
Case Report | DOI: https://doi.org/10.31579/2692-9562/124
1A.T. Still University, Mesa, School of Osteopathic Medicine.
2 Scripps Memorial Hospital, La Jolla, Department of Electrophysiology.
3 University of California, San Francisco, Department of Radiology & Biomedical Imaging.
*Corresponding Author: Joshua Elmore, A.T. Still University, Mesa, School of Osteopathic Medicine.
Citation: Joshua Elmore, Henry Chen, Gwen Janczyk, Leonard Goldstein, Douglas Gibson, (2024), Left Ventricular Pseudoneurysm Post-Radiofrequency Ablation: A Case Report, Journal of Clinical Otorhinolaryngology, 6(4); DOI:10.31579/2692-9562/124
Copyright: © 2024, Joshua Elmore. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 05 May 2024 | Accepted: 31 May 2024 | Published: 14 June 2024
Keywords: pulsed field ablation system; radiofrequency ablation; steam pop; left bundle branch block; left ventricular aneurysm
Myocardial infarction (MI) is a recognized cause of left ventricular (LV) aneurysms, however, on rare occasions, they may be produced by radiofrequency ablation (RFA) therapy [1]. Cardiac arrhythmias, such as premature ventricular contractions (PVCs), are commonly treated with RFA. Generally, RFA is considered a safe and effective intervention, but complications can occur, including myocardial damage leading to the development of aneurysms
Myocardial infarction (MI) is a recognized cause of left ventricular (LV) aneurysms, however, on rare occasions, they may be produced by radiofrequency ablation (RFA) therapy [1]. Cardiac arrhythmias, such as premature ventricular contractions (PVCs), are commonly treated with RFA. Generally, RFA is considered a safe and effective intervention, but complications can occur, including myocardial damage leading to the development of aneurysms [1]. To our knowledge, this phenomenon is underreported, necessitating more literature to support the development of proper protocol surrounding this complication. Due to the above complications, pulse field ablation (PFA) is a promising alternative approach to RFA, and to our knowledge, is underreported.
We present a 60-year-old female patient with a chronic history of hypertension and frequent premature ventricular contractions (PVCs) at rest alongside an 18% PVC burden, and isolated PVCs confirmed by echocardiogram (see Figure 1). The patient was referred to electrophysiology for consultation regarding PVC ablation. During the procedure, a PVC originating from the lateral aspect of the lateral papillary muscle was identified.
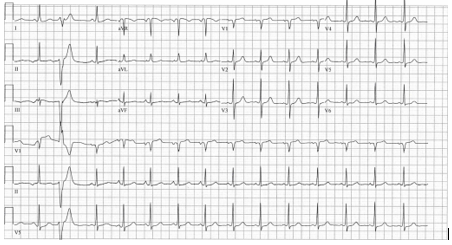
Figure 1. Initial electrocardiogram (ECG) Pre-Ablation Procedure - Reading: sinus rhythm with occasional premature ventricular complexes with new PVC
A transseptal catheterization was performed to approach the lateral papillary muscle from the lateral side due to PVC origination. 3D mapping was done using the Abbott system. An 8 French sheath was placed in the right common femoral artery and 7, 8, and 10 French sheaths were placed in the right common femoral vein. A deflectable decapolar catheter was positioned in the coronary sinus and a bidirectional tactic cath was utilized for catheter ablation. The patient had frequent PVCs in the laboratory on the date of her ablation which presented as dominant R waves in lead V1. They were negative in leads II, III, and aVF. Lead I was isoelectric to slightly negative. Catheter ablation was performed using the bidirectional TacticCath ablation
catheter with power settings set at 40 to 42 W and contact force was targeted at 10 to 20 g. Total ablation time was 8 minutes and we originally attempted ablation from the medial side using retrograde aortic approach, however, even though the PVCs were suppressed, they came back during the waiting period. We then performed transseptal catheterization and approached the papillary muscle from the lateral aspect which was successful. During follow-up, the patient presented with bilateral ocular migraines and vision issues not previously reported. Investigation revealed the presence of a left bundle branch block (LBBB), which was not observed before the ablation (see Figure 2 in comparison to Figure 1).

Figure 2. Follow-up ECG Reading: sinus rhythm with short PR, Left bundle branch block, abnormal ECG when compared with ECG #2
A post-event monitor confirmed the bundle branch block. Subsequent post-ablation echocardiography revealed the presence of an acquired posterolateral left ventricular aneurysm in the inferior wall, measuring 2.9 x 2.1 cm with a narrow neck diameter of 5.2 mm.
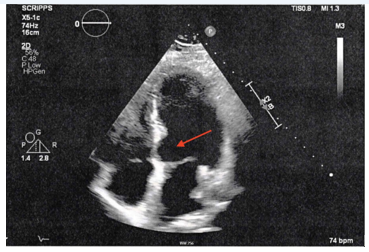
Echocardiogram: Post-Ablation Procedure - Impression: Aneurysm present in the inferior wall.
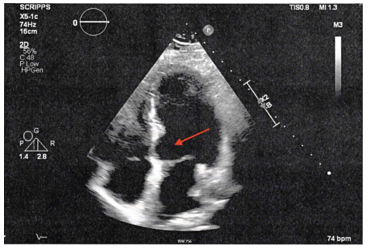
CT Cardiac: Post-Ablation Procedure - large inferior ventricular wall pseudoanauerysm measuring
2.9 x 2.1 cm, with a narrow neck diameter of 5.2 mm.
However, the echocardiogram conducted before the ablation showed no evidence of an aneurysm. The patient underwent cardiothoracic surgery for resection of the inferior wall left ventricular aneurysm, hematoma evacuation, and patch repair using a two-layer patch of bovine pericardium and Gelweave graft.
The patient was selected based on the uniqueness of the clinical presentation, rarity of the condition, and educational value. This case report was conducted in compliance with the ethical principles outlined in the Scripps Memorial Hospital guidelines and the patient's informed consent was obtained prior to the publication of this case report. Patient identifying information has been de-identified to ensure confidentiality. As this case report does not involve a human clinical trial, we did not seek consultation from an IRB affiliate. Nonetheless, we adhered closely to the guidelines set forth by HIPAA, ensuring strict compliance and patient confidentiality. Relevant articles were identified through searches of electronic databases (e.g., PubMed, Embase) using keywords such as pulsed field ablation (PFA) system, hypertension, premature ventricular contractions, PVC ablation, left bundle branch block (LBBB), acquired left ventricular aneurysm, and cardiothoracic surgery. The literature review was used to provide context, compare our findings with previous reports, and support our discussion and conclusions. The case report aims to contribute to the medical literature by documenting a rare or unusual presentation, treatment modality, or outcome.
Premature ventricular complexes (PVCs) are common with the incidence of PVCs possibly increasing the risk of heart failure and mortality [1]. Markedly, successful catheter ablation of PVCs has been shown to restore some systolic dysfunction, signifying a fundamental relationship [2]. Medical treatment and catheter ablation are considered primary therapeutic options in patients with symptomatic PVCs or a reduced left ventricular ejection fraction [1,2].
Radiofrequency (RF) catheter ablation brings primary risks and may not be necessary unless the patient presents with symptoms, nonetheless, when employed, it is highly effective at eliminating PVCs. Although rare, one of these risks is the possibility of left ventricular aneurysm development which most likely occurred during our patient’s ablation procedure as depicted by given imaging modalities. While myocardial infarction is the most traditional cause of left ventricular (LV) aneurysm development, it is imperative to consider other common etiologies, which is demonstrated by our case. The term "aneurysm" describes the bulging or outpouching of a weakened muscle wall, and in the case of ventricular aneurysm, it occurs due to the natural course of a full-thickness infarct being replaced by fibrous tissue [3]. Fibrous tissue is noncontractile creating an outpouching that externally herniates during systole, resulting in the enlargement of an area of dyskinesia [3]. Left ventricular pseudoaneurysms have a propensity to rupture and for that reason, regardless of symptomatology, excision is necessary [3]. Given that our patient's aneurysm was detected early following her ablation procedure, it is reasonable to conclude that this was an acquired aneurysm resulting from a "steam pop" complication that occurred during the procedure. During radiofrequency (RF) ablation, a steam pop can occur as a potentially severe complication which although rare, led to the development of a LV aneurysm in our patient. The described complication results in localized tissue damage due to the unwarranted heating of tissues which causes the tissues fluids to boil and the vaporization of gases [4,5]. Nonetheless, a recently developed pulsed field ablation (PFA) system shows promise as a potentially more efficient and safer alternative. PFA utilizes a unique nonthermal ablation technique capable of selectively targeting myocardial tissue which is unlike alternative types of ablation energy sources and a novel therapy [6]. The PFA method causes a disrupting in cell membranes, creating permanent nanoscale pores using extremely rapid electrical pulses ranging from micro- to nanoseconds [7,8,9,10]. Electroporation is the result which ultimately leads to cell death [6]. Nevertheless, the maximum field strength for tissue necrosis varies amongst different tissue types, with tissues such as the myocardium having a lower propensity for dielectric cell membrane collapse when paralleled to blood vessels and nerves [11,12,13]. With the intention of minimizing the risk of harmful outcomes, the PFA method can be employed to ablate myocardial tissue effectively and exclusively. The pulsed ablation system is groundbreaking because it represents a new and innovative approach to tissue ablation and the comparison between RF and PFA is underreported. Ultimately, the goal is the potential utilization of pulsed electrical fields in catheter ablation for ventricular arrhythmias to improve safety and minimize collateral damage by exploring its application during these types of procedures and similar ones. PFA therapy aims to target and isolate specific characteristics of cardiac tissue for irreversible electroporation, inducing cell death and durable lesions [3]. Lower damage thresholds and selectively of PFA minimizes collateral injury to surrounding tissues by affecting cardiac tissue only. System polarity, waveform shape, and catheter design are all PFA parameters that can be customized for treatment safety and efficacy optimization [3]. A recent study researching single-shot pulmonary vein isolation (PVI) with the PFA system found that the PFA PVI was achieved in 100% of cases, with a single-shot isolation rate of 99.5% [14]. Another paper comparing the IMPULSE (NCT03700385), PEFCAT (NCT03714178), and PEFCAT II (NCT04170621) observed out of 121 patients, 100% of pulmonary veins (PVs) achieved acute PVI using PFA alone [6]. Both of the articles outlined above explain how employing a "single-shot" PFA catheter for PVI established meritorious durability and satisfactory safety, complemented by a low rate of atrial arrhythmia reappearance within one year. Subjects contributing to these studies underwent follow-up evaluations at specific time points, including 30 days, 75 days (PEFCAT and PEFCAT II studies), or 90 days (IMPULSE study), as well as at 6 months and 12 months [6]. During these evaluations, it was determined that in intermittent AF patients, PVI using either the flower or basket PFA catheter was found to be a safe, effective, and durable treatment option for patients with paroxysmal Atrial Fibrillation (AF) [6].
This case highlights the rare occurrence of an acquired postolateral LV aneurysm following RFA for PVCs. The patient’s development of a LBBB and subsequent ocular migraines following the ablation procedure raised concerns, leading to the discovery of the aneurysm. The prompt intervention with cardiothoracic surgery for resection of the aneurysm and patch repair demonstrates the importance of a timely diagnosis and management in such cases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
