
Case Report | DOI: https://doi.org/10.31579/2693-2156/020
* Critical Care Unit, Al-Rodah Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
*Corresponding Author: Yasser Mohammed Hassanain Elsayed, Critical Care Unit, Al-Rodah Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
Citation: Elsayed Y M H, (2021). Left bundle branch block and Wavy triple sign (Yasser’s sign) intertwining COVID-19 Pneumonia with Renal Impairment; defective Sgarbosa criteria for Thrombolytic: A Case Report in Cardiology, Infectious Diseases, Nephrology, and Critical Care Medicine. J Thoracic Disease and Cardiothoracic Surgery, 2(1); DOI:10.31579/2693-2156/020
Copyright: © 2021, Elsayed Y M H. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2021 | Accepted: 18 April 2021 | Published: 10 May 2021
Keywords: COVID-19; pneumonia; left bundle branch block; Wavy triple sign; Yasser’s sign; Sgarbosa criteria; renal impairment; tachypneic; cefotaxime; azithromycin; oseltamivir; paracetamol
Rationale: Left bundle branch block is a diagnostic utility for ST-segment elevation myocardial infarction equivalent. Consequently, administration of thrombolytic is a pivotal step. Emergent Sgarbosa criteria and their modification are considered helpful guide keys. Wavy triple an electrocardiographic sign (Yasser Sign) is a novel diagnostic sign in hypocalcemia. Interestingly, the presentation of COVID-19 pneumonia with an intertwining left bundle branch block, renal impairment, and hypocalcemia has a risk impact on both morbidity and mortality of COVID-19 patients. Patient concerns: An elderly carpenter male COVID-19 patient was admitted to intensive care unit with COVID-19 pneumonia with interlacing left bundle branch block, renal impairment, and Wavy triple sign (Yasser’s sign). Diagnosis: Left bundle branch block and Wavy triple sign (Yasser’s sign) intertwining COVID-19 pneumonia with renal impairment. Interventions: Arterial blood gases, chest CT scan, electrocardiography, oxygenation, and echocardiography. Outcomes: Gradual dramatic clinical, electrocardiographic, and radiological improvement had happened. Lessons: The triage of the left bundle branch block with the COVID-19 patient is highly significant for both diagnosis of acute myocardial infarction and giving thrombolytic. The combination of left bundle branch block, renal impairment, and hypocalcemia COVID-19 pneumonia signifies the risk in the current case study.
Left bundle branch block (LBBB) is a common condition in clinical cardiovascular. Suspected acute myocardial infarction (AMI) in the setting of LBBB presents a unique diagnostic and therapeutic challenge to the clinician. The diagnosis is especially difficult due to electrocardiographic changes caused by altered ventricular depolarization. Sgarbossa’s criteria were initially very weak and, over time, became highly suggestive of acute ST-segment elevation myocardial infarction (STEMI)[1]. Sgarbossa et al. suggested a score of > 3 points in the next criteria for the diagnosis of AMI in the existence of LBBB: (1) concordant ST-segment elevation of 1 mm (0.1 mV) in at least 1 lead (5 points), (2) concordant ST-segment depression of at least 1 mm in leads V1 to V3 (3 points), or (3) excessively discordant ST-segment elevation, defined as greater than or equal to 5 mm of ST-segment elevation when the QRS result is negative (2 points) [2]. A modified Sgarbossa rule has been proposed for the diagnosis of AMI in the existence of LBBB [3]. An interesting point regarding this rule, the substitution of the third Sgarbossa element (excessively discordant ST-segment elevation as defined by 5 mm of ST-segment elevation in the setting of a negative QRS) with one defined proportionally by ST-segment elevation to S-wave depth (ST/S ratio) was proposed to have better diagnostic utility for STEMI equivalent[4]. LBBB concerning acute STEMI is very important. Yasser et al. (2019) reported a case of LBBB with thereafter developed acute STEMI that was indicating for thrombolytic therapy [1]. Wavy triple an electrocardiographic sign (Yasser Sign)is a new innovated diagnostic sign in hypocalcemia [5]. The analysis for this sign in the author interpretations are based on the following;
1. Different successive three beats in the same lead are affected.
2. All ECG leads can be implicated.
3. An associated elevated beat is seen with the first of the successive three beats, a depressing beat with the second beat, and an isoelectric ST-segment in the third one.
4. The elevated beat is either accompanied by ST-segment elevation or just an elevated beat above the isoelectric line.
5. Also, the depressed beat is either associated with ST-segment depression or just a depressing beat below the isoelectric line.
6. The configuration for depressions, elevations, and isoelectricities of ST-segment for the subsequent three beats are variable from case to case. So, this arrangement non-conditional.
7. Mostly, there is no participation among the involved leads. The author intended that is not conditionally included in an especial coronary artery for the affected leads[5].
The initial presentation of a novel Coronavirus-2 (COVID-19) that is resulting in severe acute respiratory syndrome (SARS) had appeared in Wuhan, China in December 2019[6]. COVID-19 Disease is a highly communicable, rapidly spread, lethal worldwide disease[7]. Despite COVID-19 disease was primarily presented with respiratory symptoms, but cardiovascular involvements were common and accompanied by higher mortality among these patients [8].
Case presentation
A 57-year-old married carpenter Egyptian male patient presented in the emergency department with acute tachypnea and fever. Fatigue, loss of appetite, and generalized body aches were associated symptoms. Currently, he had a history of contact with a neighbor who confirmed a COVID-19 patient in the past 10 days. The patient was admitted to the intensive care unit (ICU) with acute pneumonia. Upon general physical examination; generally, the patient was tachypneic, distressed, with a regular pulse rate of 70 bpm, blood pressure (BP) of 100/70 mmHg, respiratory rate of 36 bpm, the temperature of 39.3 °C, and pulse oximeter of oxygen (O2) saturation of 91%. He seemed obese. No more relevant clinical data were noted during the clinical examination. The patient was treated in ICU with COVID-19 pneumonia (Figure 1A).

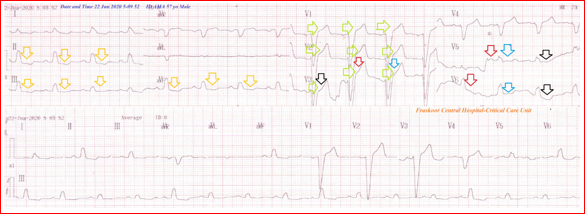
LBBB and Wavy triple sign (Yasser’s sign) of hypocalcemia in consequent ECG (Figure 2).
Initially, the patient was treated with O2 inhalation by O2 cylinder (100%, by nasal cannula, 5L/min). The patient was maintain treated with cefotaxime; (1000 mg IV every 8 hours), azithromycin (500 mg PO single daily dose), oseltamivir (75 mg PO twice daily only for 5 days), and paracetamol (500 mg IV every 8 hours as needed). SC (enoxaparin 80 mg twice daily), aspirin tablet (75 mg, once daily), clopidogrel tablet (75 mg, once daily), and hydrocortisone sodium succinate (100 mg IV every 12 hours) were added. The patient was hourly monitored for temperature, pulse, blood pressure, and O2 saturation. The initial complete blood count (CBC); Hb was 10.4 g/dl, RBCs; 3.89*103/mm3, WBCs; 8.6*103/mm3 (Neutrophils; 86.9 %, Lymphocytes: 9.4%, Monocytes; 2.7%, Eosinophils; 1% and Basophils 0%), Platelets; 148*103/mm3. S. Ferritin was high; 569 ng/ml. D-dimer was high (644 ng/ml). CRP was high; 17.1 g/dl. LDH was high; 611 U/L. SGPT was normal; 17 U/L, SGOT was normal; 13 U/L. Serum creatinine showed moderate elevation; 4 mg/dl and blood urea; showed mild elevation; 124 mg/dl was high. RBS was; 113 mg/dl. Ionized calcium was mildly low; 0.69 mmol/L. The troponin test was negative. Initial ABG showed acute metabolic acidosis. After 8 days of management; CBC; Hb was 12.7 g/dl, RBCs; 3.94*103/mm3, WBCs; 7.15*103/mm3 (Neutrophils; 66.4 %, Lymphocytes: 24.2%, Monocytes; 9.4%, Eosinophils; 0% and Basophils 0%), Platelets; 208*103/mm3. Serum ferritin was normal; 266 ng/ml. D-dimer was normal (142 ng/ml). CRP was negative (0.1 g/dl). LDH was still high; 552U/L. SGPT was normal; 25 U/L, SGOT was normal; 19 U/L. Serum creatinine showed mild elevation; 3.3 mg/dl and blood urea showed mild elevation; 125 mg/dl were normal. Ionized calcium was normal; 1.10 mmol/L. The troponin test had still negative. RBS was normal; 93 mg/dl. Last ABG showed partly compensated metabolic alkalosis. The last chest CT scan was done within 8 days of the presentation showing nearly dramatic improvement of the above ground-glass consolidations. (Figure 1B).

Echocardiography showed mild hypokinesia in the anterior segment with an EF of 55%. Left bundle branch block and Wavy triple sign (Yasser’s sign) intertwining COVID-19 pneumonia with renal impairment was the most probable diagnosis. Within 24 days of the above management, the patient finally showed nearly complete clinical, radiological, and laboratory improvement. The patient was continued on aspirin tablet (75 mg, once daily), oral nitroglycerine capsule (2.5 mg, twice daily), oral calcium, and vitamin-D preparation for 30 days with further recommended cardiac and renal follow-up.
Overview:
• An elderly carpenter male COVID-19 patient was admitted to the intensive care unit with COVID-19 pneumonia with interlacing LBBB, renal impairment, and Wavy triple sign (Yasser’s sign).
• The objective primary for my case study was the presence of LBBB in the presence of COVID-19 pneumonia, renal impairment, and Wavy triple an ECG sign (Yasser Sign) of hypocalcemia in ICU.
• The secondary objective for my case study was the question of; How did you manage the case?
• The triage of the left bundle branch block with the COVID-19 patient is highly significant for both diagnosis of acute myocardial infarction and giving thrombolytic.
• The combination of left bundle branch block, renal impairment, and hypocalcemia COVID-19 pneumonia signify the risk in the current case study.
ABG: Arterial blood gases
AMI: Acute myocardial infarction
CBC: Complete blood count
COVID-19: Coronavirus disease 2019
ECG: Electrocardiography
IV: Intravenous
LBBB: Left bundle branch block
O2: Oxygen
SGOT: Serum glutamic-oxaloacetic transaminase
SGPT: Serum glutamic-pyruvic transaminase
STEMI: ST segment elevation myocardial infarction
VR: Ventricular rate
• There are no conflicts of interest.
• I wish to thanks the nurse team of the intensive care unit to give me extra copies of the ECG to help me.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
