
Case Report | DOI: https://doi.org/10.31579/2690-1897/126
General surgery, Armed Forces Hospital, Muscat, Oman
*Corresponding Author: Raya Al Shaaibi, General surgery, Armed Forces Hospital, Muscat, Oman
Citation: Raya Al Shaaibi, Smitha, Amani Al Saidi and Salma Al Shamsi. (2022) Lateral neck malignant cyst. J, Surgical Case Reports and Images 5(4); DOI:10.31579/2690-1897/126
Copyright: © 2022, Raya Al Shaaibi, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 September 2022 | Accepted: 26 September 2022 | Published: 10 October 2022
Keywords: branchial cyst; papillary thyroid carcinoma
Branchial cysts are the most common lesions in lateral neck cysts. Rare branchial cysts are associated with malignant tumors metastatic from the thyroid gland. Occult thyroid papillary carcinomas often present as a solid mass in the lateral neck, with only a few cases revealing a branchial cyst as the initial manifestation.
Branchial cleft cysts are the most common congenital neck masses arising laterally. The majority of branchial cleft cysts are benign. Branchial cleft cysts can contain malignant tissue, including papillary thyroid carcinoma. We present a case of branchial cyst with papillary cancer and the discovery of micro-papillary thyroid carcinoma one year after the initial diagnosis of branchial cyst.
R.M is a 20-year-old female, presenting to the surgical outpatient department with a 7-month history of right-sided neck swelling with no other complaints. On examination, she had a 4 x 3 cm cystic, nontender swelling in the lateral side of her sternocleidomastoid, fixed with a smooth surface, not attached to the skin, and no palpable cervical lymphadenopathy.
Ultrasound of the neck showed a 4.8 x 2.6 cm cystic lesion with internal moving echoes seen on the right side of the neck, which may represent a 2nd branchial cleft cyst. An 8 x 6 mm small soft tissue echogenicity adherent along its posteromedial wall may represent a mural soft tissue nodule or adherent debris.
No cervical lymphadenopathy was seen. A CT scan revealed the same finding. Intra-operatively, a solitary cystic mass containing dark fluid was found (figure 1).
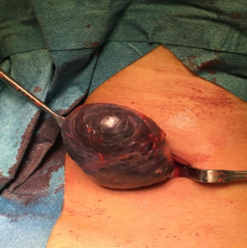
Figure1: Intra-operative finding
The specimen was sent for histopathological examination and found to be cystic papillary carcinoma. The patient was followed up with a serial ultrasound of the neck to detect the primary site. All were reported as normal studies. One year after the first presentation, ultrasound showed a small ill-defined hypoechoic nodule measuring 3.7 x 3.1 mm noted in the lateral aspect of the right lobe with no evidence of internal vascularity or micro-calcification within the nodule. No cervical lymphadenopathy was detected. Ultrasound guided fine needle aspiration was done and reported as papillary carcinoma of the thyroid (papillary micro-carcinoma). Consequently, total thyroidectomy was done for the patient.
Papillary thyroid microcarcinoma is a subgroup of papillary thyroid carcinoma defined by the World Health Organization as having a dimension of 1.0 cm or less. PTMs are usually incidentally found in radiological investigations or in histopathological examinations for benign thyroid diseases [1]. Papillary thyroid cancer is common thyroid tumors with metastatic potential. These tumors may be occult and may present with asymptomatic congenital neck masses. Management is controversial as PTMs do not frequently become clinically apparent. Patients can be under observation while their tumors are not progressing. However, they are pathologically multifocal and involve lymph nodes in high incidence [2].
Branchial cyst is a lateral neck mass resulting from the proliferation of epithelial remnants of the second branchial arch or the cervical sinus. It is a common congenital anomaly in the pediatric age group, representing 20% of cervical lesions in children [3]. Lateral cyst mass usually is a benign lesion. However, when it presents in patients above 40 years it raises the suspension of malignancy, which most likely is metastatic from primary cancer in the upper aerodigestive tract [4]. In case of histopathology came as squamous cell carcinoma, primary tumors were discovered by pan-endoscopy before neck surgery with tonsillectomy and mapping biopsies [5].
The metastatic cystic lesion was discovered incidentally in 4% to 22% of cases with a primary diagnosis of branchial cyst [2,6,7,8,9]. Radiographic evaluation by ultrasound and CT scan can address the diagnosis, but histopathology investigation is essential to confirm it [10]. A malignant lateral cervical cystic lesion without the presence of a primary origin can be defined as branchiogenic carcinoma, as a malignancy arising from a branchial cyst [11].Branchiogenic carcinoma is first described by Von Volkmann in 1882 as malignant transformation of branchial cyst epithelium, which has a lot of controversies in the literatures [12].More attention is drown to the association between solitary cystic neck mass and occult primary source in the tonsils or the base of the tongue and can be detected after performing an ipsilateral tonsillectomy or biopsy for the base of the tongue [13]. However to conclude the diagnosis of branchiogenic carcinoma, no primary source should be detected after 5 years from the diagnosis and the histological appearance of the tumor must be similar to the histology of branchial vestige.[i] PTC metastasis to a branchial cleft cyst has been reported in the literature, where the patient underwent excision of a branchial cleft cyst with unexpected histological that consistent with PTC [15].
Histopathological examination of lateral neck cyst may demonstrate the presence of lymph tissue, which makes it difficult to discriminate between cystic lymph nodes and branchial cysts [16]. Moreover, the lateral anlage of the thyroid develops from the fourth-fifth branchial pouch with the possibility of entrapping normal thyroid tissue presenting as a branchial cyst with ectopic thyroid tissue. As described in the literature, thyroid cancers can present in the ectopic sites, such as a branchial cyst, the diagnostic dilemma is whether it of occult primary carcinoma or the presence of metastatic disease [17]. These cystic changes and unknown primary carcinoma could explain the pathophysiology in our case.
Unusual neck cysts in adult patients should raise the suspicion of malignancy. Assessment needs to be completed by imaging and FNAC or excisional biopsy is essential to confirm the diagnosis and proper management of the patient. All benign congenital lesions should be thoroughly examined for the possibility of containing occult carcinomas.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
