
Research Article | DOI: https://doi.org/10.31579/2692-9406/098
*Corresponding Author: La Vonne A. Downey, Roosevelt University, 430 Michigan Ave, Chicago.
Citation: © 2022 La Vonne A. Downey, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Copyright: L V A. Downey. (2022). Level of Agitation of Patient in the Emergency Department. Biomedical Research and Clinical Reviews. 6(2); DOI: 10.31579/2692-9406/098
Received: 23 November 2021 | Accepted: 06 January 2022 | Published: 15 January 2022
Keywords: agitation; psychiatric; emergency
His primary purpose of this study was to determine the level of agitation that psychiatric patients exhibit upon arrival at the emergency department. The secondary purpose was to determine whether the level of agitation changed over time depending upon whether the patient was restrained or unrestrained.
Methods: This study was a convenience study of psychiatric patients who presented to a level one trauma center. The patient’s level of agitation upon arrival and for every 30 minutes for 3 hours was assessed using the Sedation Assessment Tool. A comparison was made of SAT scores using SPSS v25 between patients who were and were not restrained.
Results: This study demonstrating that the most agitated patients were the ones who were restrained. However, few psychiatric patients in this study were restrained. Additionally, the level of agitation decreased for most subjects whether restraints were used or not within the 90-minute time frame.
Conclusions: This study found that most psychiatric patients were not agitated upon arrival to the E.D. Those that were the most agitated E.D. patients did calm down even when they were not restrained. These results suggest that we should consider and evaluate the benefits of using alternatives to restraints for psychiatric patients in the E.D.
Psychiatric patients frequently present to emergency departments (E.D.s) across the country [1]. On average, 3.7% of all E.D. patients needed restraint and seclusion, or restraint alone[2-3]. The relationship between the use of restraints and psychiatric patients' agitation in the E.D. is unclear. There are few studies regarding the level of agitation of undifferentiated psychiatric patients presenting to E.Ds. Studies such as Frueh et al. have found that the use of restraints can be traumatic to patients [4]. Others, have cited the need to reduce potential injuries to hospital staff (5-11). It can make it difficult to assess, diagnose, treat and engage with sedated patients. Additionally, sedation medications may interfere with physical illnesses.
The Joint Commission on Accreditation of Healthcare Organizations, Centers for Medicare and Medicaid Services, and many states have regulated the use of restraints and seclusion and pushed for the use of alternatives to restraints [12]. Other organizations such as the Substance Abuse and Mental Health Services Administration have called for a change from seeing restraints as a positive intervention to one that traumatizes patients and healthcare workers [13]. Despite this call for reduction, restraints are still commonly used in Emergency Departments at a range of 25 to 30% [14-18]. Many want to change this practice and reduce restraint usage in the E.D. (19-23). However, the best and most humane methods for modulating agitated patients in the E.D. are not yet determined [20-29].
The purpose of this study was to determine the level of agitation that psychiatric patients exhibit upon arrival to the emergency department. The secondary purpose was to document the change in the level of agitation of psychiatric patients, whether restrained or not, over their time in the E.D.
Location: Inner city, urban level 1 Trauma Center. The location was designated as a police catchment drop-off for psychiatric patients.
Observational Study
This study was a convenience sample of psychiatric patients who entered the emergency department (ED), were enrolled by research fellows from September 2017 through July 2018. Research fellows were in the ED from 6 A.M. to 6 P.M. Monday thru Friday. Only patients who were brought in while a research fellow was present were included in the study as the fellow had to use the assessment tool from the time the patient was brought into the ED. Fellows were trained by the Emergency Department chair on how use and score the Sedation Assessment Tool (SAT). A sample size of 300 or more was needed to achieve 80% power using an alpha of .05 [32]. The level of agitation was assessed using the Sedation Assessment Tool (SAT) every 30 minutes for 3-hour block. A comparison was made of SAT scores using SPSS v25 between patients who were and were not restrained. The study was IRB approved as exempt from consent due to observational nature of study. Additional information, such as the attendings SAT scores, race, gender, and mode of arrival, were collected from the patient’s chart during their stay in the E.D. Once the patient was either admitted, transferred or sent home from the ED the research fellow no longer had access to their information and or chart.
Those included in the study were patients who presented to the Emergency Department with a psychiatric complaint thought to be unrelated to physical illness. Those excluded from the study were patients who were restrained for non-behavior reasons or were medically unstable.
The Sedation Assessment Tool (SAT) is a simple, rapid, and valuable scale used to measure the degree of agitation and response to medication administration and the resultant level of sedation [30-31]. It is easy to administer, with high reliability and no contraindications or complications. See below for table on how score relates to patient responsiveness and speech.
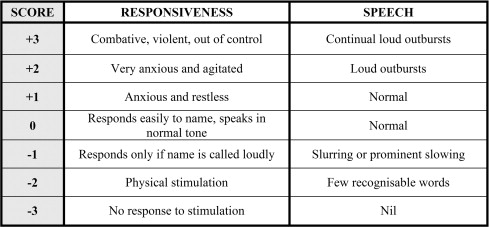
Source: Calver et al.
It was administered by trained research fellows who were responsible for observing subjects in E.D. The SAT was administered upon arrival and every 30 minutes for a 3-hour period.
The chemical restraints used were the following: Ativan/Lorazepam, Haldol/Haloperidol, or Adasuve. The physical restraints used included: Wrist/ Ankle restraints or waist straps.
The study E.D. uses a triage scoring system that is scored 1-5. It is based upon presenting physical parameters such as lab values and vitals (30). The triage scores found in this study were 94% (331) Level 2 or Level 3. Those subjects whom 96% (26) of subjects rated a +3 on the initial SAT score were also given a Triage Score of 2 or 3. This was also seen for 94% (46) of subjects rated a +2 on the initial SAT score were given a Triage score of 2 or 3.
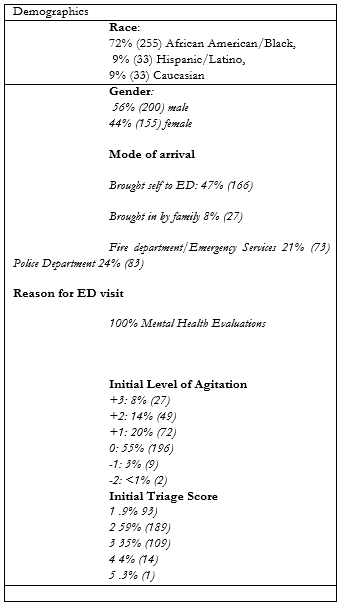
There was a total of 358 patients enrolled in the study. The consisted of 72% (255) African American/Black, 9% (33) Hispanic/Latino, 9% (33) Caucasian. There were more at 56% (200) males than 44% (155) females. The majority were 88% (311) unemployed. The predominate mode of arrival was brought self to ED: 47% (166), brought in by family: 8% (27), CFD/EMS: 21% (73), and CPD: 24% (83). Their initial level of agitation was as follows: +3: 8% (27). +2: 14% (49), +1: 20% (72), 0: 55% (196), -1: 3% (9), and -2: <1 xss=removed xss=removed xss=removed xss=removed>
SAT scores did not necessarily determine which patient was restrained. At 1 hour, 85% (299) of subjects were not restrained whatsoever. However, at 1 hour, 9% [7] of subjects rated an SAT score of +1 were restrained either chemically, physically, or both. These two factors limited the ability to do analysis and comparison of those restrained or not, types of restraints and diagnosis as there was either too low a number or little variance.
There was a significant change in levels of agitation over time. In the study using a paired T-test, there is a statistically significant change (p <0 xss=removed>
There was also a small difference in the SAT scores provider gave compared to the SAT score given by research fellows. A small percent 16% (51) of patients, received conflicting scores on the SAT assessment when conducted by E.D. provider (physician or nurse) vs. when conducted by the research fellow. The score indicates a range of variation in SAT scores. The scores given by the provider were the ones that went into the charts. The difference in shared with the providers.
The results of this study confirm previous research by demonstrating that the most agitated patients were the ones who were restrained [1-9]. That being said, not many psychiatric patients in this study were restrained. Additionally, the level of agitation decreased for most subjects whether restraints were used or not within the 90-minute time frame.
The positive findings in this study results demonstrated that most psychiatric patients are not agitated upon arrival to the E.D. However, the majority of agitated subjects were brought in by Police or Fire Department/Emergency Medical Services. Although, not the focus of this study that finding might indicates that training of first responders in how to reduce and manage aggressive behaviors and de-escalation techniques could impact the level of agitation of patients they bring into the E.D. setting. The training could assist as several studies have shown in the efforts and methods advocated and shown to effectively reduce the use of restraints in the E.D. [20-29].
The level of agitation does not appear to be considered when giving a triage score as there was slight variation within those scores for those who were highly or those who were not agitated. The finding indicates that a triage system based on physical signs and symptoms might not apply when assigning a triage priority to psychiatric patients. Several studies have shown that using a mental health triage system such as the Australian Mental Health triage system does a much better job of determining who needs to be seen than the standard triage system currently used in most U.S. E.D. [30].
The study has several limitations. It had a low percentage of agitated subjects upon arrival. In total only 8% of subjects arrive classified as “combative, violent, out of control” or +3 on SAT scale. These individuals were also not homogenous in terms of diagnoses or indications for restraints.
The study was conducted at a level 1 urban hospital site in the United States. Additionally, this location was a designated site for police to bring psychiatric patients. This may have introduced selection bias. Results might be different in other countries that use other scales, have a more robust psychiatric care system, and use different E.D. triage scoring.
The SAT score tool is observational and based on visual assessment, and therefore subjective. A retrospective chart analysis suggests a difference between SAT score rating given by research fellow vs. SAT score given by E.D. Provider.
This study found that most psychiatric patients are not agitated on arrival in the E.D. Those that were the most agitated E.D. patients did calm down even when they were not restrained. These results suggest that we should consider and evaluate the benefits of using alternatives to restraints for psychiatric patients in the E.D. There needs to be more research done to see t the impact of using alternatives to restraints as to whether or not it will result in better patient care, better outcomes.
More research needs to be done that examines the impact of training police officers to manage psychiatric patients. Would the training decrease the level of agitation for patients brought in by first responders needs to be addressed? Additionally, the impact on the levels of agitations seen within the E.D. and how that relates to the use of restraints could indicate if pre-hospital conditions relate to agitation levels.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
