomodulatory sulfone. However when dapsone is not available or cannot be given due to G6PD deficiency, steroids can be given.
Interesting features were its presentation like Varicella in the early stages, the unusual age of occurrence, presence of both IgA and IgG autoantibodies in the DIF at the dermoepidermal junction and the trigger being exposure to cypermethrin pesticide. It may be prudent to conclude that pesticide companies should advise their clients not to enter the house for first 24 hours after the spray and to inhabit the place only after the house is properly cross ventilated.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
