
Research Article | DOI: https://doi.org/10.31579/2692-9759/037
1 Bachelor of Medicine and Surgery.
2 Santa Ana Hospital Motril: Hospital Santa Ana.
*Corresponding Author: Antonio Carranza Pinel, Unidad de Cuidados Intensivos Cardiológicos, Hospital Universitario Clínico San Cecilio, Avda. del Conocimiento s/n, 18016 Granada, Spain.
Citation: I Baig, A Eslami, A Berger, C Nordberg, J Blankenship (2022) Left Branch Cardiac Stimulation. Beginning of a Program in Icu. Cardiology Research and Reports. 4(4); DOI: 10.31579/2692-9759/037
Copyright: © 2022 Antonio Carranza Pinel, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 March 2022 | Accepted: 28 March 2022 | Published: 20 April 2022
Keywords: cardiac stimulation; symptomatic bradyarrhythmias; hispanic stimulation
Cardiac pacing is the only treatment available for patients with Symptomatic bradyarrhythmias in the absence of reversible causes. For about 50 Apical right ventricular pacing has been used for years.
Cardiac pacing is the only treatment available for patients with Symptomatic bradyarrhythmias in the absence of reversible causes. For about 50 Apical right ventricular pacing has been used for years. However, this technique can produce asynchrony in patients who require frequent stimulation, being associated with an increased risk of heart failure, mitral dysfunction and fibrillation handset. Pacing at alternative sites in the right ventricle, such as the septum or outflow tract, has not been shown to be superior to apical stimulation.
For this reason, interest in techniques that simulate physiological stimulation has gone growing in recent years. Within this type of technique, the most physiological and up-to- date Today the most used is Hispanic stimulation (HE), with multiple studies that support its feasibility and clinical benefits. HD has been associated with a lower risk of pacing cardiomyopathy, heart failure, and mortality compared with apical right ventricular pacing.
However, there are factors that limit the use of HE routinely: the success of a HD implantation requires a long learning curve even for implanters considered experts, high capture thresholds must be assumed during implantation and there is even the risk of maintaining high thresholds in subsequent reviews. Besides, the HE may not be successful in patients with distal Hisian blocks, or may require Unacceptably high thresholds to correct bundle branch blocks.
Huang et al. demonstrated in 2017 the feasibility of stimulation below the area Left bundle branch block (LBB) in a patient with complete bundle branch block left and heart failure, achieving cardiac resynchronization. Others have been capable of reproducing the feasibility of ERI in small series of cases.
Today ERI is a growing cardiac pacing technique, more reproducible than HD and with promising results. The objective of our study is to corroborate the feasibility and reproducibility of this technique, as well as showing the results of the follow-up during the first three months after implantation.
Prospective descriptive study of 20 patients and their follow-up in consult during the first three months. During the intervention, ultrasound-guided puncture of the left axillary vein was performed. Medtronic Select Secure 3830-69 Electrode Implantation, Advanced Over Sheath fixed curve C315 for His, from Medtronic. The objective was to position the cable in the interventricular muscle septum until a right bundle branch block pattern is achieved (qR or qRS in V1) with the stimulation performing the monitoring of the technique in portable electrophysiological measurement system with fully integrated stimulator EP- TRACER 2 Portable.
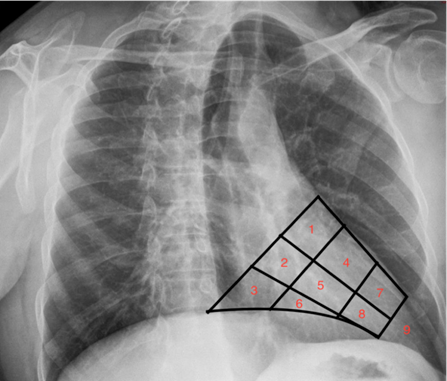
The radiological image is used as a reference for the correct position of the electrode. In right anterior oblique at 30o dividing the cardiac silhouette into nine segments starting the division at the level of the tricuspid valve and segment nine being the apex. (Image 1). We carry out a 1.5 cm sampling on said segment towards the septum baseline and / middle septum until the required electrocardiographic pattern is obtained at the beginning of the stimulation in 5 V at 0.4 ms.
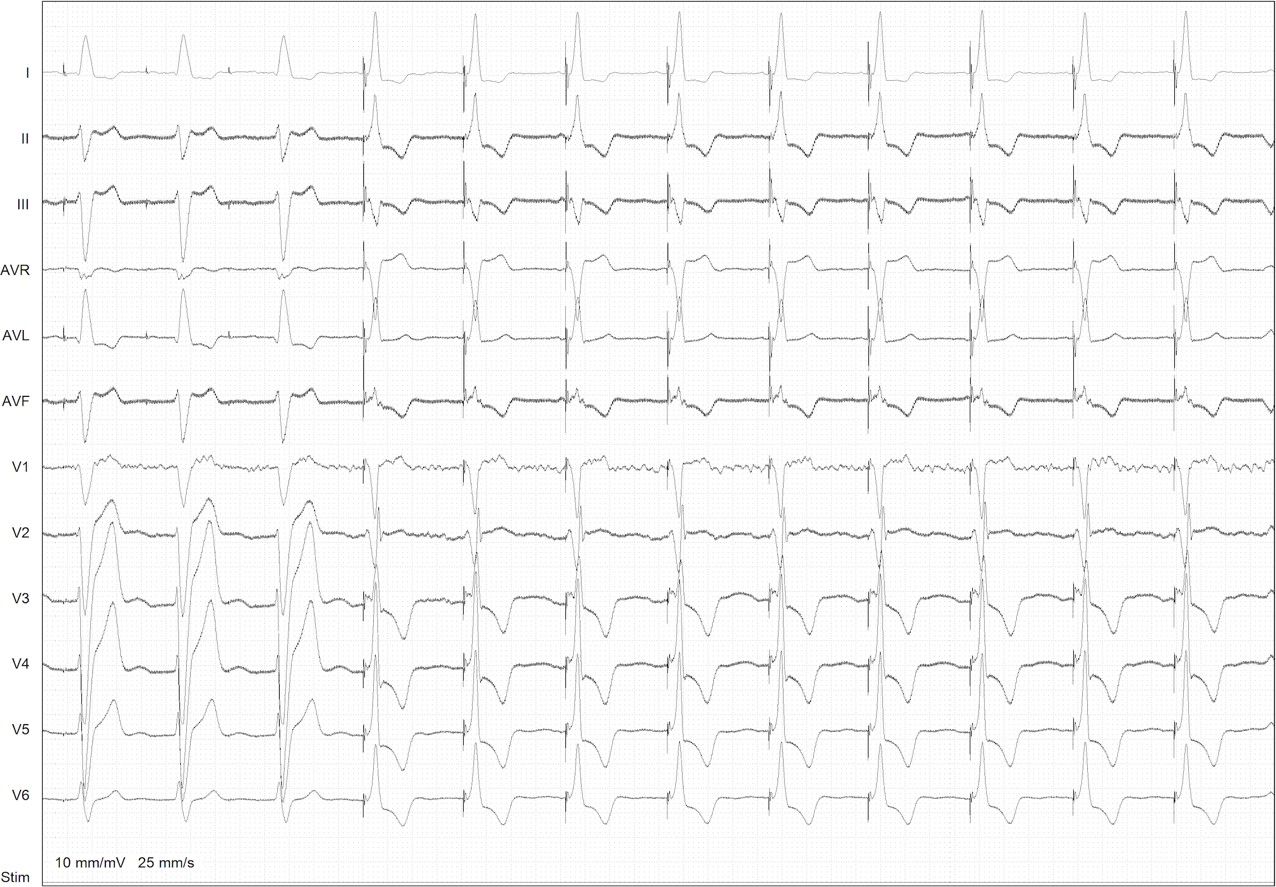

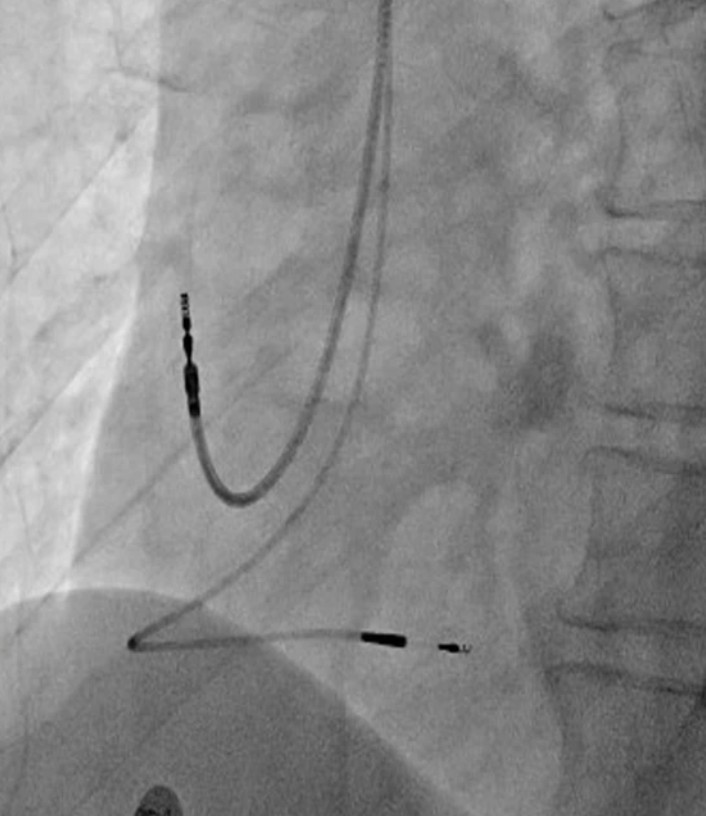
If we maintain this pattern (qR or qRS in LV) by lowering the stimulation threshold between 3 V and 5 V and after making a first measurement of the impedance, we begin to penetrate the electrode into the intraventricular septum in an oblique X-ray view left at about 30o. (Picture 4).
After verifying that the electrode penetrates the septum satisfactorily, we perform new measurements until the narrowest possible paced QRS is obtained with a stimulation threshold always <2>
A total of 12 dual-chamber and 8 single-chamber pacemakers were
Left bundle branch pacing in patients with an indication for Cardiac resynchronization is a novel technique, arising from the greater evidence of the deleterious effects on the heart caused by sustained apical stimulation of the Right ventricle. Despite the lack of studies that corroborate the safety and The long-term efficacy of this technique, in our unit, has been shown to be a safe procedure, with good results after three months of follow-up.
In this observational study, left bundle branch stimulation is shown as a effective procedure, managing to improve ventricular function, safe and reproducible, carried out by Intensivistas, in a Regional Hospital.
The study and the article have not received any funding.
There is no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
