
Case Report | DOI: https://doi.org/10.31579/2578-8949/008
*Corresponding Author: Benjamin Dylan, Department of Dermatology, Southern California, USA.
Citation: Benjamin Dylan, Hayden Wyatt, Cesar Ricardo,and Mitchell Troy, Lesions of Cutaneous Leishmaniasis Elicited after Local Trauma: A Case Report. J .Dermatology and Dermatitis. Doi: 10.31579/2578-8949/008
Copyright: © 2017 Benjamin Dylan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 May 2017 | Accepted: 30 May 2017 | Published: 04 June 2017
Keywords: public health; dermatology; cutaneous leishmaniasis; leishmania; local trauma; lesion; skin
In Brazil there is an average of 30,000 cases of Cutaneous Leishmaniasis reported annually, and around the world it happens for about each 20 seconds. Although there are still opportunities to contribute with studies about this disease; supporting the medical community, especially dermatologists, mainly because of the necessity of knowing that a relatively simple procedure can result such a relevant trauma. Female patients presented erythematous plaque in the limb. Lesion appeared days after laser sessions for hair removal. Biopsy showed amastigotes forms and positive culture. After unsuccessful treatment it was managed with N-methyl glucamine 20 mgSbV/kg/day, during 20 days, there was significant improvement of the clinical picture. This study aims to present a case report of Cutaneous Leishmaniasis initiated after local trauma. Literature reports describe primary or secondary lesions of Cutaneous Leishmaniasis elicited after a local trauma. The mechanism used in order to explain these events was the migration of infected macrophages induced by cytokines. Similar events have also been reported as part of the locus minoris resistentiae concept that comprises situations in which microorganisms have a tendency to settle at places of weakened resistance. Considering that Leishmaniasis lesions are usually developed in promastigote forms are inoculated by the Phlebotominae, in this case it was noted that the infection has been favored by the local trauma.
Considered to be an emergent disease, Cutaneous Leishmaniasis (CL) happens every 20 seconds in the world. In Brazil an average of 30,000 cases are notified annually [1]. Even though, the certain about its pathogenesis is not enough yet [2]. Gender, skin temperature [3], polymorphisms of the species [2,4], host's immune response [4], site of inoculation [5] have already being implicated, but poorly understood [5]. Thus, this study aims to report a case of Cutaneous Leishmaniasis triggered after local trauma.
A Thirty year-old information analyst, female patient, from Brasilia, Brazil, presented at our centre in November 7th, 2012, with an erythematous ulcerated plaque with crusts in the lower third of her right limb (Figure 1). The lesion started as a necrotic patch a day after a Glass laser® session for hair removal in July 7th, 2012. She denied any recent trips before the event, but informed that she usually visits the local botanic park. She was treated with cephalexin and bacitracin ointment without improvement.
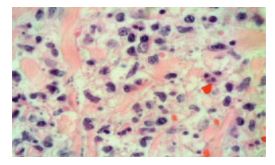
During the investigation, she was submitted to a skin biopsy that showed amastigotes inside histiocytes and inflammatory process (Figure 2). Smear and culture were positive. The Leishmania identified as Leishmania (Viannia) braziliensis was performed by Polymerase Chain Reaction (PCR), RFLP and sequencing of ribosomal DNA from region ITS1 [6]. The HIV serology was negative and the patient was not taking any immunosuppressant drugs. The investigation for fungi, mycobacteria and cutaneous tuberculosis was negative.
She was treated with 3 (three) doses of intramuscular pentamidine injections, 4 mg/kg/day. This treatment's choice was based on a clinical trial in course at our centre, after the patient's informed consent. As no improvement was obtained after three months of follow up, the patient was retreated with N-methyl glucamine 20 mgSbV/kg/day - 20 days, with complete healing of the ulcer (Figure 3).


lesions of CL elicited after local trauma [7-10]. In two experimental models described, involving hamsters [3] and BALB/c mice [11], it was observed an earlier and more frequent onset of Leishmaniasis lesions where trauma was previously induced. The mechanism used to explain these events would be the migration of infected macrophages induced by inflammatory cytokines [3,8,11]. The profile of these cytokines is also important, since the tissue growth factor beta (TGFβ) is increased during tissue repair. TGFβ is also implicated in macrophage inactivation, which could favor the progression and recurrence of the disease [3,5].
Similar events have also been reported as part of the locus minoris resistentiae concept that comprises situations in which microorganisms have a tendency to settle at places of weakened resistance, such as sites of trauma [12]. In other words, trauma does not inoculate the parasite, but favors its fixation at that site [13]. These reports identified this mechanism during paracoccidioidomycosis [13], Pott's disease [14], parvovirus B19 [12], atypical mycobacteria [15] and Tricophyton mentagrophytes infections [16].
On the reported case, an immunocompetent patient, that resides in an endemical area for CL (Distrito Federal, Brazil), and who did not have any clinical signs of the disease, is described. The patient developed CL lesion at the same site of the induced trauma, with short incubation period, as stated in literature [3,11]. The Leishmania species responsible for such lesions is already expected to be Leishmania (Viannia) braziliensis, since it is the most prevalent species in Brazil and in Distrito Federal [4,17].
Leishmaniasis is dynamic disease, as its transmission is continually changed in relation to environmental, demographic and human behavioural factors [18]. Considering that Leishmaniasis lesions are usually developed where promastigote forms are inoculated by the Phlebotominae [4]. The finding of Leishmaniasis lesions following trauma may contribute to a greater comprehension of the metastasis-like formation process during Leishmania infection. It may also alert dermatologists to the possibility of this event on such a frequent practice.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
