
Case Report | DOI: https://doi.org/10.31579/2690-1897/127
1 Oman Medical Specialty Board, OMAN.
2 Oncoplastic Breast Surgeon, Royal Hospital muscat, OMAN.
*Corresponding Author: Sawab Al Hosni, Oman Medical Specialty Board, OMAN.
Citation: Sawab Al Hosni, Ibrahim Al Waili. (2022). Lateral Intercostal Artery Perforator Flap for Breast Cancer: A Case Report from Oman. Journal of Surgical Case Reports and Images, 5(5); DOI: 10.31579/2690-1897/127
Copyright: © 2022, Sawab Al Hosni, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 September 2022 | Accepted: 29 September 2022 | Published: 16 November 2022
Keywords: breast cancer; intra-op ultrasound; lateral intercostal artery perforator flap
Breast cancer is the commonest cancer in females. Historically, breast cancer surgery (BCS) was not considered a safe option, until 20 years back when those concerns were dismissed by the introduction of several surgical techniques. Today, women living in countries with fairly advanced healthcare systems, have the option of getting surgical treatment that is both safe and aesthetically pleasing. One of the promising surgeries being discussed in literature and is not widely practiced worldwide is the Lateral Intercostal Artery Perforator Flap (LICAP) flap.
We present a case of a 52 y/o lady who self-presented to the Breast Surgery Outpatient Department (OPD) after she noticed a mass on her left breast. The patient was willing for BCS as she was particularly concerned about cosmesis. LICAP flap surgery was performed and the results were remarkable. LICAP flap is a surgical technique that, despite it requiring sharp surgical skills, continues to be a promising addition to the BCS options for women with breast cancer. With good planning and using intra-op ultrasound it can be the preferred choice for many patients.
Breast cancer is the commonest occurring cancer in females around the world, accounting for about 12% of women. The incidence has been increasing due to the aging population, however, 5-year survival rates have also increased as tumors are being detected earlier and better treatments are being provided [1]. Historically, mastectomies have been the mainstay of treatment for breast cancer as first introduced by William Stewart Halsted (1852-1922) who, later on, was strongly against breast reconstruction and whose opinions have greatly influenced the controversy for several decades mainly for his oncological concerns [2, 3]. In the past twenty years or so, breast conserving surgery started becoming an acceptable option for women with breast caner, and today, different options and techniques have been studied and are available for almost every woman in a country with an advanced healthcare system [2].
Evolution of breast reconstruction surgery
Czerny (1895) was the first surgeon to ever introduce the idea of replacing excised breast tissue with a lipoma. Not long after that, Legueu (1898) and Morestin (1903) attempted to reconstruct the breast after mastectomy by using tissue from the contralateral breast, creating a large unattractive “breast” in the centre of the chest, which was abandoned for oncological concerns and poor cosmesis. Ombredanne (1906) introduced using the pectoralis minor muscle to replace the breast tissue and covering it with a rotating thoracoabdominal skin flap. In that same year, Tansini created a latissmus dorsi (LD) flap which was not used until 70 years following his design, when Olivari re-introduced it with the addition of an implant. Implants were first created by Cronin in 1963, which marked an important phase to the evolution of reconstructive surgery of the breast [2]. From the early 1970s up to the early 1990s, standard surgical treatment for breast conserving surgery (BCS) was first by using the latissmus dorsi myocutaneous flap, followed by the introduction of several techniques including the transversus rectus abdominis myocutaneous (TRAM) flap and the deep inferior epigastric perforator (DIEP) flap along with gluteal and thigh flaps [2,3].
In recent years, Hamdi et al established several highly versatile BCS flaps including the lateral intercostal artery perforator (LICAP) flap [4]. This technique, however, is not frequently used in current practice as it required a tedious microsurgical perforator dissection and perhaps, possible conversion to an LD flap [5].
Anatomy
Often the is skin is redundant in the area of the upper back. This makes the lateral chest wall, adjacent to the inframmary fold, a possible area to harvest skin and fat from for reconstruction, which is basically, the concept of the LICAP flap. According to cadaver dissection in one study, within 6-8cm from the mis-axillary line, there are 2-5 lateral intercostal artery perforators. This characterizes the flap pedicle that can be rotated 180 degrees. Furthermore, one perforator bundle that is more than 5mm in diameter is enough to supply the rotated flap [5].
A 52 y/o married lady, with 6 children, and a background history of ulcerative colitis controlled with medical management, no previous surgical history, self-presented to the Breast Surgery OPD on 19/11/2020 after she noticed a left breast mass 4 months prior to presentation. She did not notice an increase in the size, nor did she notice any nipple changes or discharge.
She has no family history of breast or other cancers, no personal history of smoking or using contraceptive pills and no history of weight loss.
Physical examination
On examination, the patient was haemodynamically normal, local examination of the breasts revealed small breasts of A cup size. There was no obvious asymmetry but skin tethering was noticed on the left breast laterally. There was no nipple retraction or discharge and no skin changes like ulceration, erythema or peu d’orange. On palpation, a small firm lump was felt on the left breast at 3 o’clock measuring about 2x2cm, occupying about a quarter of the breast. Axillary lymph nodes were also palpable on that side. The contralateral breast looked normal and did not reveal any lumps on palpation and there were no palpable axillary lymph nodes.
A Tru-cut biopsy was taken.
Examination
a) Mammogram
A subtle hyperdense focus is noted in the left breast upper outer quadrant. A 1.4x0.7x1.3 cm irregular speculated lesion is noted in the left breast at the 3 o’clock location (figure 1).
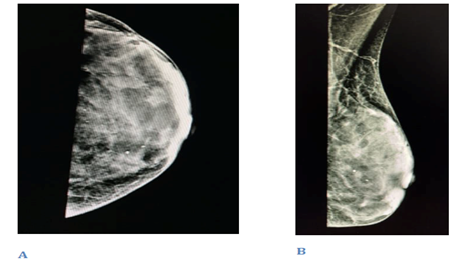
Figure 1: mammogram, A. cranio-caudal view, B. mediolateral oblique view
b) US
The ultrasound report showed an ill-defined hypoechoic mass with irregular margins measuring 2.3x1.4cm, BIRADS 5 (figure 2).
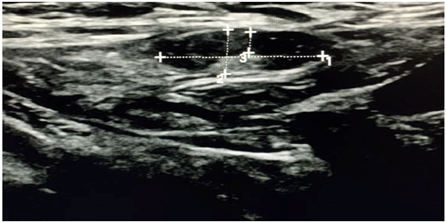
Figure 2: Ultrasound image of left breast lesion
c) CT chest, abdomen, pelvis:
As part of staging, the patient had a CT chest, abdomen and pelvis which showed no evidence of metastatic disease.
d) Histopathology
The histopathology report from the left breast mass biopsy showed invasive ductal carcinoma, Nottingham grade III. There was lymphovascular invasion and the hormone receptors that were positive were ER and PR. The Her-2 receptor came back as negative.
Surgery
The patient was taken for a left breast conserving surgery (wide local excision [WLE] + LICAP + sentinel lymph node biopsy). Pre-operatively, marking was done around the tumor, and the LICAP vessels were marked with the use of a hand-held ultrasound Doppler. Methylene blue was injected in the peri-areolar area and massaging was done for about 10 minutes. Then the left axilla was opened and blue-stained lymph nodes were identified and sent for frozen section, which eventually were reported as negative for metastasis hence no further nodes were dissected. A standard WLE elliptical incision was made over the tumor. Upper and lower flaps were raised and a formal WLE was done down to the pectoralis major muscle. The specimen was oriented with a short superior and a long lateral suture. For the LICAP reconstruction, an elliptical incision was made over the area that was identified and marked using the Doppler ultrasound. The flap was raised and rotated safeguarding the blood supply and venous drainage. The flap was then brought forward and rotated into the WLE space. Skin de-epithelialisation was done with good bleeding from the flap and it was fixed using 3-0 Vicryl. Wash done and haemostasis was secured. LICAP clips were inserted to the WLE cavity for future radiotherapy. The wound was closed in layers using 3-0 Vicryl and the skin was closed with monocryl 3-0 subcutaneously. No drain was inserted (figure 3).
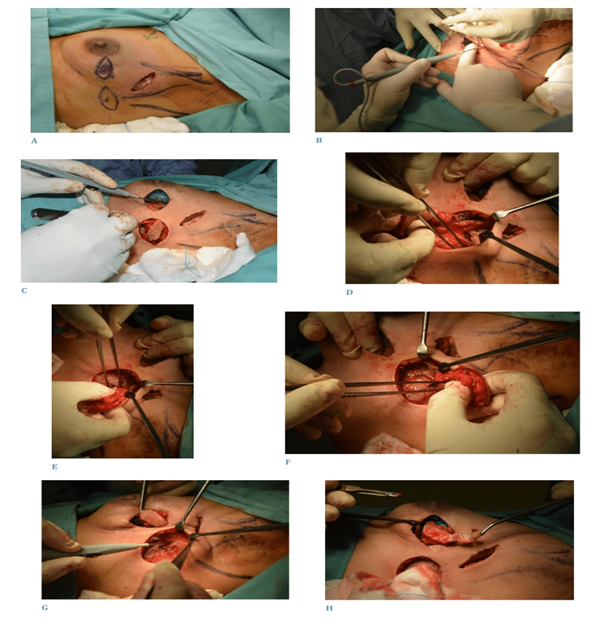
Figure 3: surgery steps. A. marking of flap and slnb, B. elliptical skin incision to create the flap, C. flap created, D - G. rotation of the flap, H. skin de-epithelialisation, I & J, skin closure.
The patient in this study was followed up on 5 days (figure 4), 6 weeks and 12 months post-op with excellent outcomes and great patient satisfaction.

Figure 4: Post-operative day 5. I. Anterior view, J. Lateral view.
One of the difficulties in creating a lateral artery perforator flap lies in the fact the perforator does not supply a wide area, hence, the flap might not be large enough to cover the excised tissue [6]. However, this surgical technique may be favourable to patients as not only does it provide good aesthetic outcomes, but it requires a shorter hospital stay and there is no muscle sacrifice in the procedure. An advantage to the surgeon would be that the viability of the flap, ie the vascularity, can be assessed immediately after rotating it [5].
Currently, lateral intercostal perforator flaps are not widely practiced as compared to other commoner breast reconstruction surgeries, due to technical difficulties in creating a flap with a limited range of movement along with the difficulty in the surgical technique itself. Introducing it to current surgical practice is a further development in the evolution of breast reconstruction surgery and a great addition to the options available for patients in order to provide them with aesthetically-pleasing results which is the sine qua non of breast reconstruction surgery.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
