
Research Article | DOI: https://doi.org/10.31579/2641-0419/429
1 Bundeswehr Zentralkrankenhaus Koblenz, Klinik IA, Rübenacher Str. 170, 56072 Koblenz, Germany.
2 GFO Klinken Bonn, Robert-Koch-Str. 1, 53115 Bonn, Germany.
# Both authors contributed equally.
*Corresponding Author: Heyder Omran, GFO Kliniken Bonn, Robert-Koch-Str. 1, 53115 Bonn.
Citation: Jaroslaw Heinrich, Jörg Kamlah, Heyder Omran, (2024), Left Atrial Appendage Occlusion: Analyzing Factors for Peridevice Leak with Dual-Occlusive Devices, J Clinical Cardiology and Cardiovascular Interventions, 7(16); DOI: 10.31579/2641-0419/429
Copyright: © 2024, Heyder Omran. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 November 2024 | Accepted: 10 December 2024 | Published: 31 December 2024
Keywords: Left atrial appendage occlusion; dual-occlusive device; 3D transesophageal echocardiography; peridevice leakage; off-axis; compression
Background: This study examines factors influencing peridevice leak (PDL) in patients treated with the Amplatzer Amulet Occluder for left atrial appendage occlusion (LAAO).
Materials and Methods: A retrospective analysis was conducted on 217 patients who underwent successful LAAO with the Amplatzer Amulet Occluder due to atrial fibrillation and anticoagulation contraindications. Follow-up transesophageal echocardiography (TEE) was performed 1-3 months post-procedure to detect PDL and analyze related procedural and anatomical factors.
Results: PDL occurred in 42% of patients, predominantly mild (<3 mm). Key factors associated with increased PDL risk included occluder compression <12%, off-axis device positioning, and device size ≥25 mm. Baseline patient characteristics and procedural details did not significantly impact PDL rates.
Conclusion: For optimal LAAO outcomes, pre- and periprocedural assessment of LAA size and device positioning is crucial. Ensuring occluder compression above 15% may minimize PDL risks, especially for larger devices.
DRT = device related thrombus
LAA = left atrial appendage
LAAO = left atrial appendage occlusion
MAE = major adverse events
PDL = peridevice leaks
(3D-) TEE = (Three dimensional-) transesophageal echocardiography
One of the most common cardiac arrhythmias, especially atrial tachycardia, is atrial fibrillation. It is presented with a prevalence of 1-2% in population, rising by age continuously (15% in men above 80 years of age) (1, 2). Well known, atrial fibrillation increases the imminent risk of ischemic thromboembolism, developed predominantly in the left atrial appendage (LAA), in all parts of the atrial system (3). Amongst all, stroke is the most feared undesirable event (4).
Oral anticoagulants, such as anti-factor Xa inhibitors, thrombin inhibitors, and vitamin K antagonists, represent a contemporary first-line strategy for prevention of thromboembolism. To minimize bleeding risks, however, patients should first be evaluated using anticoagulation scoring systems, such as CHA2DS2-VASc (≥2) and HAS-BLED (≤2) (5-8).
In patients with contraindications to oral anticoagulation, older studies such as PROTECT AF (9), PREVAIL (10) and Prague-17 (11) have already demonstrated the non-inferiority of left atrial appendage occlusion (LAAO) compared to anticoagulation, which is reflected in a Class IIB recommendation in the 2024 ESC Guideline (12) and Class IIA recommendation in the 2023 ACC/AHA/ACCP/HRS Guideline (13). Current randomized studies could upgrade these recommendations in favor of LAAO in the coming years (14).
There are two main types of LAA closure devices: the single-occlusive device, represented by, among others, the Watchman (Boston Scientific, Boston), and the Amplatzer Amulet as a dual-occlusive device (Abbott, Boston) (22). Since the inception of interventional LAAO, the occurrence of peridevice leaks (PDL) and device-related thrombus (DRT) has remained a challenge in some cases.
Ironically, PDLs, have been identified as influencing factors for systemic thromboembolism (15) and the formation of DRT (16), which in turn has emerged as a primary cause of ischemic strokes (17). In cases of severe PDL a second occluder might even become an option (18) next to vascular plugs, embolic coils or radiofrequency ablation leading to a second intervention for the patient with possible additive adverse events.
Factors influencing the formation of PDL include, among others, LAA size and anatomy, device undersizing, off-axis implantation (19), and volume loading (20).
As an experienced center in the implantation of dual-occlusive devices, specifically the Amplatzer Amulet, we investigated factors influencing the formation of PDL in this study, with the aim of anticipating these factors in the future and ideally preventing the development of PDL in advance.
1.1 Study Design
In this single-center study, we examined a total of 217 consecutive patients who underwent a successful LAAO with the Amplatzer Amulet Occluder between September 2015 and January 2023 due to atrial fibrillation and contraindications to oral anticoagulation. All patients attended a follow-up 3D transesophageal echocardiography (TEE) 1-3 months post-procedure (22). The primary objective of this investigation was to identify factors influencing the development of PDL. We collected data on baseline characteristics, clinical and laboratory features, pre-LAAO medication, bleeding risk factors, LAAO indications, implantation characteristics, and periprocedural adverse events up to discharge according to the Munich consensus document (21). Additionally, TEE characteristics of the LAA were documented during the procedure and at the first follow-up TEE as described below. All patients had no severe leaks on periprocedural TEE and met the criteria for device success.
2.2 Procedural data
At least 24 hours before the index LAAO procedure, patients underwent TEE to screen for thrombi in the LAA and to assess the overall feasibility of occluder implantation. All procedures were performed under general anesthesia using contrast angiography and TEE (GE Vivid E9 BT12). We recorded the volume of contrast medium (ml), fluoroscopy time (minutes), and radiation dose (cGy*cm²) using DAVID hemodynamic software. The procedure duration, measured in minutes, concluded with patient extubation. The procedure was conducted in accordance with the manufacturers' guidelines.
TEE Review
An experienced examiner retrospectively analyzed high-quality 3D-TEE images using the GE EchoPAC BT12 software based on the stored images to provide the most detailed insights possible into the research question. Incomplete data sets were excluded.
In the first step, the morphology of LAA was assessed from the periprocedural TEE using the 12-channel multislice mode, which allows for a 3D reconstruction of the LAA, following the established definitions (22).
Next, the orifice area, representing the immediate opening of the LAA, and the landing zone, extending from the left circumflex coronary artery to 10 mm into the LAA from the left superior pulmonary vein, were measured. The mean diameter (D average) was calculated using the perimeter (Dper) with the formula "Dper = P/π". The depth of the LAA was defined as the shortest orthogonal distance from the landing zone to the LAA roof (21).
In the follow-up TEE, the focus was on detecting PDL, which were classified as mild (< 3> 5 mm). Additionally, DRT, transseptal shunts, off-axis positioning of the occluder, and occluder compression in the LAA were evaluated.
Color-flow Doppler was used to detect leaks around the LAA occluder in the form of residual color jets that were visible despite the occluder being in place. The same methodology was applied to identify transseptal shunts. Device-related thrombus was defined as an echogenic, well-demarcated formation on the occluder.
Off-axis positioning was identified when the disc and the central waist, which connects to the main body of the occluder, did not form a right angle, implicating a tilting of the occluder. Occluder compression was defined as the maximum extent of the occluder within the LAA and was calculated as the ratio of the implanted occluder size, documented as a percentage.
Statistical Analysis
Continuous variables were expressed as means ± standard deviations and analyzed using the Student's t-test for normally distributed data. For non-normally distributed data, the Mann-Whitney U test was employed. Categorical variables were reported as absolute counts and percentages, with comparisons made using the chi-square test. Statistical significance was defined as a two-sided p-value of < 0>
3.1 Patient Characteristics
Among the total cohort of 217 patients who received an Amplatzer Amulet Occluder, 91 patients, or 42%, exhibited at least one mild leak (< 3>
As shown in Table 1, none of the aforementioned parameters, including comorbidities, medication, laboratory values, the CHA2DS2-VASc score, the HAS-BLED score, or atrial fibrillation classification, had a significant impact on the occurrence of leaks.
| Table 1. Patient Characteristics | ||||
| . | Overall Cohort n= 217 (%) | Leaks n= 91 (%) | No leaks n= 126 (%) | p value |
| Age (years) | 77.41±7.19 | 77.73±7.07 | 77.18±7.29 | 0.58 |
| Age≥75 (years) | 149 (69) | 66 (73) | 83 (66) | 0.30 |
| Male | 110 (51) | 49 (54) | 61 (48) | 0.43 |
| Body mass index (kg/m2) | 27.05±4.74 | 26.33±4.09 | 27.57±5.11 | 0.13 |
| Height (cm) | 170.09±9.20 | 170.79±8.70 | 169.59±9.55 | 0.35 |
| Weight (kg) | 78.51±15.57 | 77.02±13.45 | 79.58±16.93 | 0.23 |
| CHA2DS2VASC score | 4.55±1.52 | 4.55±1.57 | 4.56±1.48 | 0.98 |
| HASBLED score | 3.80±1.09 | 3.73±1.02 | 3.86±1.13 | 0.38 |
| Atrial fibrillation | ||||
| Paroxysmal | 117 (54) | 47 (52) | 70 (56) | 0.57 |
| Persistent | 24 (11) | 10 (11) | 14 (11) | 0.98 |
| Permanent AF | 76 (35) | 34 (37) | 42 (46) | 0.54 |
| Clinical features | ||||
| Coronary artery disease | 87 (40) | 38 (42) | 49 (39) | 0.67 |
| Myocardial infarction | 29 (13) | 11 (12) | 18 (14) | 0.64 |
| PCI | 50 (23) | 24 (26) | 26 (21) | 0.32 |
| CABG | 18 (8) | 7 (8) | 11 (9) | 0.78 |
| Heart failure | 68 (31) | 30 (33) | 38 (30) | 0.66 |
| Arterial hypertension | 180 (83) | 74 (81) | 106 (84) | 0.59 |
| Pacemaker | 36 (17) | 18 (20) | 18 (14) | 0.28 |
| Diabetes mellitus | 59 (27) | 19 (21) | 40 (32) | 0.08 |
| Hyperlipidemia | 86 (40) | 35 (38) | 51 (40) | 0.77 |
| COPD | 38 (18) | 15 (16) | 23 (18) | 0.74 |
| Nikotin | 53 (24) | 19 (21) | 34 (27) | 0.26 |
| Hemoglobin (g/dl) | 11.70±2.32 | 11.50±2.38 | 11.85±2.27 | 0.26 |
| Creatinine (mg/dl) | 1.29±0.90 | 1.31±0.94 | 1.28±0.87 | 0.83 |
| GFR (ml/min) | 58.96±23.18 | 58.49±23.26 | 59.30±23.21 | 0.80 |
| Quick (%) | 87.26±22.19 | 86.70±22.47 | 87.66±22.07 | 0.76 |
| INR | 1.12±0.22 | 1.12±0.20 | 1.12±0.23 | 0.94 |
| PTT (sec) | 26.89±5.98 | 26.83±5.39 | 26.93±6.42 | 0.90 |
| Medication before LAAO | ||||
| ASA | 39 (18) | 17 (19) | 22 (17) | 0.82 |
| Clopidogrel | 15 (7) | 7 (8) | 8 (6) | 0.70 |
| ASA + Clopidogrel | 4 (2) | 2 (2) | 2 (2) | 0.74 |
| Vitamin K antagonist | 16 (7) | 4 (4) | 12 (10) | 0.15 |
| Noval oral anticoagulant | 108 (50) | 46 (51) | 62 (49) | 0.85 |
| Low molecular weight heparin | 24 (11) | 11 (12) | 13 (10) | 0.68 |
| Beta blocker | 166 (77) | 68 (75) | 98 (78) | 0.60 |
| Statin | 110 (51) | 42 (46) | 68 (54) | 0.26 |
| Diuretic | 146 (67) | 65 (71) | 81 (64) | 0.27 |
| ACE inhibitor | 53 (24) | 25 (27) | 28 (22) | 0.37 |
| Sartane | 85 (39) | 37 (41) | 48 (38) | 0.70 |
| Risk factors for bleeding | ||||
| Previous stroke | 47 (22) | 21 (23) | 26 (21) | 0.67 |
| TIA | 7 (3) | 4 (4) | 3 (2) | 0.41 |
| Prior major bleeding | 112 (52) | 51 (56) | 61 (48) | 0.27 |
| Renal disease | 92 (42) | 35 (38) | 57 (45) | 0.32 |
| Liver disease | 15 (7) | 6 (7) | 9 (7) | 0.86 |
| Labile INR | 5 (2) | 1 (1) | 4 (3) | 0.32 |
| Age>65 | 204 (94) | 87 (96) | 117 (93) | 0.40 |
CAD: coronary artery disease; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft; COPD: chronic obstructive pulmonary disease; GFR: glomerular filtration rate; INR: international normalized ratio; PTT: prothrombin time; ASA: acetylsalicylic acid; ACE: Angiotensin-Converting-Enzyme; TIA: transitory ischemic attack
The primary indication for LAAO was previous bleeding events, with the majority being major bleeds (52%). The occurrence of leaks did not differ significantly in this regard (see Table 2).

3.2 Procedural Data
The procedure time averaged 70.36 ± 30.87 minutes, with a contrast medium usage of 80.30 ± 39.96 ml, fluoroscopy time of 11.82 ± 33.20 minutes, and radiation dose of 1692.15 ± 1689.60 cGy*cm². There were no significant differences between groups with and without leaks. Hospital stay averaged 6.27 ± 3.95 days, with no significant differences between the groups.
The most significant factor influencing leaks was the size of the implanted occluder. Occluders in the leak group were significantly larger (23.51 ± 3.81 mm for leaks vs. 22.25 ± 3.90 mm for no leaks; p = 0.02). Specifically, occluders > 25 mm were significantly more associated with leaks (51% for leaks vs. 37% for no leaks; p = 0.04) (see Table 3).
| Table 3. Procedural data | ||||
| . | Overall Cohort n= 217 (%) | Leaks n= 91 (%) | No leaks n= 126 (%) | p value |
| Procedure time (min) | 70.36±30.87 | 70.03±31.05 | 70.60±30.86 | 0.90 |
| Contrast medium (ml) | 80.30±39.96 | 79.53±44.34 | 80.87±36.64 | 0.81 |
| Fluoroscopy time (min) | 11.82±33.20 | 12.75±36.55 | 11.17±30.75 | 0.73 |
| Radiation dose (cGy∗cm2) | 1692.15±1689.60 | 1493.27±1484.03 | 1832.64±1813.51 | 0.15 |
| More than 1 device tried | 2 (1) | 1 (1) | 1 (1) | 0.82 |
| Final Occluder implanted (mm) | 22.77±3.90 | 23.51±3.81 | 22.25±3.90 | 0.02 |
| Final Occluder > 25 mm | 92 (42) | 46 (51) | 46 (37) | 0.04 |
| Hospital stay (days) | 6.27±3.95 | 6.46±3.95 | 6.13±3.97 | 0.54 |
3.3 Periprocedural Adverse Events
As shown in Table 4, the incidence of major adverse events (MAEs) was minimal. Cardiac tamponade and major bleeding were the most frequent, occurring in 2 cases each, but there were no significant differences between the groups. The most common minor adverse events were vascular complications, occurring in 6% of cases, also without significant differences between the groups.

3.4 TEE Analyses
The periprocedural anatomical characteristics of the LAA, including morphology, landing zone, orifice area, and depth, did not significantly impact the occurrence of leaks (see Table 5).

However, the TEE follow-up (Table 6) revealed different results. Minor leaks accounted for 34% of all leaks, followed by 6% moderate leaks and 2% severe leaks. The most significant factors influencing leaks were off-axis positioning of the occluder (32% for leaks vs. 12% for no leaks; p < 0 xss=removed>
 Transseptal shunts occurred in 30% of cases, but there was no statistical significance between the groups. Interestingly, DRT were more frequent in the group with no leaks (n=4 (3%) for no leaks vs. n=1 (1%); p = 0.32), although this difference was not statistically significant.
Transseptal shunts occurred in 30% of cases, but there was no statistical significance between the groups. Interestingly, DRT were more frequent in the group with no leaks (n=4 (3%) for no leaks vs. n=1 (1%); p = 0.32), although this difference was not statistically significant.
In our retrospective study, we examined a cohort of patients who received the Amplatzer Amulet Occluder, focusing on risk factors for the development of PDL in the first TEE, performed 1–3 months after the index procedure. To avoid interobserver variance, the 3D-TEE images from the hospital’s Picture Archiving and Communication System (PACS) were re-evaluated by an experienced cardiologist.
The results revealed three major risk factors for the development of PDL with the Amplatzer Amulet Occluder:
1. A compression of the occluder less than 12% within the LAA
2. A final occluder size of ≥ 25 mm (see image 01)
3. An off-axis position of the disc relative to the occluder’s body (see image 02)
Baseline characteristics, such as age, gender, comorbidities, pre-procedure medication, LAAO indications, as well as procedural data and complications during the hospital stay, did not play a significant role as risk factors in our cohort.

Image 01: TEE 100° view, large occluder, 31 mm Amplatzer Amulet, 25 % compression, mild leak
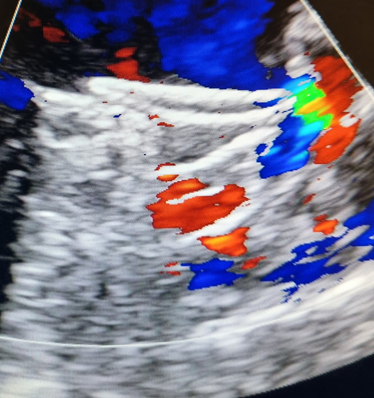
Image 02: TEE 90° view, off-axis position, 28 mm Amplatzer Amulet, 23 % compression, moderate leak
In contrast, Price et al. (15), in the Amulet IDE Trial, identified a higher CHA2DS2-VASc score and non-paroxysmal atrial fibrillation as significant risk factors for PDL. It is worth noting that these factors were only associated with single-occlusive devices. Besides, Mansour et al. (23) also identified male gender as a significant factor in a small study.
Similar to our findings, Nguyen et al. (24) and Lakkireddy et al. (19) found that a “chicken wing” LAA anatomy did not pose a risk factor for PDL, although one might have expected that the chicken wing morphology, characterized by a bent body, could complicate correct positioning of the Amplatzer Amulet device.
The incidence of severe leaks (>5mm) in our study was 2%, which aligns with rates from the Amulet IDE Trial (1.1%) (26) and Mansour et al. (3.8%) (23) but was higher than in an earlier study by Saw et al. (25), where a rate of 0.6% was reported for the Amplatzer Cardiac Plug, the predecessor of the Amulet.
There are conflicting results concerning the relevance of compression in PDL development. While we observed significantly more leaks with a compression rate below 12%, the Amulet IDE Trial (26) did not identify a significant difference even in severe leaks, whether with single- or dual-occlusive devices. Nguyen et al. (24), however, supported our findings, identifying a compression rate of less than 10% as a significant factor. Periprocedurally, we calculate the diameter derived from the perimeter and add 15% to this diameter for optimal occluder compression within the LAA, as recommended in the instructions for use.
One possible explanation for undersizing could be insufficient periprocedural volume preload due to pre-procedure fasting, which is standard for interventional procedures. Both Zhang, Cong et al. (2019) (27) and Al-Kassou, Tzikas et al. (2017) (20) demonstrated in the past significant differences in LAA volume based on patients’ volume status using 3D-TEE.
An off-axis position of the occluder within the LAA, often indicating a tilted position of the occluder’s body, has been identified as a contributing factor to PDL in several studies for both the Watchman and Amplatzer Amulet Occluders (19, 28, 29). We were able to confirm this finding with significant results in our cohort as well (32% for leaks vs. 12% for no leaks; p < 0>
Furthermore, the occluder’s size was critical in our study. A larger occluder (≥ 25 mm in diameter) exhibited lower compression rates. In our cohort, although compression below 15% alone did not maintain statistical significance for PDL (59% for leaks vs. 46% for no leaks; p = 0.053) and only became significant below 12% (p < 0 xss=removed xss=removed xss=removed mm, p = 0.003)>
In a 5-year outcome study, Dukkipati et al. (2022) (32) found a significantly increased risk of ischemic stroke or systemic embolism with smaller leaks (≤ 5mm) for the Watchman. Over a shorter follow-up of 18 months, Price et al. (2022) (15) in the Amulet IDE Trial observed similar results for both single- and dual-occlusive devices for PDLs <3mm>3mm, although the hazard ratio was higher for single-occlusive devices. Thus, even small PDLs are clinically relevant and should be minimized.In optimizing LAAO planning, modern technology can assist. For example, virtual reality is helpful in improving pre-procedural planning (33). Ideally, the device should fully occupy the left atrial appendage, making 3D-printing a promising option currently under investigation (34).
The rate of severe PDLs (>5mm) with a dual-occlusive device is low. Large LAAs require precise pre- and periprocedural assessment of LAA anatomy. Specifically, an occluder compression of at least 15% should be ensured when selecting the device, with consideration that inadequate intravascular volume during the procedure can lead to device undersizing.
The rate of severe PDLs (>5mm) with a dual-occlusive device is low. Large LAAs require precise pre- and periprocedural assessment of LAA anatomy. Specifically, an occluder compression of at least 15% should be ensured when selecting the device, with consideration that inadequate intravascular volume during the procedure can lead to device undersizing.
The primary limitation of our study is its retrospective design. Additionally, we only had a short follow-up period, examining echocardiographic PDL occurrence but not its clinical consequences concerning adverse events, in the first TEE performed 1–3 months after the index procedure. Our results are also applicable solely to dual-occlusive devices.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
