
Research Article | DOI: https://doi.org/10.31579/2640-1053/164
Research and Training Center ‘Physical and Chemical Materials Science’ Under Kyiv Taras Shevchenko University and NAS of Ukraine, Kiev, Ukraine.
*Corresponding Author: Anthony Kodzo-Grey Venyo. Research and Training Center ‘Physical and Chemical Materials Science’ Under Kyiv Taras Shevchenko University and NAS of Ukraine, Kiev, Ukraine.
Citation: Grey Venyo AK (2023), Leydig Cell Tumour of Testis and Scrotal Contents: A Review and Update, J. Cancer Research and Cellular Therapeutics, 7(5); DOI:10.31579/2640-1053/164
Copyright: © 2023, Anthony Kodzo-Grey Venyo. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 October 2023 | Accepted: 25 October 2023 | Published: 31 October 2023
Keywords: leydig cell tumour; testis; benign; malignant; diagnosis; histopathology; immunohistochemistry; electron microscopy; biopsy; radiology imaging; orchidectomy; frozen section biopsy; follow-up; lymph node dissection; tumour markers
It has been iterated that even though testicular cancers are relatively uncommon, and they account for only 1% to 2% of global male cancer diagnoses, it is the commonest malignancy in men who are aged between 15 years and 44 years. It has also been iterated that testicular tumours may originate from any of the cell types that are present within the testes and the on the whole fall into the two competing categories of germ cell tumours, of which approximately 95% of testicular cancer is comprised of, and sex cord-stromal tumours which constitute the remaining 5% of testis tumours in in adults. Out of the 5% of sex cord-stromal tumours, Leydig cell tumours are regarded to be commonest tumour which is derived from the same Leydig cells which normally reside within the interstitium of testis and secrete testosterone in the presence of luteinizing hormone. Leydig cell tumours of the testis are generally known to be benign tumours and only 5% to 10% being of Leydig Cell Tumours of the testis are considered to be malignant or portend malignant features. Leydig Cell Tumours of the testis have a bimodal distribution with peaks in the prepubertal age group and between the ages of 30 to 60. Apart from this Leydig Cell Tumours of the testis, had been reported in all age groups of males including young males and the over 90-yearl old male individuals sporadically. Due to Leydig cells' hormonally active properties, Leydig Cell Tumours might manifest with precocious puberty, breast tenderness, or gynecomastia, as well as infertility problems. Leydig cell tumours are derived from Leydig cells, which are histologically packed between the seminiferous tubules of the testis and they are physiologically responsible for testosterone secretion in response to luteinizing hormone. Apart from Leydig cell tumour afflicting the testis or rare occasions, Leydig Cell Tumour may also on very rare occasions afflict the epididymis. Leydig Cell Tumour of testis may manifest in different ways including: painless mass in the testis or intra-scrotal mass, precocious puberty, including early development of pubic hair as well as penile and musculoskeletal growth beyond that expected for the child’s age. Diagnosis of Leydig Cell Tumour of Testis whether benign or malignant is made based upon the histopathology examination and immunohistochemistry staining features of the tumour. Traditionally, Leydig cell tumours of the testis had been treated by the undertaking of radical orchidectomy based upon the provisional diagnosis of a malignant tumour only to find that the pathology examination of the orchidectomy specimen has confirmed features of Leydig Cell tumour of the testis which most often is benign. Radical orchidectomy alone has generally been curative for clinically benign Leydig cell tumours of testis. Testis-sparing surgery could be considered if the clinical suspicion of Leydig cell tumour is high, and pre-operative testicular serum tumour marker levels are within normal limits, and the size of the tumour is less than 2.5 cm. An intra-operative frozen section should always be undertaken to confirm benign Leydig Cell tumour of the tests, and a radical orchiectomy undertaken if the tumour is reported to be malignant. Leydig cell tumours of testis, do depict malignancy by metastasizing. About 10% of Leydig cell tumours in adults exhibit malignant biological behaviour. The only treatment for malignant Leydig cell tumour of testis is retroperitoneal lymph node dissection, in addition to the undertaking of radical orchidectomy due to the fact that they are known to be resistant to chemotherapy and radiotherapy. Because of the possibility of local recurrence of Leydig Cell Tumour of Testis, it is important for clinicians to ensure their patients undergo regular clinical and radiology imaging follow-up assessments for a long time.
Leydig cell tumours are rare tumours of the testis of the gonadal interstitium which may be hormonally active and which may lead to feminizing or virilising syndromes. Leydig cell tumours do comprise about 4% of adult testicular tumours [1] [2] and 3% of testicular tumours in infants and children. These Leydig Cell Tumours of testis could be pure tumours or they could be mixed tumours with other sex cord–stromal or germ cell tumours. Leydig cell tumours usually have a local manifestation; metastases of Leydig Cell Tumours had been stated to occur in about 2.5% of cases. [1] [2] The commonest sites for metastases are lymph nodes, lung, liver, and bones. [1,3] It has been pointed out that as with germ cell tumours, the route of spread of Leydig cell tumour of testis is via hematogenous and lymphatic spread to the retroperitoneal lymph nodes. Unlike germ cell tumours; nevertheless, it has been pointed out that Leydig cell tumours of testis and scrotal contents do portend a relative lack of sensitivity to radiotherapy and chemotherapy agents. [1,4]
Clinical presentations of Leydig cell tumour of testis include the following: [1]
Diagnosis of Leydig cell tumour of testis is confirmed by the histopathology and immunohistochemistry staining study features of the testis tumour. In cases of Leydig Cell Tumour of testis, Serum testosterone levels usually tend to raised; nevertheless, serum oestradiol levels might also be increased, especially when feminization is evident in the tumour. The results of the ensuing laboratory studies tend to be normal in patients who have pure Leydig cell tumours of testis: [1]
Ultrasound scan of scrotal contents and testis is stated to be a radiology imaging option which confirms the diagnosis, especially when clinical examination findings of patients are equivocal [1,5,6] Magnetic resonance imaging (MRI) scan could demonstrate small nonpalpable Leydig cell tumours which are not visible upon ultrasound scan. Computed tomography (CT0 scanning of the abdomen and chest radiography is stated to be indicated when malignancy is suspected. Radical orchidectomy was previously the primary treatment for Leydig cell tumours of testis, and radical orchidectomy remains in use for malignant cases. Nevertheless; the prognosis is poor for metastatic Leydig Cell tumour of testis and there are no standard treatment recommendations. Even though complete or partial remission following chemotherapy had been reported, it has been found ineffective in the majority of cases. [1,3] Testis-sparing surgery with the undertaking of enucleation of the mass is stated to be increasingly reported in the scenario of benign cases of Leydig cell tumour of testis, in both the adult and paediatric populations. [1,7,8] [9] It has been pointed out that when Leydig cell tumours of testis are diagnosed and treated early, testicle-sparing surgery had proven to be feasible and safe and could be regarded as first-line option of treatment. Nevertheless, because of the rarity of Leydig cell Tumour of testis, and non-availability of frozen section pathology examination facilities in many hospitals in the world, it would be envisaged that many cases of Leydig Cell tumours of the testis would continue to be diagnosed pursuant to the undertaking of radical orchidectomy based upon a provisional clinical diagnosis of malignant tumour of the testis. A high index of suspicion is required to establish a pre-operative diagnosis of Leydig Cell tumour of Testis. The ensuing article on Leydig Cell Tumour of testis and Scrotal contents has been divided into two parts: (A) Overview which has discussed general miscellaneous aspects of Leydig Cell Tumour and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, And Some Studies related to Benign and Malignant Leydig Cell Tumours of Testis and Epididymis.
To review and update the literature on Leydig Cell Tumour of Testis and Epididymis.
Internet data bases were searched. The search words that were used included: Leydig cell tumour of testis; Testicular Leydig cell tumour; Leydig cell tumour of testes; Intra-scrotal Leydig cell tumour; Leydig cell tumour of epididymis; and epididymal Leydig cell tumour. Seventy-one (71) references were identified which were used to write the article which has been divided into two parts: (A) Overview which has discussed miscellaneous general aspects of Leydig Cell Tumour and (B) Miscellaneous Narrations and Discussions from some case reports, case series and some studies related to Leydig tumour of testis and epididymis in human beings.
Definition / General Statements Related to Leydig Cell Tumour of Testis
The ensuing generation statements had been made related to Leydig Cell Tumour of testis: [10]
• Leydig cell tumour of testis is the commonest sex cord stromal tumour of the testis and Leydig Cell Tumour of Testis is comprised of cells simulate non-neoplastic Leydig cells.
• It has been iterated that a small minority, comprising of less than (<) 10% of cases of Leydig Cell Tumours of testis are clinically malignant. [11,12]
Essential features
The essential features of Leydig Cell Tumour of testis had been summated as follows: [10] • Leydig cell tumour of testis is the commonest sex cord stromal tumour of the testis.
• Histology examination of specimens of Leydig Cell Tumour of testis does demonstrate the following: diffuse / nodular growth of polygonal cells with abundant eosinophilic cytoplasm, uniform round nuclei and prominent central nucleoli; Reinke crystals may be found to be present within the tumour.
• Immunohistochemistry staining studies of Leydig Cell Tumour of testis does demonstrate the following: The tumour upon immunohistochemistry staining studies exhibit positive staining for the ensuing tumour markers as follows: o inhibin A+, o calretinin+, o MelanA+, o SF1+, o AR+
• Features of Leydig Cell Tumour of testis that are associated with malignant potential include the following: o Size of tumour greater than (>) 5 cm, o Infiltrative borders of the tumour, o Evidence of cytological atypia upon pathology examination of the tumour. o Presence of frequent mitoses within the tumour greater than (>) 3 mitoses within (/) 10 high power fields o Vascular invasion of the tumour, o Necrosis within the tumour
• Treatment: o Surgical resection of the testicular tumour is regarded as the standard treatment of Leydig Cell Tumour of testis and surgical resection of Leydig cell tumour of testis is regarded as curative for non-metastasizing Leydig cell tumours of testis.
• Prognosis of Leydig Cell Tumour of Testis: o It has been iterated that the overall 5-year survival following the undertaking of orchidectomy for Leydig Cell Tumour of testis is higher than (>) 90% Terminology
• Another term that is utilized for Leydig cell tumour of testis is interstitial cell tumour of testis; but this name is iterated to be an obsolete terminology [10] Epidemiology The epidemiology of Leydig Cell Tumour of testis has been summated as follows: [10]
• It has been documented that Leydig cell tumour of testis does constitute 1% to 2% of testicular tumours in adults and 3% to 6% of testicular tumours in prepubertal males [13,14]
• Leydig Cell Tumour of testis is mostly sporadic found or reported, and Leydig Cell Tumour is rarely associated with hereditary leiomyomatous and renal cell carcinoma syndrome [15]
• Leydig cell tumour of testis does tend to occurs at any age with 2 peaks that are reported in the 5 years to 10 years group and in the 30 years to 60 years group of patients. [13]
Sites
The sites within the testis that tend to be afflicted by Leydig Cell Tumour of testis include the following: [10]
• The parenchyma of the testis.
• On rare occasions, Leydig cell tumour tends to be found within ectopic rests of Leydig cells in the epididymis. [16]
Pathophysiology
Prognostic factors
The prognostic factors of Leydig Cell Tumours of the testis had been summated as follows: [10]
Treatment
The treatment of Leydig Cell Tumour of the testis has been summarized as follows: [10]
Gross macroscopy Examination Features.
The macroscopy examination features of Leydig Cell Tumour of the Testis, had been summated as follows: [10]
Frozen section description of Leydig Cell Tumour of Testis
The frozen section examination features of Leydig Cell Tumour of Testis had been summarized as follows: [10]
Microscopy (histopathology) examination features of Leydig Cell Tumours of Testis description
The microscopy (histopathology) examination features of Leydig Cell Tumours of Testis had been summarized as follows: [10]
Microscopy histopathology examination of Leydig Cell Tumour of Testis does demonstrate the ensuing patterns:
Cytology examination features of Leydig Cell Tumour of the Testis had been summarized as follows: [10]
Cytology description
The cytopathology examination features of Leydig tumour of the testis had been summarized as follows: [10]
Positive Immunohistochemistry stains
It has been iterated that Leydig Cell Tumours of the Testis Cells do exhibit positive immunohistochemistry staining for the following markers: [10]
Negative Immunohistochemistry stains
It has been iterated that Leydig Cell Tumours of the Testis Cells do exhibit positive immunohistochemistry staining for the following markers: [10]
Electron microscopy description
The electron microscopy examination features of Leydig Cell Tumour of Testis had been summarized as follows: [10]
The molecular and cytogenetics examination features of Leydig Cell Tumour of Testis had been summarized as follows: [10]
Differential diagnosis
The differential diagnoses of Leydig Cell Tumour of Testis had been summated as follows: [10]
Testicular tumour of adrenogenital syndrome or testicular adrenal rest tumours:
Leydig cell hyperplasia:
Granular cell tumour.:
Large cell calcifying Sertoli Cell Tumour. [10]
Malakoplakia: [10]
Seminoma: [10]
[B] Miscellaneous Narrations and Discussions from Some Scase Reports, Case Series, And Studies Related to Leydig Cell Tumours of Testis.
Ruf et al. [11] stated that Leydig-cell tumours (LCT) of the testis are poorly understood clinically. Ruf et al. [11] analysed the clinical characteristics of LCT in a large patient sample and compared their findings with corresponding data of germ-cell tumours (GCT). Ruf et al. [11] reported that in a sample of 208 patients who had been treated during between 1995 and 2017 in 33 institutions, the following characteristics were registered: age, manifesting symptoms, primary tumour size, testis-sparing surgery (TSS) or orchidectomy, malignancy, laterality, medical history, and outcome. Ruf et al. [11] reported that their data analysis included descriptive statistical methods and logistic regression analysis. Ruf et al. [11] summarized the results as follows:
Ruf et al. [11] made the ensuing conclusions:
Pozza et al. [19] undertook a study in order to understand their question regarding when should 'not so rare' Leydig cell tumours (LCTs) of the testis be suspected, diagnosed, and treated? Pozza et al. [19] iterated the ensuing summations related to their study:
With regards to the Study design, size, and duration, Pozza et al. [19] reported that a case-cohort study of consecutive patients who were diagnosed with LCTs over a 10-year period was prospectively enrolled from 2009 to 2018 and they were compared to matched cohorts of patients with seminomas or no testicular lesions that were screened in the same timeframe. Relating to the participants/materials, setting, methods, Pozza et al. [19] reported the following:
Pozza et al. [19] summated the main results of their study and the role of chance as follows:
Pozza et al [19] also stated the ensuing:
Abe et al. [37] reported a 33-year-old man who was referred to their hospital for male infertility with painless swelling of his left scrotal content. He underwent a left high orchidectomy was based upon a diagnosis of left testicular tumour. Histologically, the testicular mass was a Leydig cell tumour.
Shiraishi et al. [38] stated the following:
Shiraishi et al. [38] reported a case study of a Leydig cell tumour in a single testis manifesting as male infertility. Shiraishi et al. [38] reported A 38-year-old male who was referred to their hospital because of a tumour within his right testis. He had undergone left orchidectomy when he was one year old because of a testicular tumour. During an examination related to his infertility, he had ultrasound scan which had demonstrated a 1 cm tumour. His serum tumour markers were all within normal ranges. The results of his hormonal examination showed that the results of his serum luteinizing hormone (LH) 30.3 mIU/ml (1.5-12.4) and follicle stimulating hormone (FSH) 11.9 mIU/ml (1.7-8.6) were higher than the normal limits, but his serum total testosterone (total T) and oestradiol (E2) were within normal ranges. He underwent firstly, testicular tumour enucleation, and then testicular sperm extraction (TESE) was undertaken from a macroscopically normal site of the testis. Histopathology examination diagnosis of the testis tumour as a benign Leydig cell tumour encompassed by Leydig cell hyperplasia. For 12 months following his operation there had not been any recurrence of his testis tumour. Even though his high serum LH and FSH had persisted, his serum total T and E2 were within normal ranges. Komai et al. [39] reported a case of Leydig cell tumour of the post-pubertal cryptorchid testis with the main manifestation of male infertility. Komai et al. [39] reported a 36-year-old man who had consulted another clinic and his semen analysis had demonstrated oligospermia. A solid mass was found palpable within his right inguinal undescended testis. He was referred to the hospital of Komai et al. [39] for treatment of the testicular tumour. He underwent a right inguinal orchidectomy and pathology examination diagnosis was Leydig cell tumour with no malignant findings. After the surgery improvement was seen in his semen analysis. There was no evidence of recurrence of his tumour 9 months after surgery. Madina Pérez et al. [40] reported a case of Leydig cell tumour in a cryptorchid testis. Medina Pérez et al. [40] reported a 55-year-old man who had presented with no specific scrotal symptoms. A cryptorchid testis was found upon his clinical examination and the patient underwent orchidectomy. During his operation, a solid, well-circumscribed, round nodule of 0.8 cm in diameter was found in an atrophic testis. Histopathology examination of the tumour showed a Leydig cell tumour with crystals of Reinke and immunostaining with vimentin. Efthimiou et al. [41] 72-year -old man who had manifested with a 2-month history of painless left testicular enlargement. In the past, he had had undergone orchidopexy of the contralateral testis for cryptorchidism. His clinical examination demonstrated an irregular hard swollen left testis and a small right one. He did not have any gynecomastia. The results of his serum tumour markers (Alpha-fetoprotein, human chorionic gonadotropin, and lactate dehydrogenase) were negative for malignancy. He had ultrasound scan of testes which demonstrated an 11 cm × 6-cm nonhomogeneous testicular mass with multiple hypoechoic nodules. Metastases were not evident in the staging investigations. He underwent a left radical orchidectomy. Histopathology of the specimen demonstrated malignant LCT. Immunohistochemistry was positive for inhibin A, and Ki-67, and immunohistochemistry staining studies of the tumour had shown that the tumour was negative for pancytokeratin, cytokeratins AE1/AE3, cytokeratins 8/18, epithelial membrane antigen, carcinoembryonic antigen, alpha-fetoprotein, human chorionic gonadotropin, vimentin, CD30, and actin. His post-operative hormone profile demonstrated hyper-gonadotropic hypogonadism. The patient was placed on testosterone substitution treatment and retroperitoneal lymph node dissection was suggested, but he refused to undergo any further operation.
Michalec et al. [42] stated the following:
Michalec et al. [42] reported the rare case of leydigioma in 71-year-old man with unilateral cryptorchidism. Michalec et al. [42] stated that only a few cases had been reported as arising from undescended testis.
Taguchi et al. [43] reported an 85-year-old man who had visited their hospital with a complaint of painless swelling of his right testis. He underwent a right high orchiectomy under the diagnosis of right testicular tumour. Histopathology examination of the right testicular tumour specimen confirmed the diagnosis of Leydig cell tumour. Taguchi et al. [43] stated that they had reviewed 86 cases of this tumour that had been previously reported in Japan and to their knowledge, their patient is the oldest one who had been treated in Japan. Harada et al. [44] reported a 63-year-old man who had visited their hospital with a symptom of painless swelling of his left scrotum. He underwent left trans-inguinal high orchidectomy since he had ultrasound scan which had suggested a testicular tumour. Histologically, the testicular mass was a Leydig cell tumour of testis. Sugimoto et al. [45] reported a 40-year-old man who was referred to their hospital with gynecomastia and painless swelling of his right scrotum. He had ultrasound scan which demonstrated 15 mm x 10 mm mass with low echogenicity within his right testis. He underwent right high orchidectomy. Histologically, Reinke's crystals and capsular invasion by tumour cells were found. The final diagnosis, the tumour was a malignant Leydig cell tumour of the testis. Bertola et al. [46] stated that Leydig cell tumours (LTC) are uncommon neoplasms that arise from gonadal stroma which account for 1% to 3% of all testicular tumours. Bertola et al. [46] reported a case of LCT in a 36-year-old man who had been suffering from painful bilateral gynecomastia for one year. The results of his endocrine function tests showed decreased gonadotropin concentrations, and reduction of testosterone/oestradiol ratio. He had ultrasound scan which revealed a 10 mm to 12 mm hypoechoic area within his right testis, which was not evident upon his clinical examination. He underwent right orchidectomy and histological examination of the orchidectomy specimen confirmed the supposed existence of an LCT. After surgery, the gynecomastia had completely disappeared, and his hormonal alterations had returned to normal. Dounis et al. [47] reported a man had manifested with left painful breast enlargement and impotence as his main complaints of a right cryptorchid young man. He underwent ultrasound scan which demonstrated a hypoechoic mass which was found in his right testis. He underwent right orchidectomy and post-operatively the increased level of his serum oestrogens and the decreased levels of testosterone were normalized 6 months following his orchidectomy, his gynecomastia had subsided considerably, and his impotence had improved quite satisfactorily. De Jong et al. [48] reported one case of a bilateral testicular Leydig cell tumour in a man of 29 years old. They stated that there are few cases of such tumours which had been reported in the literature and that Gynecomastia forced the patient to consult his doctor. His hormonal profile was found to be practically normal; nevertheless, his serum oestradiol level was at the limit superior of normal range, and his serum testosterone level was at the limit inferior (lower range). His testicular palpation was normal. He had scrotal ultrasound scan which confirmed the diagnosis of testicular tumour. They recommended that scrotal ultrasound scan should be performed in every patient who has unexplained gynecomastia. There was no metastasis in the reported patient. Before the treatment, the patient’s sperm conservation was performed (his sperm was normal). The reported surgical treatment sequence for the patient who did not have a child was the next one as follows: 1. inguinal orchidectomy was undertaken at the side of bigger tumour. Histological diagnosis was the benign Leydig cell tumour; 2. one month later, an inguinal orchidotomy at the other side was undertaken and the palpable tumour of 9 mm was removed. The extemporaneous biopsy confirmed the same diagnosis as at the other side; 3. one year later, there is no evidence metastasis, and the woman of the reported patient became pregnant. Carmignani et al. [9] undertook a long-term evaluation of conservative surgical treatment of benign Leydig cell tumour. Carmignani et al. [9] performed a multi-centre retrospective clinical study at 6 European centres. They examined case files of all patients who were diagnosed as having Leydig cell tumour and treated with conservative surgery. Patients underwent clinical examination, hormone and tumour marker assays, scrotal and abdominal ultrasound, chest x-ray, and an endocrinological examination. Carmignani et al. [9] summarized the results as follows: From 1987 to 2006, 22 patients who had Leydig cell tumour had undergone conservative surgery. The mean patient age of the patients was 35 years and the ages of the patients had ranged between 5 years and 61 years. The mean follow-up of the patients was 47 months and the follow-up of the patients had ranged between 1 month and 230 months. No local recurrence or metastasis was found. The patients presented with symptoms as follows: a palpable testicular nodule in 3 patients, that amounted to 13.7% of the patients or a nodule which was diagnosed by ultrasound scan on 15 patients, that amounted to 68.2% of the patients, gynecomastia by 2 patients, which amounted to 9.1% of the patients, precocious pseudo-puberty by 1 patient, which amounted to 4.5% of the patients, or scrotal pain by 1 patient, which amounted to 4.5% of the patients. Three patients were monorchid after their undergoing of contralateral orchidectomy for inguinal hernia repair (1 patient, 28 years before surgery) and nonseminomatous germ cell tumour (2 patients, 1 month and 6 years before surgery). The diagnosis after frozen section biopsy examination of the testis specimen was Leydig cell tumour in 20 of 22 cases that amounted to 91.0% of the cases. The mean histological size of the nodule was 1.11 cm, and this had ranged from 0.5 cm to 2.5 cm. Preoperative serum FSH and LH levels were high in 4 patients. Serum tumour marker levels were normal before and after surgery. Follow-up was undertaken for all patients every 3 to 6 months with clinical examination, tumour marker levels assessments, scrotal and abdominal ultrasound scan, chest x-ray. Six patients which amounted to 27.3% of the patients underwent abdominal computerized tomography. Carmignani et al. [9] made the following conclusions:
Giannarini et al. [49] stated that even though majority of Leydig cell tumours are benign, radical orchidectomy at the time of publication of their article in 2007 was considered the standard therapy. Giannarini et al. [49] retrospectively analysed the long-term follow-up of a series of patients who had Leydig cell tumours who were electively treated with testis sparing surgery. Giannarini et al. [49] reported that between November 1990 and December 2005, 17 consecutive patients with Leydig cell tumours had undergone testis sparing surgery on an elective basis. The pre-operative evaluation of the patients included clinical examination, serum markers for germ cell tumours, scrotal ultrasound, abdominal computerized tomography, chest x-ray and hormonal profile if clinically required. Testis sparing surgery was undertaken through an inguinal approach with spermatic cord clamping. Frozen section examination was undertaken in all cases, which had revealed Leydig cell tumours. Follow-up of the patients consisted of clinical examination, scrotal ultrasound scan, abdominal computerized tomography and chest x-ray every 6 months for the first 2 years, then annually. Tumour recurrence and survival were evaluated. Giannarini et al. [49] summarized the results as follows:
Giannarini et al. [49] concluded that in patients with Leydig cell tumours testis sparing surgery with frozen section examination does provide an excellent long-term oncological outcome. Vergho et al. [50] compared retrospectively the outcome of testis-sparing surgery (TSS) to radical orchiectomy (RO) in patients who had Leydig cell tumour (LCT). About the methods of their study, Vergho et al. [50] reported that between 1992 and 2008, 16 patients with LCT of the testis were identified. All but 1 tumour could be identified by ultrasonography. Alpha-fetoprotein and beta-human chorionic gonadotropin levels were normal in all patients. Eight patients had undergone RO and their mean age during their surgical operation was 42 years and their ages at the time of their surgery had ranged between 27 years and 61 years; the median tumour size was 12.9 mm and the tumour size had ranged between 10 mm and 25 mm. and the remaining 8 patients underwent TSS and their mean age at surgery was 34 years and their ages had ranged between 18 years and 49 years; the median tumour size was 8.6 mm and the tumour size had ranged between 4 mm 23 mm. Staging (abdominal computed tomography and chest x-ray or thoracic computed tomography) was negative in all patients. , Vergho et al. [50] summarized the results as follows:
Vergho et al. [50] concluded that in the medium term, TSS is a safe procedure in patients with LCT that measure less than 25 mm. Laclergerie et al. [51] compared the oncological outcomes of testicle-sparing surgery (TSS) and radical orchiectomy (RO) in patients who had Leydig cell tumour (LCT) of the testis. Laclergerie et al. [51] undertook a multi-centre retrospective clinical study within 12 centres in France. All the patients who had histologically proven LCT were included and analysed according to treatment (organ-sparing surgery or radical orchiectomy). The patients had undergone preoperative clinical, biological and imaging assessment. Demographic, clinical, and pathological variables were collected at baseline and compared between the groups according to surgical treatment. Follow-up was calculated utilizing the reverse Kaplan-Meier estimation and was updated at the end of 2015. Laclergerie et al. [51] summarized the results as follows:
Laclergerie et al. [51] concluded that long-term follow-up had indicated that testicle-sparing surgery does not compromise relapse-free survival in the treatment of Leydig cell tumour of the testis.
Loeser et al. [52] compared retrospectively the outcome of testis-sparing surgery (TSS) to radical orchiectomy (RO) in patients who had Leydig cell tumour (LCT). Loeser et al. [52] reported that between 1992 and 2008, 16 patients who had LCT of the testis were identified. All but 1 tumour could be detected by ultrasound scan of scrotum and scrotal contents. Alpha-fetoprotein and beta-human chorionic gonadotropin levels were normal in all patients. Eight patients underwent RO and their mean age at surgery was 42 years and their ages had ranged between 27 years and 61 years; the median tumour size was 12.9 mm and the tumour size had ranged between 10 mm and 25 mm and the remaining 8 underwent TSS and their mean age at surgery 34 years as well as their ages had ranged between 18 years and 49 years; the median tumour size was 8.6 mm and the size of the tumour had ranged between 4 mm and 23 mm. Staging (abdominal computed tomography and chest x-ray or thoracic computed tomography) was negative in all patients. Loeser et al. [52] summarized the results as follows:
Canda et al. [53] reported their experience in performing testis sparing surgery (TSS) to treat sequential bilateral testicular tumours. Canda et al. [53] undertook TSS on two patients with bilateral sequential testicular tumours. Canda et al. [53] summarized the results as follows: A 43-year-old patient (Case 1) and a 33-year-old patient (Case 2) had previous inguinal orchidectomy for seminoma. The patients were diagnosed as having secondary testicular tumours within the contralateral testes on follow up. They were treated by means of TSS after frozen section analysis of the peritumoral testicular tissue. Pathology examination of the excised tumours demonstrated immature teratoma and Leydig cell tumour. Both patients were disease free without local recurrence and did not have erectile dysfunction, and thus did not require androgen replacement therapy after a follow up of 6 months and 44 months, respectively. Canda et al. [53] concluded that TSS after frozen section analysis appears to be a safe and feasible procedure that, in carefully selected cases, offers adequate cancer control, preserves sexual function, and provides psychological benefits.
Bozzini et al. [54] iterated that the gold standard treatment for Leydig cell tumours (LCTs) is still considered to be radical orchidectomy, but testis sparing surgery (TSS) in conjunction with intraoperative frozen section (FSE) had been recently attempted with promising results. Bozzini et al. [54] identified studies by searching electronic databases. A bibliographic search covering the period from January 1980 to December 2012 was conducted utilizing PubMed/MEDLINE and EMBASE database. Bozzini et al. [54] excluded studies if they were single case reports, meeting abstracts and conference proceedings. Bozzini et al. [54] stated that their analysis was based upon a total of 13 studies which had fulfilled the predefined inclusion criteria. A total of 247 participants were included in the 13 studies examined in their systematic review. 145 cases were treated with radical orchiectomy and 102 with TSS. In the radical surgery group, the follow-up had varied from 6 months to 249 months. In the TSS group, the follow-up had varied from 6 months to 192 months. Frozen section was undertaken in a total of 96 patients. Sensitivity was 87.5%. None of the patients treated with TSS had manifested a metastatic recurrence, while in patients treated with radical orchiectomy three patients had manifested with metastatic recurrence. Bozzini et al. [54] stated that in selected cases radical surgery appeared excessive and the potential for a shift to TSS as the standard management is gathering momentum. Bozzini et al. [54] made the following conclusions:
Kong et al. [55] stated the following:
Kong et al. [55] reported a patient with azoospermia, a testicular Leydig cell tumour (LCT), and elevated plasma testosterone levels. Kong et al. [55] described the diagnostic and therapeutic experience of this case, and their follow-up of the patient's clinical indicators and fertility status. Kong et al. [55] reported that the patient was diagnosed with azoospermia and a testicular LCT. The patient underwent testicular tumour excision and long-term follow-up. After 4 months of follow-up, the patient's semen examination index had significantly- improved and his wife became naturally pregnant. At 4 months of gestation, the foetus was delivered because of a ruptured amniotic cavity. Twenty-six months after tumour removal, the patient's sex hormone levels had completely returned to normal and spermatogenic function had partially recovered, but there was no natural pregnancy with his partner. Kong et al. [55] made the ensuing conclusions:
Luckie et al. [14] stated the following:
Luckie et al. [14] reported on 12 children with LCT within 3 institutions between 2000 and 2016. Luckie et al. [14] reported that the manifesting symptoms of LCT included precocious puberty, palpable testicular mass, and scrotal swelling. Radical orchidectomy was undertaken in 9 patients. Three patients were treated with enucleation. All patients were alive at their last follow-ups without evidence of local recurrence or metastasis.
Carvajal-Carmona et al. [15] stated the following:
Carvajal-Carmona et al. [15] investigated the role of FH mutations in predisposition to LCTs. Carvajal-Carmona et al. [15] tested for pathogenic effects of the N64T mutation and screened an additional 29 unselected adult LCTs for FH alterations. Carvajal-Carmona et al. [15] also tested these LCTs for mutations in two genes, the LH/choriogonadotropin receptor (LHCGR) and the guanine nucleotide-binding protein alpha (GNAS) that had been implicated in LCT tumorigenesis. Carvajal-Carmona et al. [15] summarized the results as follows:
Carvajal-Carmona et al. [15] concluded that their study had shown that some LCTs are caused by FH mutations and represented one of the first reports of germline mutations within any type of adult testicular tumour.
Huang et al. [16] stated the following:
Huang et al. [16] reported a case of primary epididymal LCT in a 41-year-old Chinese man. The patient manifested with right epididymal swelling for 3 months without endocrine manifestations, including gynaecomastia and decreased libido. He had ultrasound scan of his scrotal contents which demonstrated a mass that measured about 1.5 cm in diameter entirely within the cephalic region of his right epididymis. No abnormality was found within his bilateral testes. The patient underwent total mass resection without any post-operative treatment. Histological examination of the excised mass had demonstrated that the well-circumscribed tumour was separated by conspicuous hyalinised fibrous stroma; the tumour cells were noted to be large and polygonal with round nuclei and abundant eosinophilic cytoplasm. Immunohistochemistry staining studies of the tumour demonstrated that phenotypically, the tumour cells had expressed four markers of sex cord differentiation which included: calretinin, melanA, CD99 and inhibin. There was no recurrence at his 2-year follow-up. Huang et al. [16] also stated the ensuing:
Al-Agha and Axiotis [17] stated the following:
Rossato et al. [56] made the ensuing iterations:
Rossato et al. [56] undertook a retrospective study evaluating the clinical and histopathological characteristics of 13 patients who were surgically treated for testicular tumour and diagnosed to be afflicted by Leydig cell tumour (LCT). Rossato et al. [56] stated that it was possible to retrieve the archived paraffin embedded tumour together with neighbouring healthy testicular tissue of all subjects who were affected by LCT (12 benign and 1 malignant form), that were analysed for INSL-3 expression. Immunohistochemistry staining studies of the tumour sections of the 13 patients affected by LCT had demonstrated constitutive expression of INSL3 protein within all LCT, irrespective of the histological pattern of each LCT and with no significant differences of staining intensity between all tumours. Particularly, no gross differences were observed between the staining for INSL3 in the 12 benign LCTs and the only one showing malignant clinical behaviour. Rossato et al. [56] made the ensuing discussing iterations:
Pozza et al. [19] undertook a study which was aimed to answer when should 'not so rare' Leydig cell tumours (LCTs) of the testis be suspected, diagnosed, and treated. Pozza et al. [19] stated the following:
Pozza et al. [19] reported a case-cohort study of consecutive patients who were diagnosed with LCTs over a 10-year period who were prospectively enrolled from 2009 to 2018 and compared to matched cohorts of patients with seminomas or no testicular lesions screened in the same timeframe. Pozza et al. [19] reported that out of the 9949 inpatients and outpatients who had been referred for scrotal ultrasound scans, a total of 83 men with LCTs were included. Pozza et al. [19] reported that the enrolled subjects had undergone medical history and clinical examination and they were asked to undergo routine blood tests, hormone investigations (FSH, LH, total testosterone, oestradiol, inhibin B, sex hormone-binding globulin (SHBG), prolactin), and semen analysis. Patients who consented also underwent contrast-enhanced ultrasound, elastography, gadolinium-enhanced scrotal magnetic resonance imaging, and hCG stimulation test (5000 IU i.m.) with serum total testosterone and oestradiol measured at 0, 24, 48, and 72 hours. Pozza et al. [19] summarized the results as follows:
Kim et al. [21] analysed the clinical and pathological features of 40 Leydig cell tumours of the testis. The ages of the patients had ranged from 2 years to 90 with an average age of 46.5 years of age. The commonest initial presentation of the patients was testicular swelling, which was at times associated with gynecomastia; 15% of the patients had manifested because they had gynecomastia and they were found to have palpable testicular tumours. All three children were brought to the physician because of the finding that they had isosexual pseudo-precocity. The tumours, one of which was asynchronously bilateral, had ranged from 0.5 cm to 10.0 cm (with an average size of 3 cm) in greatest diameter. They were usually well circumscribed, however, in seven of them the margin with the adjacent testis was noted to be ill-defined. Upon microscopy examination the commonest pattern was that of diffuse sheets of neoplastic cells, but insular, trabecular, pseudo-tubular, and ribbon-like patterns were also found. The neoplastic cells were noted to be most often large and polygonal with abundant eosinophilic, slightly granular cytoplasm; occasionally the cytoplasm was found to be abundantly vacuolated. In eight of the tumours some of the cells were found to be spindle-shaped, and in six of the tumours some had scanty cytoplasm. Crystalloids of Reinke were found in 35% of the tumours. Conspicuous nuclear atypicality was present in 12 tumours and the mitotic rate had ranged from less than 1 to 32 per 10 high-power fields. Blood vessel invasion, lymphatic invasion, or both were noted in four tumours. Follow-up information of 2 months to 22 years, with an average follow-up of 4 years was available for 30 patients. Five of the patients died as a result of spread of their tumour. A comparison of the clinically malignant tumours with those that were associated with survival for 2 years or longer than 2-years post-operatively had revealed that the former occurred in older patients and they were accompanied by symptoms of shorter duration and an absence of endocrine presentations. The malignant tumours were larger, often they had an infiltrative margin and they had spread beyond the confines of the testis, they frequently exhibited blood vessel or lymphatic invasion, and had a greater degree of cellular atypia and necrosis and a higher mitotic rate than the benign tumours.
Fankhauser et al. [22] stated the following:
Fankhauser et al. [22] analysed published case series data on Leydig cell tumours. They assessed the association between clinicopathological variables and the presence of metastatic disease was assessed using regression analyses. Fankhauser et al. [22] summarized the results as follows
Fankhauser et al. [22] made the ensuing conclusions:
Mukhopadhyay et al. [57] reported A 6-year-old boy presented with precocious puberty (see figure 1). He had isotope scan, which had demonstrated that his bone age was greater than (>) 12 years and less than (<) 14 years. He had ultrasound scan which demonstrated a heterogeneous echogenic space-occupying lesions which had involved the whole of his left testis with many micro- and macrocalcification and increased vascularity. The volume of his left testis was 12 cc. He had hormonal assay which showed his serum luteinizing hormone (LH) levels was <0.07 U; normal human chorionic gonadotropin level <1 mIU/ml; alphafetoprotein (AFP) level 0.97 IU/ml; serum testosterone 17.9 nmol/L; and serum cortisol, adrenocorticotropic hormone, and 17 OH progesterone level were 8.86 μ/dl, 37.9 pg/ml, and 31.56 ng/ml, respectively. All the levels of his hormonal studies were within normal limits except his serum testosterone levels that were raised. He had computed tomography (CT) scan of abdomen which was normal. The patient underwent orchidectomy. Grossly, the testis with scrotum measured 5.5 cm × 3.5 cm × 2.5 cm, testis was 4 cm × 3 cm × 2 cm, and the attached spermatic cord was 5.5 cm in length. Cut section had shown lobulated, yellow wellcircumscribed mass (see figure 2). Upon microscopy pathology examination, the sections showed polygonal cells with abundant eosinophilic cytoplasm and prominent nucleoli which were arranged in sheets and nodular pattern (see figure 3). Pleomorphism was noted to be present in some places. Immunohistochemical staining of the tumour with calretinin was undertaken and this showed positive staining of the tumour (see figure 4). Diagnosis of benign LCT was made based upon his clinical, hormonal, pathological, and immunohistochemical study findings.

Figure 1: Gross picture of lobulated yellow well-circumscribed mass. Reproduced from: Reproduced from: [57] under Copyright: © 2017 Journal of Indian Association of Pediatric Surgeons. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.

Figure 2: Polygonal cells with abundant eosinophilic cytoplasm, prominent nucleoli (x 400). Reproduced from: [57] under Copyright: © 2017 Journal of Indian Association of Pediatric Surgeons. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.

Figure 3: Immunohistochemistry positivity for calretinin (x 400). Reproduced from: [57] under Copyright: © 2017 Journal of Indian Association of Pediatric Surgeons. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Zeuschner et al. [58] stated that Gynecomastia is a common incidental finding in males which can be caused by a variety of benign or malignant diseases and that in rare cases, it results from Leydig cell tumours, which is an uncommon clinical entity that accounts for 3% of all testicular tumours. Zeuschner et al. [58] also iterated that some of them are hormonally active but they rarely cause symptomatic endocrine disturbance. Zeuschner et al. [58] reported a 32-year-old man who had presented with gynecomastia which he had already been suffering from for the preceding two years. Even though he had been seen by three other specialists, including a urologist, none of them had identified the small mass in the upper pole of his right testis. Zeuschner et al. [58] decided to undertake testis-sparing surgery which confirmed the diagnosis of a hormonally active Leydig cell tumour. During follow-up, his hormonal status normalized, and his gynecomastia began to resolve. Genov et al. [59] reported that in April 2019, a 45-year-old man was admitted to their Urology department with a large painless mass within his right testis of 1 year duration. The patient stated that one month preceding his admission, the lesion had commenced to grow. On his clinical examination, his right testis was found to measure 6.5 cm × 3.0 cm in size, with a palpable tumoral mass of about 3.5 cm × 2.0 cm in size, also the patient had a regular pulse of 78 beats/min, a temperature of 36.9 °C, as well as a respiratory rate of 18 -breaths per minute. No other signs were found, including gynecomastia or swelling of superficial lymph nodes. His penis and pubic hair were normally developed. The results of the patient’s laboratory blood tests such as complete blood cell count, renal function tests, liver function tests, and urinalysis were within normal ranges. The results of his serum tumour markers including: alpha-fetoprotein (AFP), β-human chorionic gonadotropin (β-hCG) and lactate dehydrogenase (LDH) were negative, and his hormonal investigations like serum testosterone, prolactin and follicle stimulating hormone (FSH) were within normal ranges. He underwent ultrasound scan assessment which revealed a mixed echogenic space occupying lesion which had involved half of his right testis with increased vascularity and some cystic areas. The patient underwent trans-inguinal radical high right orchidectomy, based upon a preliminary diagnosis of right testicular tumour and the specimen was submitted for histopathology examination. Postoperative pathology examination of the orchidectomy specimen showed that the tumour had cells in nets and trabeculae with chailinized and oedematous stroma, without haemorrhage and necrosis or vascular invasion. The tumour nuclei were noted to be monomorphic, oval-shaped with passing nucleoli, finely dispersed chromatin and no mitoses were found (see figure 5). The spermatic cord, scrotal skin, and surgical margins were free of any tumour. Immunohistochemistry staining studies of the tumour showed that the tumour cells had exhibited positive staining for inhibin and negative staining for pan-cytokeratin, calretinin and synaptophysin (see figure 6). Based upon the pathology and immunohistochemical examination features of the tumour, the testicular tumour mass was diagnosed as a benign Leydig cell tumour of testis

Figure 4: Histology image of Leydig cell tumour. Reproduced from: [59] under Copyright © 2019 The Authors. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)

Figure 4: Immunostaining image of Leydig cell tumour. Reproduced from: [59] under Copyright © 2019 The Authors. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
Six months pursuant to his surgery, the follow-up CT-scan did not identify any local recurrence and distant metastases and his hormonal investigations had remained within the normal ranges.
Zhu et al. [60] stated the following:
Zhu et al. [60] highlighted the radiology-imaging phenotype, as well as the pathological findings of a case of LCT in a 62-year-old man. Zhu et al. [] reported that pre-operative non-contrast CT scan of the patient’s abdomen had revealed a 7.0 cm × 6.4 cm × 5.3 cm oval mass that had heterogeneous density, which was located within his right testis. He also had Pelvic non-contrast MRI scan which showed a heterogeneous mass on T1-weighted and T2-weighted images. The solid part of the tumour exhibited high signal on the diffusion-weighted imaging, and an obvious enhancement on the contrast-enhanced MR imaging. He had ultrasound scan examination which demonstrated a large mixed echogenic space occupying lesion which had involved the whole of his right testis with multiple cystic areas and increased vascularity. The patient underwent radical orchiectomy. The pathologic diagnosis was LCT. The patient underwent operative resection of the tumour. Due to the negative resection margins and absence of distant metastases, the patient did not receive additional radiotherapy or chemotherapy. Four months pursuant to his surgery, he had follow-up assessment CT-scan which did not reveal any local recurrence and distant metastases. Zhu et al. [60] made the ensuing additional iterations:
Justo et al. [61] reported a 91 years old man who had manifested with an increase of the volume of his scrotum for about 1 year, with local pain and hyperaemia over the preceding 7 months. He sought medical attention at the time and was treated with antibiotic therapy for epididymo-orchitis. When it was noted that his symptoms had persisted, he was then referred to the Urology outpatient clinic of the Santa Casa de Misericórdia de Ribeirão Preto. During his clinical examination, he was found to have an enlarged scrotum on the left with transillumination showing fluid, without hyperaemia. During the consultation, a scrotal ultrasound scan was requested. Upon his return, he produced an ultrasound scan report of hydrocele with fine debris within the left side, with a nodular, solid, rounded, partially defined, hypoechoic image with increased flow to the Doppler study that measured 2.0 cm x 1.4 cm x 1.1cm. The patient had complained of dysuria and polyuria, and Justo et al. [61] opted for treatment with antibiotic guided by urine culture and surgical treatment afterwards. He had a frontal chest radiography as a first radiology imaging procedure which demonstrated diffuse osteopenia and ectasia of the aorta. He had Computed tomography (CT) scan which had demonstrated a left renal cyst and infra-centimetric bilateral inguinal lymph nodes. After 3 months, he underwent a trans-inguinal left unilateral orchidectomy, with hydrocele repair. The surgical specimen was sent for histopathology examination. Macroscopic examination of the surgical specimen demonstrated a left testis which measured 5.8 cm x 2.9 cm x 2.7cm, with a smooth outer surface and cut with a yellowish, spongy parenchyma, containing a brown nodule, firm, well delimited and homogeneous, that measured 1.7 cm x 1.5cm, restricted to the parenchyma. Microscopy examination of the surgical specimen demonstrated features of a neoplasm which had consisted of cells with a hypertrophic nucleus, sometimes with evident nucleolus and broad and eosinophilic cytoplasm, all were contained within the testicular parenchyma, with no evidence of infiltration in testicular coating. Absence of invasion of vein and lymphatics. Epididymis and spermatic cord without evidence of neoplastic infiltration. The surgical resection margin of the spermatic cord was free of tumour. The pathology staging of the tumour was: pT1, pNx, pMx. Immunohistochemistry staining studies of the tumour showed that the tumour cells had exhibited positive staining for inhibin, calretinin, melan-A and KI-67. Diagnosis was reported to be consistent with the diagnosis of Leydig cell tumour. The patient returned for follow-up assessment 1 month after his operation, with the presence of hematoma within his scrotum, which was confirmed by ultrasound scan of his scrotum and scrotal contents. sonogram. Just et al. [61] opted for a conservative treatment. Justo et al. [61] made the ensuing educative detailed summating discussions:
Table 1
Scrotal Masses in elderly men.
Testicular
Primary lymphoma
Stromal tumours
Spermatocitic Seminoma
Metastasis
Epidermoid cyst
Leydig Cell Hyperplasia
Fibroma of gonadal origin
Haemangioma
Paratesticular
Lipomas
Adenomatoid Tumours
Leiomyomas
Testicular Appendage with Torsion
Fibrous Pseudo-tumour
Liposarcoma
Reproduced from: [61]
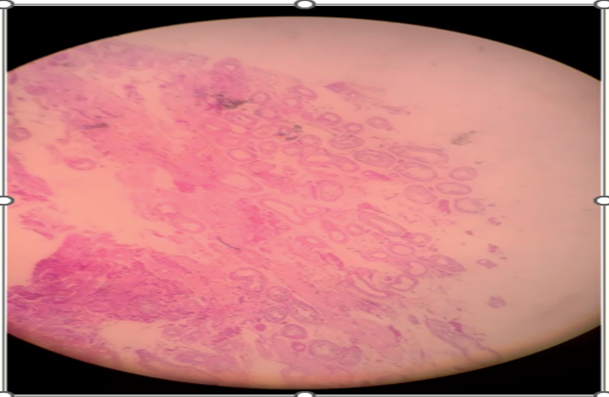
Figure 7: Epididymis (4x). Reproduced from: [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure 8: Seminiferous tubules (4x). Reproduced from [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure 9: Rete testis and seminiferous tubules. (4x). Reproduced from: [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure 10: Inhibin antibody (4x). Reproduced from: [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure 11: Calretinin antibody (4x). Reproduced from: [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure 12: Melan-A antibody (4x). Reproduced from: [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure 13: Ki-67 antibody (4x). Reproduced from: [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure 14: CD 117 antibody (4x), Reproduced from: [61] under Copyright: This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Conflict of interest – none
Acknowledgements –
Acknowledgements to:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
