
Case Report | DOI: https://doi.org/10.31579/2768-0487/132
Eduardo Vazquez N General Hospital, Puebla.
*Corresponding Author: Jonathan De Jesus Ulloa Peregrina, Eduardo Vazquez N General Hospital, Puebla.
Citation: Ulloa Peregrina JDJ, Lien Chang LEJ, (2024), Leukemia Secondary to Lymphoblastic Lymphoma with Development of Aplasia Medullary Post Induction of Hypercvad, Report of Case Clinical and Revision of The Literature, Journal of Clinical and Laboratory Research, 7(4); DOI:10.31579/2768-0487/132
Copyright: © 2024, Jonathan De Jesus Ulloa Peregrina. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 February 2024 | Accepted: 29 February 2024 | Published: 08 March 2024
Keywords: lymphoblastic lymphoma;secondary lymphoblastic leukemia; secondary bones marrow aplasia; hyper-cvad
We describe the case of a patient with lymphoblastic lymphoma who received 8 cycles of chemotherapy with subsequent development of secondary acute lymphoblastic leukemia, requiring initiation of a remission induction chemotherapy scheme based on Hyper-CVAD, developing secondary bone marrow aplasia.
Secondary leukemias are broadly defined as a group of cancers that arise after the existence of a previous malignant neoplasm or patients treated previously with cytotoxic therapy, that is to say chemotherapy or radiotherapy. [1, 2]
The most important group of therapy-related leukemias is that associated with alkylating agents or topoisomerase II inhibitors such as etoposide, doxorubicin and mitoxantrone which have been associated with specific cytogenetic abnormalities in the chromosomes [5 or 7] and in the MLL gene (11q23) [2,3,4]
The course and prognosis depend on the cytogenetic and clinical characteristics. molecular to that presented at the time of diagnosis
Although secondary acute myeloid leukemia (s-AML) has been widely described, it is knows very little about secondary acute lymphoblastic leukemia (s-ALL).
Isolated case series report an s-ALL rate of less than 1perecentage of all acute leukemias 5, its pathogenesis is mainly attributed to the effect of therapies cytotoxic on hematopoietic progenitor cells [2.]
Normally, topoisomerase II plays multiple roles in survival cell phone, so as replication, transcription, condensation and segregation chromosome, allowing a segment of double-stranded DNA to pass through another achieving like this alter its topology.
Toposimorese II inhibitors generate DNA double-strand breaks causing cell death, therefore its side effects generate alterations genetics mainly MLL, PML, RARA and AML1 (RUNX1), and translocations chromosomal as 11q23, being he guy further frequent of translocation in t-AML and acute leukemias [6]
It has been described that the latency from the first diagnosis of malignant neoplasia until the diagnosis of s-ALL is in a range of 60 to 77 months, patients who have a history of hematological malignancies, as well as carriers of the MLL gene rearrangement compared to other cytogenetic subgroups present a shorter latency period [1, 5, 7]
Breast cancer has been the most reported previous diagnosis followed by lymphoproliferative neoplasms (non-Hodgkin lymphoma, chronic lymphocytic leukemia, lymphoma Hodgkin's disease, multiple myeloma) and thyroid, lung, brain, ovary and prostate [2,8,9,10,] likewise family history of lymphomas seems to increase five times the risk of secondary acute leukemia [7]
There is little literature on the treatment of secondary leukemias by absence of prospective studies that directly compare the results, in addition of a worry regard to a elderly morbidity and mortality related with he treatment given previous exposure to cytotoxic therapies.
Patients with secondary leukemia can be expected to have a rate of initial complete response of just over 50perecentage, most of them relapse and Studies suggest that despite continuing with intensive chemotherapy after remission, just around of 10perecentage can be long-term survivors
The Hyper-CVAD chemotherapy (CT) regimen with or without tyrosine inhibitors kinase, has been one of the regimens mostly used to induce remission to these patients even without being able to define it as a first-line regimen, and particularly when a patient with s-ALL is being considered for transplant allogeneic of progenitor cells hematopoietic (TaCPH).
In younger adults, if an HLA-matched sibling donor is available, the TaCPH can be the option preferred and, probably, represent the only possibility of cure, although there are no data from prospective studies that establish this definitively. absolute way.
Older adults who cannot tolerate the side effects of intensive chemotherapy They could be included in clinical trials of targeted therapies. This therapeutic area remains unsatisfactory and further studies are needed to demonstrate effectiveness in treatment schemes [2,3]
Case Clinical
Current condition began in December 2018 with inflammation and growth of the left parotid gland, of rapid evolution, going to a private doctor who decided to treat it as parotitis, with unspecified medications, without improvement of the symptomatology. In March 2019, there was a new increase in the size of the tumor. neck, going to a private hospital, where they requested a tomography in which showed a tumor in the left neck measuring 10 cm in its greatest diameter (not shown). has no study or report), so he was scheduled for a parotid biopsy left and periparotid tissue, which was performed on 06-07-19, reporting lymphoma lymphoblastic with immunohistochemistry positive for Bcl2, CD3 and TdT. (See figures 1.2 and 3) He is evaluated by an external hematologist, who begins first-line CHOP chemotherapy. like (without prednisone or anthracycline due to apparent early cardiotoxicity) for eight cycles, start he 06-15-19 and the ended the 11-29-19, decreasing injury tumor to 18 mm in its largest diameter and isolated nodes of 14 and 15 mm in the neck, with a reduction of 53perecentage compared to baseline, classifying it as a partial response according to to the RECIST 1.1. Was valued by the Service of radiation oncology, who they decide apply radiotherapy 3600 cGy in 18 sessions ending on 07-31-20. It is documented complete remission with new tomographic study. It is valued for the first time in our service on 10-05-2020 with a new simple and contrasted neck tomography, thorax, abdomen and pelvis with late venous phase negative for measurable lesions and no measurable. In November 2020, he attended the Hematology consultation at our unit. presenting evil state general, pallor integumentary and diaphoresis profuse with blood cytometry result leukocytes 3.7/ µ L, neutrophils 0.9/ µ L lymphocytes 2.4/ µ L, hemoglobin 11.9 g/dl, platelets 30,000/ µ L, chemistry blood DHL 884 U/l, bone marrow aspirate was performed with a report of 100perecentage blasts, which They measure 12 to 16 microns in diameter, with scant cytoplasm and vacuoles inside, cores variegated the most cerebriforms, with 0 to 1 nucleolus evident in his inside. Immunophenotype with detection of 74perecentage blasts, CD45+, HLA-DR+, CD34-, TdT+, CD10+, CD19+, CD79+, CD33+, concluding B acute lymphoblastic leukemia common with aberrant CD33 secondary to lymphoma lymphoblastic of cells T, deciding to start remission induction chemotherapy with a Hyper- Reversed CVAD phase B on 11-11-20 applying each phase with 28-day intervals, receiving last phase on 06-23-21, completing the four cycles and documenting no detection of malignant clone by flow cytometry (minimal residual disease of bone marrow negative). On 08-18-21 he entered the Emergency Department with syndrome hemorrhagyparous by gingivorrhagia, documenting cytometry hematic with leukocytes 320/ µ L, neutrophils 144/ µ L, hemoglobin 4.8g/dl, platelets 27000/ L. If suspected of relapse medullary HE makes biopsy of marrow I mean with report of cellularity 30perecentage, (See figure 4) presence of the 3 series cell phones, TdT negative, CD3 negative, discarding infiltration leukemic I lymphomatous. HE concludes aplasia medullary secondary and continues with maintenance chemotherapy adjusted POMP scheme (mercaptopurine fiftyperecentage and methotrexate 44perecentage) without reinductions, for keep figures acceptable cells in peripheral blood. On 06/07/22 he had blood cytometry with leukocytes 2.6/ µ L, neutrophils 0.9/ µ L, hemoglobin 14 g/dl, platelets 58000/ µ L, so bone marrow aspirate was performed with minimal residual disease negative for neoplastic phenotype, maintenance chemotherapy dose is again adjusted POMP (methotrexate twentyperecentage and Mertaptopurine(50perecentage) Follow-up he day 08-18-22 continuing with POMP chemotherapy regimen adjusted to said doses, cytometry hematic of control leukocytes 2.8/ µ L, neutrophils 1.6/ µ L, platelets 113,000/ µ L, hemoglobin 13.6g/dl.
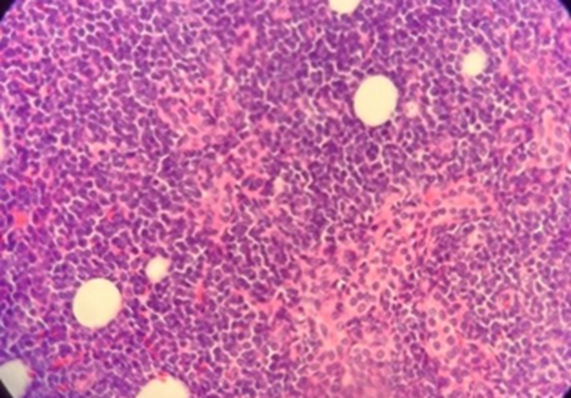
Figure 1: Hematoxylin and Eosin (lymph node).
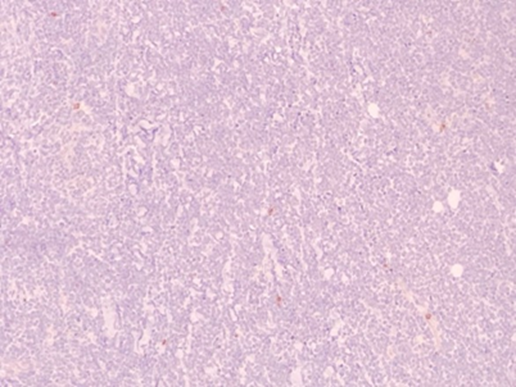
Figure 2: Myeloperoxidase (lymph node).
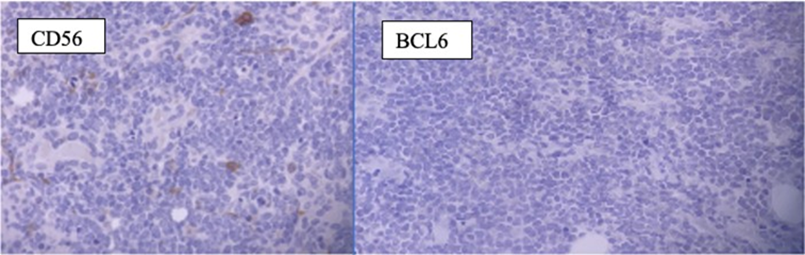
Figure 3: CD56, BCL 6 (lymph node).
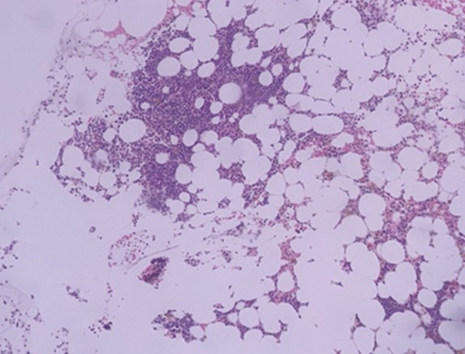
Figure 4: Bone marrow 10 Discussion.
The leukemias lymphoblastic high schools are an entity bit characterized due to the limited literature and absence of protocols therapeutic, No being possible estimate the survival neither choose between a scheme chemotherapy or other, probably be an entity underdiagnosed due to the high mortality to short and medium term, masking symptomatology with the neoplasia malignant of base. This associated mostly to agents’ chemotherapy as the inhibitors of the topoisomerase II and the agents’ alkylating agents, the which are used frequently in the most of regime’s chemotherapy for different guys of cancer mostly of mother and lymphomas. Our patient account with antecedent of to have received cyclophosphamide unknown dose, which could have been the trigger for developing leukemia. HE decides Start Q.T. with scheme Hyper-CVAD, he which has been he mainly used, presenting multiple paintings of neutropenia febrile with resolution of the same to the introduce recovery of the series granulocytic, with suitable answer in each cycle, presenting minimal residual disease negative for neoplastic cells at complete the first and fourth QT cycles documenting negative cerebrospinal fluid leukemic infiltration, which improves the prognosis. When spinal aplasia is evident secondary, which could be associated with high doses of chemotherapy drugs, He decided adjust dose of Q.T. of POMP for keep figures acceptable in lines peripheral cell phones. At the moment, he patient HE finds completing oral maintenance and has fully returned to oral activities daily.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
