
case report | DOI: https://doi.org/10.31579/2639-4162/066
1MBBS (National University of Singapore – Yong Loo Lin School of Medicine);
2FRCS (A&E), MBBS, FAMS (Em Med), Senior Consultant, Dept of Emergency Medicine, Singapore General Hospital. Professor, Duke NUS Graduate Medical School, Yong Loo Lin School of Medicine, National University of Singapore and Lee Kong Chian Medical School, Nanyang Technological University. Director, Sing Health Duke NUS Institute of Medical Simulation (SIMS), Singapore.
*Corresponding Author: Fatimah Lateef, Senior Consultant, Dept of Emergency Medicine, Singapore General Hospital. Professor, Duke NUS Graduate Medical School, Yong Loo Lin School of Medicine, National University of Singapore and Lee Kong Chian Medical School, Nanyang Technologi
Citation: Wei Quan Tan, Lyn Hui Wen Yeo and Fatimah Lateef. (2022) Lead AVR: Under-appreciated and Often Overlooked. Journal of General medicine and Clinical Practice, 5(3); Doi: 10.31579/2639-4162/066
Copyright: © 2022 Fatimah Lateef, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 June 2022 | Accepted: 28 June 2022 | Published: 06 July 2022
Keywords: electrocardiography; st-elevation acute myocardial infarction; acute coronary syndromes
Electrocardiography (ECG) is one of the most common investigations carried out to evaluate the initial functional status of the heart. It is simple, generally reliable and rapid, providing critical information that can drastically alter diagnostic probabilities. Its sensitivity and specificity for diagnosing different clinical conditions do vary and is context specific.
Electrocardiography (ECG) is one of the most common investigations carried out to evaluate the initial functional status of the heart. It is simple, generally reliable and rapid, providing critical information that can drastically alter diagnostic probabilities. Its sensitivity and specificity for diagnosing different clinical conditions do vary and is context specific. [1] ECG is done in various healthcare settings for the evaluation of numerous conditions. Some may be linked to time-dependent diagnoses, eg. ST-Elevation Acute Myocardial Infarction (STEMI) and thus requires quick recognition and familiarity. Early recognition of specific patterns on the electrocardiogram can make the difference between life and death. As such, the skill of interpreting an electrocardiogram is essential to any medical professional.
The traditional reading of the ECG often did not place much emphasis on
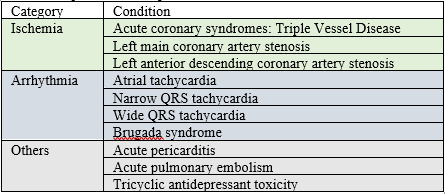
lead aVR. [2] With the explosion of medical knowledge and research in recent times, the previously neglected aVR has been gaining prominence and importance. First and foremost, there has been much interest in how aVR can be useful in the localization of obstruction in acute coronary syndrome: specifically looking at left main coronary artery occlusion, proximal left anterior descending artery stenosis, as well as severe triple vessel disease [2]. Besides its utility in acute coronary syndromes, aVR could potentially provide valuable information regarding other non-coronary artery disease conditions. These other conditions are wide ranging, from acute pericarditis to tricyclic antidepressant poisoning, often not getting as much attention as the acute coronary syndromes. We aim to summarize several pertinent non-coronary artery disease applications of lead aVR, and to highlight the key electrocardiographic features of each condition. (Table 1)
Acute Pericarditis (Figure 1)
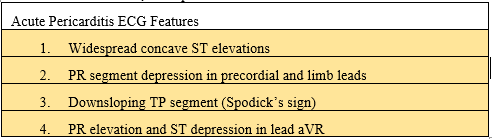
The electrocardiogram is a key tool in the evaluation of acute pericarditis. Clinicians classically look for widespread concave ST segment elevations accompanied by PR segment depression throughout both the precordial and limb leads [2]. Another feature that has often been cited is Spodick’s sign which is characterized by a downsloping TP segment. [3] Lead aVR offers important diagnostic utility for patients with acute pericarditis: the pattern of reciprocal PR elevation and ST depression in the right clinical context is suggestive.[4-6]
Given that ST elevations are commonplace in both acute pericarditis and STEMI, it is paramount to look for clues to differentiate between the two conditions. Lead aVR provides key information in this aspect. Features suggestive of STEMI include ST elevation in lead III > II, ST depressions in leads other than aVR or V1, upward convexity of ST segment elevation. [7] These patterns should always raise suspicion of a STEMI and efforts need to be undertaken to rule out a STEMI accordingly. Clinical correlation is also useful.
Another potential mimic is the entity known as Benign Early Repolarization (BER), which can also present with generalised concave ST segment elevations. Features more suggestive of BER include ST elevations localized to the precordial leads, notched J point (known as a ‘fish hook’ appearance), absence of PR depression and an ST segment elevation/T wave ratio of less than 0.25. [8] It is important to note that the ST segment elevation amplitude is measured from the end of the PR segment to the J point.
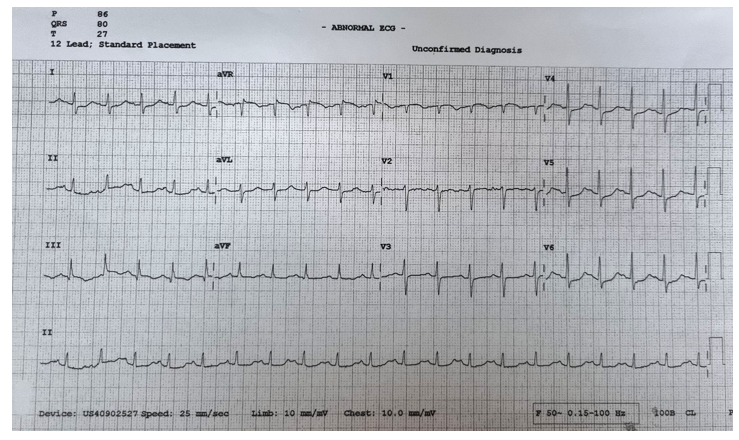
Acute Pulmonary Embolism (Figure 2)
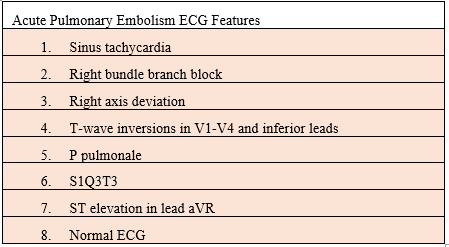
While there are many different electrocardiogram findings that may be observed in a patient with acute pulmonary embolism (PE), none of them are sensitive enough to rule out or specific enough to rule in the condition. [1, 9] Features that may be present include sinus tachycardia, nonspecific ST segment and T wave changes, partial or complete right bundle branch block, right axis deviation, T wave inversions in V1-V4 and inferior leads suggestive of right ventricular strain, and P pulmonale suggestive of right atrial enlargement. [10] The ‘classical’ finding of S1Q3T3 is in fact uncommon in PE, and so is ST elevation in lead aVR. Some patients with PE have an entirely pristine or normal ECG. [10, 11]
The usefulness of electrocardiography in PE is in raising the suspicion of the condition in the right clinical situation; as well as in prognosticating the severity of PE as well as in risk stratification. [12] ST elevation in lead aVR has recently been linked to cardiopulmonary instability [13] and right ventricular (RV) dysfunction in patients diagnosed with acute pulmonary embolism. This may have implications on anticipating RV dysfunction early in the course of PE which may impact management decisions. [11] In addition, studies have also shown that patients with ST elevation also have a higher risk of overall mortality, and in-hospital complications. [12] Evidently, ST elevation in aVR has major prognostic value for acute PE patients.
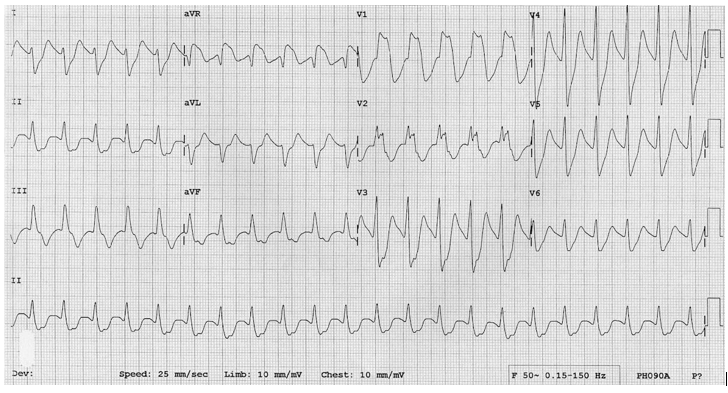
Tricyclic Antidepressant (TCA) overdose (Figure 3)
TCAs are still used in clinical medicine today despite the widespread adoption of Selective Serotonin Reuptake Inhibitors (SSRIs) for the treatment of clinical depression. Beyond depression, TCAs are used in other conditions, ranging from psychiatric conditions such as obsessive compulsive disorder to chronic pain disorders such as migraine and neuropathic pain. [14-16] Overdose is a potentially lethal condition that needs to be rapidly picked up and treated. TCAs can be fatal at doses as low as ten times the daily dose. [17] Failure to detect TCA overdose in a timely manner may result in significant risk of cardiovascular toxicity (hypotension and arrhythmias) and neurological toxicity (mental status changes and seizures). The ECG is helpful in determining the extent of TCA overdose. [18]
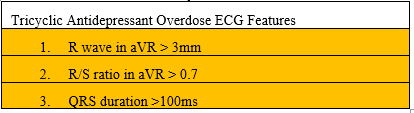
The classic ECG findings of TCA overdose were coined in 1995 by Liebelt et. al, which include R wave in aVR > 3mm and R/S ratio in aVR > 0.7, and QRS duration >100ms. [19] It was found that the findings of the R wave and R/S ratio in aVR were better predictors of the severity of TCA poisoning than the QRS duration [20]. However, reports on TCA overdose have mainly used the QRS duration of >100ms as an indication for sodium bicarbonate therapy [21]. One postulation would be the relative ease of assessment of the QRS duration compared to the R/S ratio and the R wave. Further studies can be considered to elucidate any possible clinical implication of the R wave and R/S ratio in clinical practice.
Regular Wide QRS Complex Tachycardias (WCT)
For the scope of this paper we have chosen to focus on regular WCT in view of clinical relevance. A fundamental question to answer in the approach to such an arrhythmia is whether the patient has a ventricular tachycardia (VT) or a supraventricular tachycardia (SVT) with aberrancy or a bundle branch block. This dichotomy, while critical, is not simple to make. [22, 23]
The urgent need to differentiate between both reliably has given birth to the development of several criterias over the years, the most widely adopted and practiced being the Brugada criteria. [24] Other approaches have surfaced such as the Vereckei approach and the Limb Lead Algorithm [25], with merits of their own. In 2007, Vereckei proposed an update to his earlier algorithm, emphasizing the central role of the aVR lead in the analysis of WCT, which showed better sensitivity and negative predictive value compared to the Brugada algorithm. [26] In 2017, a prospective study by Jain et al found that the updated aVR Vereckei algorithm was indeed more sensitive for the differential diagnosis of WCT compared to the Brugada criteria. [27] That being said, there has
been some doubt regarding the practical utility of the Vereckei criteria based on a study in 2012 done by Baxi et al where emergency medicine residents achieved only fair-to-good individual accuracy and moderate agreement while using the Vereckei criteria, with a suggestion of further simplification of the criteria before clinical implementation. [28] More studies are required to compare the utility of different WCT algorithms in various clinical settings. [23, 29]
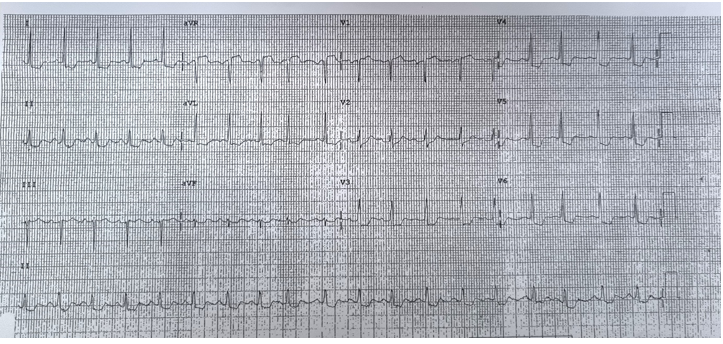
aVR is a lead that is relatively overlooked when approaching ECGs. Besides its increasing recognition and importance in acute coronary syndrome [Fig 4], practitioners reading ECGs should make it a point to screen lead aVR as part of their standard ECG reading approach. With the emergence of new evidence and increasing interest in aVR, it is increasingly recognized to have much diagnostic and prognostic significance of certain patterns in aVR across various conditions. It would be both useful and interesting to further investigate its use in clinical decision making, especially specific to certain cohorts of patients. This can eventually lead to better patient outcomes.
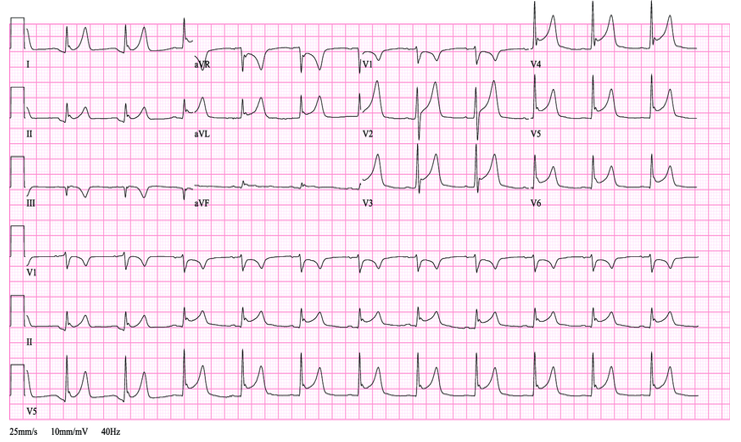
Widespread concave ST elevation
PR segment depression in Leads 1, II, V5, V6
Spodik Sign of downsloping TP segment best seen in Leads II, V2 to V6
In Lead aVR: Elevation of the PR segment and depression of the ST segment
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
