
Research Article | DOI: https://doi.org/10.31579/2694-0248/017
Department of Orthopaedic Surgery. Full profesor. University Hospital Manuel Ascunce Domenech. Camagüey City. Cuba.
*Corresponding Author: Alejandro Alvarez López , Department of Orthopaedic Surgery. Full profesor. University Hospital Manuel Ascunce Domenech. Camagüey City. Cuba.
Citation: Alejandro Alvarez López (2022). Lateral Knee Osteoarthritis. J. Clinical Orthopedics and Trauma Care, 4(1); Doi:10.31579/2694-0248/017
Copyright: © 2022 Alejandro Alvarez López, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 November 2021 | Accepted: 20 December 2021 | Published: 03 January 2022
Keywords: lateral knee osteoarthritis; valgus angular deviation; arthroscopy; osteotomy; partial and total knee replacement
Background: gonarthrosis is a common entity characterized by involvement of one or more compartments, of which the lateral one is the one with the lowest incidence in isolation.
Aim: the aims of this research are too updated on the most important features on lateral knee osteoarthritis and look for updated bibliography on the subject.
Methods: PubMed, Hinari, SciELO and Medline databases were searched for citations from August 1st 2021 to September 30th 2021 using the EndNote search manager and reference manager. Out of 312 articles, 44 selected citations were used in this review, being 42 of the last five years.
Results: the main causes of lateral knee osteoarthritis are mentioned, especially the secondary ones. Reference is made to the main clinical and imaging elements for diagnosis based on plain radiography and magnetic resonance imaging. Both conservative and surgical treatment modalities are exposed, in the latter the main indications and complications are described, among which osteotomies and arthroplasties stand out.
Conclusions: lateral gonarthrosis is the least common of the unicompartmental gonarthrosis that affect the knee joint. Clinical and imaging diagnosis provides the essential elements for both conservative and surgical therapeutic behaviour, the latter modality includes techniques that preserve the joint such as osteotomies and others that do not, such as arthroplasties.
Osteoarthritis is the most common degenerative and progressive joint disease. It affects millions of people and involves joints such as the hips, spine and knees with a high economic cost.
The knee is one of the most affected joints by this degenerative entity, the main symptoms and signs are mechanical pain with swelling and limitation of joint movement to different degrees, accompanied by crepitus and locking. [1, 2]
A simple X-ray is the most used test to confirm the diagnosis; it stands out due to its low cost and high availability. Radiographs may show the classic signs of joint space narrowing, sclerosis, subchondral cysts, osteophytes and subluxation. [3, 4]
The knee joint is made up of three compartments, the medial and lateral tibiofemoral, in addition to the patellofemoral; all of them are not affected symmetrically. Unicompartmental knee osteoarthritis, mostly affects the medial tibiofemoral compartment, then the patellofemoral and finally the lateral one with the lowest incidence of all. Valgus deviation is defined as one that exceeds 7 to 10 degrees. [5, 6, 7]
Treatment of patients with lateral gonarthrosis ranges from conservative to surgical modalities, the latter differentiated between those that preserve the joint and others that do not, such as partial or total arthroplasties, each modality with very specific indications. [8, 9, 10]
The aims of this investigation are too updated on the most important features of lateral knee osteoarthritis and look for updated bibliography on the subject.
An extensive literature search in various data bases such as: PubMed [https://pubmed.ncbi.nlm.nih.gov/], Hinari [https://www.who.int/hinari/es/], SciELo [https://scielo.org/es/] and Medline [https://medlineplus.gov] was carried out with search term including ' lateral knee osteoarthritis', 'valgus knee osteoarthritis', and 'valgus knee deformity' from August 1st 2021 to September 30th 2021. Out of 312 articles, 44 selected citations were used in this review, being 42 of the last five years.
Our inclusion criteria included all the investigations in patients with lateral knee osteoarthritis. Articles related to complications derived from arthroplasty and those carried out in immature skeletons were excluded.
3. Etiology
Lateral knee osteoarthritis may be primary or secondary, within the latter, the post-traumatic gonarthrosis is due to previous fractures of the tibial plateau and postoperative procedures such as meniscectomies. Lateral tibial plateau is more convex than medial that is why meniscectomy increases significantly the contact between the joint surfaces and favors the development of degenerative changes in the joint. [11, 12]
4. Pertinent physical examination and imaging
Patients with lateral knee osteoarthritis usually seek medical assistance complaining of moderate to severe pain and valgus deformity; both have been increased in recent months accompanied by gait claudication. On physical examination, the valgus deformity is detected by inspection; a simple and effective method of detecting angulation is by measuring the Q angle, from the anterior superior iliac spine to the center of the patella and from there to the anterior tibial tuberosity (Figure 1). [13, 14]

On palpation, joint line pain or well-localized pain, crepitus, effusion, locking and catching can be detected. Stability maneuvers show laxity of the medial ligaments and shortening of the lateral ones, these are essential elements to be taken into account for treatment. [14, 15]
Radiography is of great help for the diagnosis, but it is important to remember that osteoarthritis is an entity in which the clinical and imaging features are not linear and symmetrical, hence there may be patients with marked degenerative changes on radiographs and have few symptoms or vice versa. On plain radiographs Fujisawa point should be calculated to determinate osteotomy and evaluate limb alignment after surgical procedures. [16, 17, 18]
Although the most widely used imaging tests are plain radiographies in posteroanterior and lateral weight-bearing projections with 30 degrees of knee flexion Rosenberg view), magnetic resonance imaging also provides highly helpful features, especially those related to the condition status of the menisci, thickness and contour of the articular cartilage in addition to the state of the rest of the compartments within the joint. [20, 21]
Computerized axial tomography has very specific indications in patients with lateral knee osteoarthritis and its use is reserved for evaluating bone anatomy in surgical planning. [22, 23]
Treatment methods for patients with lateral knee osteoarthritis are similar to those of the rest of the compartments; however patients tolerate nonoperative treatment better than those with medial compartment involvement. [24, 25]
5. Treatment
5.1 Nonoperative treatment
Nonoperative treatment is the most used modality and includes non-steroidal anti-inflammatory analgesics, viscosupplementation, and intra-articular steroids. Others non-pharmacological treatment options such as braces or orthoses, modifications of footwear and physical activity, body weight lost, use of crutches or canes and physical therapy and rehabilitation also may be helpful. Pain relief from the use of orthoses suggests a good future response to corrective osteotomies and unicompartmental arthroplasties. [26, 27]
5.2 Surgical treatment
Surgical procedures for patients with lateral knee osteoarthritis and valgus deformity are osteotomies, and unicompartmental or total arthroplasty. The first modality respects the patient's joint and manages to correct the deformity. [28, 29]
Corrective osteotomies in patients with lateral knee osteoarthritis aim to reduce the weight load in the affected compartment. General indications for osteotomy include age (younger than 65 years), patients with degrees I and II of Ahlback classification of lateral compartment, slight laxity of the ligaments, and a good range of motion of at least 90 degrees of knee flexion. [30, 31]
Contraindications for femoral osteotomies are: the presence of osteoarthritis of the medial or tricompartmental compartment, symptoms related to the medial compartment of the joint due to inflammatory arthritis, flexion contracture greater than 15 degrees, knee flexion less than 90 degrees and severe osteoporosis. [32, 33]
Distal femoral osteotomies may be medial closed and lateral open, both with the purpose of aligning the limb and achieving a horizontal joint line placement. The differences between these two procedures can be seen in Table 1. [28, 31]

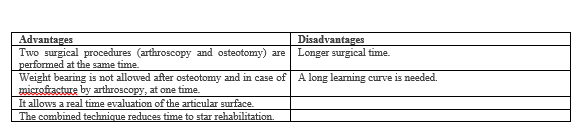
Arthroscopy can be performed in conjunction with osteotomy and is justified in patients with the presence of symptoms and mechanical joint signs due to involvement of the menisci and the possibility of loose bodies. Arthroscopy allows the performance of meniscectomies, synovectomy, and removal of loose bodies and grading of the cartilage condition in each of the compartments. [2, 34]
Advantages and disadvantages of arthroscopy and osteotomy at the same tome are summarized in the table 2. [35, 36]
Complications related to of osteotomy in patients with lateral knee osteoarthritis are few, the most common complication is joint stiffness, and its incidence is reduced by avoiding the joint during surgery. Nonunion is the second most common complication with an incidence of 4.2 to 19% and is associated with failure of the osteosynthesis material, especially when it is placed on the medial side. [32, 33]
Lateral unicompartmental arthroplasty represents from 10 to 23% of all partial arthroplasties, it is a surgical treatment modality that preserves part of the joint; the main indications for this treatment are isolated involvement of the lateral compartment with a 90-degree joint range of motion. The advantages of this technique lie in the low loss of blood during the operation and a low rate of complications. [37, 38]
The results of medial and lateral partial arthroplasty are similar. Partial arthroplasty is contraindicated in patients with involvement of other compartments of the knee, presence of instability, inflammatory arthritis, and fixed valgus deformity. In these situations, total joint arthroplasty is more advisable. [39, 40]
Lateral knee osteoarthritis usually appears later in life, hence total knee replacement is a very good option in these patients. The main indication for total knee arthroplasty is tricompartmental joint disease associated with limited response to pain despite nonoperative treatment and other surgical treatment modalities. [41, 42]
Krackow KA classification cited by Greenberg A et al. is useful during the performance of total knee arthroplasty in patients with valgus deformity and is divided into three grades (Table 3).

Valgus contracture causes contracture of the lateral structures, hence the need for extensive releases to achieve alignment and balance of the ligaments, and for this reason patellofemoral instability and peroneal nerve injuries can occur. [42, 43]
At present, robotic and navigational surgery significantly improve the short-term and long-term results of all the surgical modalities described above. [44]
Lateral knee osteoarthritis is the least common of the unicompartmental osteoarthritis that affect the knee joint. The clinical and imaging diagnosis provides the essential features for both nonoperative and surgical modalities, the latter modality includes techniques that preserve the joint such as osteotomies associated to arthroscopy and others that do not, among which arthroplasties stand out.
Declaration of competing interest
Nil grants/funding
The author declares no conflict of interest.
The material has not been previously presented.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
