
Research Article | DOI: https://doi.org/10.31579/2578-8965/216
Federal State Budgetary Educational Institution of Higher Education Novgorod State University named after Yaroslav the Wise
*Corresponding Author: Cruz García Lirios, Federal State Budgetary Educational Institution of Higher Education Novgorod State University named after Yaroslav the Wise.
Citation: Molina González MDR, Cruz G. Lirios, Gaxiola Sánchez MT, Camargo Pacheco MDJ, Rafael C. Mendoza, (2024), Latent learning curve of intellectual capital formation in a public university in central Mexico in the face of the pandemic, J. Obstetrics Gynecology and Reproductive Sciences, 8(2) DOI:10.31579/2578-8965/216
Copyright: © 2024, Cruz García Lirios. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 February 2024 | Accepted: 22 February 2024 | Published: 04 March 2024
Keywords: covid-19; stigma; knowledge management; knowledge network; risk
The latent growth curve is a technique of structural equations which propose that psychological and social phenomena can be modeled in relationships between factors and indicators. The objective of this work was to establish the differences that reflect the learning of the use of anti-pandemic devices. A longitudinal study was carried out from 2020 to 2024 in a sample of 100 students from a public university in central Mexico who were selected from high school to university. The results show that there are differences, but these are not significant. Such findings agree with studies related to stigma towards anti-pandemic policies. In relation to this state of the art, it is recommended to extend the study to the stigma derived from confinement and distancing in order to establish the learning curve of self-care and prevention. The implications of the study on treatment adherence suggest that stigma would be a latent factor that would be mediating the relationship between the intercept factor and the latent slope factor.
The history of epidemics has played a significant role in shaping the formation of intellectual capital— the collective knowledge, skills, and innovation within societies (Xu, Haris & Irfan, 2022). Throughout different periods, epidemics have spurred advancements in medicine, public health, and various fields (Vuong et al., 2022). Here is an overview of how some historical epidemics have influenced the development of intellectual capital:
The Black Death, a devastating pandemic of bubonic plague, swept through Europe in the 14th century (Papíková & Papík, 2022). Despite the immense loss of life, this epidemic had cultural repercussions (Kirchner, Ipsen & Hansen, 2021). The scarcity of labor resulting from the plague led to changes in labor relations, with increased wages for remaining workers (Wang & Wu, 2021). This shift contributed to a higher valuation of labor and knowledge, adding to societal intellectual capital.
The Spanish Flu pandemic had a profound impact on global society following World War I (Faisol, Astuti & Puji Winarko, 2021). Despite the tragic loss of lives, it brought about changes in medicine and public health (Ghasemi, Nejad & Aghaei, 2021). The response to the Spanish Flu contributed to the development of epidemiology as a scientific field (Velásquez & Lara, 2021). Improved disease surveillance emerged, laying the foundation for research and the study of future epidemics.
The HIV/AIDS epidemic led to significant advancements in medical research and the formation of intellectual capital in virology and epidemiology (Leon, 2021). The fight against HIV/AIDS also raised public awareness about health, human rights, and stigma, contributing to intellectual capital in broader areas beyond just medicine.
The Ebola outbreak in West Africa highlighted the need for a coordinated global response and prompted improvements in epidemic preparedness (Vătămănescu et al., 2023). International alliances were formed, and investments were made in research to understand and combat Ebola, contributing to intellectual capital in virology, public health, and crisis management.
The COVID-19 pandemic has had a profound impact on the formation of intellectual capital worldwide (Guillen, 2021). The response to the pandemic has accelerated medical research, scientific collaboration, and the adoption of information technologies in healthcare (Saide & Sheng, 2021). It has also underscored the importance of public health and the need for a coordinated global response.
Epidemics throughout history have driven advancements in knowledge, medicine, and societal structures (Alnatsheh, Karaatmaca & Çavuşoğlu, 2023). The challenges posed by these events have often catalyzed the formation of intellectual capital as societies adapt, learn, and innovate in the face of public health crises (Deliu, 2020). The intellectual capital developed during these times continues to shape our understanding and responses to current and future challenges.
The relationship between COVID-19 and the formation of intellectual capital is intricate and involves both challenges and opportunities (Alnassafi, 2022). Intellectual capital encompasses the intangible assets of an organization, such as knowledge, skills, innovation, and culture (Schleper et al., 2021). The impact of the pandemic on the formation of intellectual capital can be examined in several ways: The shift to remote work, driven by the pandemic, has highlighted the importance of virtual collaboration tools and digital platforms ((Bratianu & Bejinaru, 2021). Organizations have had to enhance their intellectual capital in terms of technology adoption, virtual communication skills, and collaboration methods (Karakose et al., 2021). The disruptions caused by COVID-19 have emphasized the need for continuous learning and upskilling (Jalal et al., 2021). Organizations that invest in the intellectual capital of their employees through training programs and professional development initiatives can adapt more effectively to changing circumstances.
The pandemic has created a dynamic and uncertain business environment, requiring organizations to innovate and adapt quickly (Jaradat et al., 2023). Intellectual capital is formed and strengthened when organizations encourage a culture of innovation, allowing employees to contribute ideas and solutions to address challenges (Sotomayor-Castillo et al., 2021). Building intellectual capital involves not only acquiring new knowledge but also managing and preserving existing knowledge within the organization (Mahdi & Nassar, 2021). The pandemic has underscored the importance of resilience and effective knowledge management strategies to mitigate risks and uncertainties (Gombos et al., 2021). While the pandemic has posed challenges, it has also created opportunities for entrepreneurial ventures. Organizations that can identify and capitalize on these opportunities contribute to the formation of intellectual capital by fostering a culture of entrepreneurship and strategic thinking.
The accelerated pace of digital transformation during the pandemic has led to the formation of intellectual capital related to technology adoption, data analytics, and digital strategies (Mubarik et al., 2022). Organizations that embrace digital tools and processes are likely to strengthen their intellectual capital in these areas. Intellectual capital is not limited to technical skills but also includes social capital—the relationships and networks within an organization (Putrino et al., 2020). The pandemic has prompted organizations to prioritize employee well-being, contributing to the formation of intellectual capital in terms of a positive and supportive workplace culture.
Organizations have had to reevaluate and strengthen their supply chains in response to disruptions caused by the pandemic (Xu, Haris & Irfan, 2023). The formation of intellectual capital in supply chain management involves developing strategies for resilience, risk mitigation, and agility (Landolo et al., 2021). The relationship between COVID-19 and the formation of intellectual capital is characterized by the challenges posed by the pandemic, as well as the opportunities for organizations to enhance their knowledge, skills, and innovation capabilities (Aleanizy & Alqahtani, 2021). Proactive management of intellectual capital is crucial for organizations seeking to navigate the complexities of the current business landscape and position themselves for future success.
While there may not be a specific theory explicitly named "the theory of the formation of health intellectual capital," we can draw upon existing theories and concepts to understand how intellectual capital is developed within the health sector (Augustinah et al., 2022). Intellectual capital in health involves the accumulation of knowledge, skills, and innovation that contributes to advancements in healthcare, medical research, and public health. Here are several theories and concepts that provide insights into the formation of health intellectual capital:
The Knowledge-Based View emphasizes the role of knowledge as a strategic resource for organizations (Pablos, 2023). In the health sector, organizations such as hospitals, research institutions, and public health agencies accumulate intellectual capital by fostering a culture of continuous learning, investing in research and development, and promoting knowledge sharing among professionals.
Human Capital Theory focuses on the value of individual knowledge, skills, and abilities. In the health sector, the theory suggests that investing in the education, training, and professional development of healthcare professionals contributes to the formation of intellectual capital (Schislyaeva et al., 2022). Well-trained and skilled healthcare workers enhance the overall capacity and effectiveness of the healthcare system.
The Innovation Theory highlights the importance of innovation in organizational success. In the health sector, intellectual capital is formed through innovative practices, technologies, and approaches to patient care, medical research, and public health interventions (Paoloni et al., 2022). Organizations that foster a culture of innovation contribute to the development of health intellectual capital.
Social Capital Theory emphasizes the value of social relationships and networks (Muftiasa, Wibowo & Rahayu, 2023). In the health sector, collaboration among healthcare professionals, researchers, and organizations contributes to the formation of intellectual capital. Strong social networks facilitate the exchange of knowledge, best practices, and collaborative efforts to address health challenges.
The Learning Organization Theory posits that organizations capable of continuous learning and adaptation are better positioned for success (Cristea & Dinu, 2022). In the health sector, organizations that embrace a learning culture, encourage feedback, and invest in training and development contribute to the formation of intellectual capital by staying abreast of medical advancements and evolving healthcare practices.
The Triple Helix Model describes the collaboration between government, industry, and academia to foster innovation (Al Momani et al., 2021). In the health sector, this model suggests that partnerships between public health agencies, healthcare providers, and research institutions contribute to the formation of intellectual capital by combining knowledge from various sources and driving innovation.
Health Systems Strengthening focuses on improving the six building blocks of health systems: leadership and governance, health information systems, health workforce, service delivery, medical products and technologies, and financing (Ashraf et al., 2023). Strengthening these components contributes to the development of intellectual capital in the health sector by enhancing the overall capacity and performance of healthcare systems.
The formation of health intellectual capital is a multifaceted process influenced by various theories and concepts (Florensia, Kohardinata & Laturette, 2022). It involves investments in education, research, innovation, collaboration, and continuous learning within the healthcare ecosystem. The integration of these elements contributes to the advancement of medical knowledge, the improvement of healthcare delivery, and the overall resilience of health systems.
The formation of intellectual capital in health is a multidimensional process that involves the accumulation, management, and utilization of knowledge, skills, and innovation within the healthcare sector (Campas et al., 2023). Several dimensions contribute to the formation of intellectual capital in health, each playing a crucial role in advancing medical knowledge, improving healthcare delivery, and addressing public health challenges. Here are key dimensions of the formation of intellectual capital in health:
The knowledge and skills of healthcare professionals are a vital component of intellectual capital (Agostini & Nosella, 2023). Investments in education, training, and professional development contribute to the formation of a highly skilled and knowledgeable healthcare workforce (Chi, 2021). The expertise and experience of healthcare professionals, including physicians, nurses, and allied health professionals, contribute to the intellectual capital in health. Clinical competence and specialized knowledge enhance patient care and outcomes. Investment in research institutions, laboratories, and medical facilities contributes to the structural capital in health. Ongoing research activities generate new knowledge, medical technologies, and treatment modalities, enhancing the intellectual capital of the healthcare sector. The development and utilization of robust health information systems contribute to the intellectual capital by facilitating data-driven decision-making, epidemiological research, and the efficient management of health information.
Collaboration among healthcare organizations, research institutions, and public health agencies fosters the exchange of knowledge and resources (Hariyono & Tjahjadi, 2021). Building strong relationships and partnerships contributes to the relational capital in health. Engaging with communities and stakeholders contributes to intellectual capital by addressing social determinants of health and promoting health equity. Community involvement enhances understanding and responsiveness to diverse health needs.
The integration of cutting-edge technologies, such as telemedicine, artificial intelligence, and digital health solutions, contributes to the intellectual capital in health (Haribowo, 2024). Technological innovation enhances healthcare delivery, diagnostics, and treatment options. Adoption of innovative practices and evidence-based approaches within healthcare organizations contributes to intellectual capital. Continuous improvement and the implementation of best practices enhance the overall quality of healthcare services.
A culture of continuous learning within healthcare organizations promotes ongoing professional development, adaptability to emerging challenges, and the incorporation of new knowledge into practice (Yang & Chen, 2023). Encouraging knowledge sharing and collaboration among healthcare professionals and departments within an organization enhances the intellectual capital by facilitating the exchange of ideas and expertise.
The development and implementation of effective health policies contribute to the intellectual capital by providing a framework for healthcare delivery, research priorities, and public health interventions (Amirullah, Dharma & Putri, 2021). Strong leadership and governance structures within healthcare organizations and at the national level contribute to intellectual capital by fostering a strategic vision, innovation, and effective decision-making.
A robust system for monitoring and surveillance of infectious diseases and public health trends enhances the intellectual capital by providing timely information for effective public health interventions (Pellegrini, Aloini & Latronico, 2023). Preparedness for health emergencies, including pandemics, contributes to the intellectual capital by ensuring a coordinated and effective response to unforeseen challenges.
The dimensions of the formation of intellectual capital in health are interconnected and contribute collectively to the advancement of healthcare knowledge, the improvement of patient outcomes, and the overall resilience of health systems (Carreon-Guillen & Garza-Sanchez, 2023). Organizations and systems that strategically address these dimensions are better positioned to navigate challenges, innovate, and contribute to the ongoing development of intellectual capital in health.
However, the formation of intellectual capital has not been established as permanent and continuous learning. The studies reviewed note an immediate learning curve, but do not account for its persistence over time. This is the case of stigma as a result of anti-pandemic policies and confinement and distancing strategies, as well as exposure to unverifiable information in the media and socio-digital networks.
Stigma theory can help us understand how social attitudes and perceptions influence the experiences of individuals or groups associated with a particular condition, in this case, COVID-19 (Bagcchi, 2020). Stigma refers to the negative beliefs, attitudes, and stereotypes that people may hold towards individuals or groups who are associated with a particular attribute, trait, or condition. Individuals who have contracted COVID-19 or are perceived to be at risk may face stigmatization. Terms like "COVID-positive" or "COVID-affected" can carry a stigma that leads to negative perceptions. Those associated with COVID-19 may be stereotyped as irresponsible, careless, or as a threat to public health. Stereotypes can lead to discrimination and marginalization.
Fear of infection may lead to prejudiced attitudes towards individuals with COVID-19, impacting their social interactions and relationships (Chopra & Arora, 2020). This can manifest as discrimination in various settings. Stigma can evoke strong emotional reactions, such as fear, anger, or anxiety, both from individuals with COVID-19 and from those in the community who fear contagion. Stigmatized individuals may experience power imbalances, feeling disempowered and marginalized. This can affect their ability to access resources, support, or fair treatment. Stigma may result in social exclusion, where individuals with COVID-19 are avoided or ostracized, leading to loneliness and a lack of social support. Stigma can be embedded in institutions and systems, affecting policies and practices related to employment, healthcare, and education for those associated with COVID-19.
Individuals facing stigma may develop coping mechanisms to navigate societal attitudes. Support systems and community awareness can play a crucial role in fostering resilience (Villa et al., 2020). Media coverage can contribute to stigmatization by framing COVID-19 in ways that reinforce negative stereotypes or create an atmosphere of fear. Education and awareness campaigns can help combat stigma by providing accurate information about COVID-19, emphasizing empathy, and promoting understanding. Understanding and addressing stigma related to COVID-19 is crucial for fostering a supportive and inclusive society. It requires collective efforts from individuals, communities, healthcare professionals, and policymakers to reduce stigma and discrimination associated with the pandemic. Education, empathy, and open communication are essential tools in combating COVID-19 stigma.
The objective of this work was to establish the latent learning curve around the formation of intellectual capital in the face of the pandemic.
Hypothesis. Given that the anti-covid policies were continuous and intensified according to the evolution of the pandemic, it impacted the formation of intellectual capital through learning to use anti-pandemic devices such as face masks and alcohol gel (Dai, 2020). Therefore, significant differences are expected between the intersection factor and the linear slope factor. Values close to unity can be considered as evidence of non-rejection of the hypothesis.
A longitudinal study was carried out with a sample of 100 students (M = 21.23 SD = 3.2 years and M = 9'978.34 SD = 546.45 monthly income) selected for their affiliation to public health institutions.
The COVID-19 prevention questionnaire was used, which includes personal information, symptoms of the disease, history of exposure and transfer, preventive measures, vaccination status, sanitary conditions and additional information, as well as a declaration and signature of acceptance of confidentiality. and anonymity (see annex).
Focus groups were organized for the homogeneity of the concepts. Participants were informed about the objectives and responsibilities of the project. Groups of 10 were organized to implement the informative workshop on the use of anti-COVID-19 devices. Self-reports were distributed after the workshop session.
The data were captured in Excel and processed in JASP version 17. The parameters of mean, variance, covariance, fit and residual were estimated in order to contrast the latent growth curve model. Values close to unity were assumed as evidence of non-rejection of the hypothesis except for the residual values.
The mean of the latent curve is significant for the intersection factor and the linearity factor (see Table 1). Both suggest significant differences between the beginning of the training process and the final measurement. Learning is inferred from the use of anti-pandemic devices, although an analysis of its determinants would indicate whether sex, age, education or income have an impact on the process.
| 95%% Confidence Interval | Std. Est. | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Component | Parameter | Estimate | Std. Error | z-value | p | Lower | Upper | LV | All | No X | ||||||||||||||||
| Intercept | Mean | 2.562 | 0.100 | 25.614 | < .001 | 2.366 | 2.758 | |||||||||||||||||||
| Variance | -0.055 | 0.176 | -0.310 | 0.756 | -0.400 | 0.290 | ||||||||||||||||||||
| Linear slope | Mean | -0.196 | 0.044 | -4.486 | < .001 | -0.282 | -0.111 | -0.757 | -0.757 | -0.757 | ||||||||||||||||
| Variance | 0.067 | 0.032 | 2.092 | 0.036 | 0.004 | 0.130 | 1.000 | 1.000 | 1.000 | |||||||||||||||||
Table 1: Latent curve
The mean of the latent curve is significant for the intersection factor and the linearity factor (see Table 2). Both suggest significant differences between the beginning of the training process and the final measurement. Learning is inferred from the use of anti-pandemic devices, although an analysis of its determinants would indicate whether sex, age, education or income have an impact on the process.
| Table 2. Residual variances | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 95%% Confidence Interval | Std. Est. | ||||||||||||||||||
| Variable | Estimate | Std. Error | z-value | p | Lower | Upper | LV | All | No X | ||||||||||
| 2020 | 2.044 | 0.309 | 6.611 | < .001 | 1.438 | 2.650 | 2.044 | 1.027 | 1.027 | ||||||||||
| 2021 | 2.023 | 0.285 | 7.088 | < .001 | 1.464 | 2.582 | 2.023 | 1.072 | 1.072 | ||||||||||
| 2022 | 1.005 | 0.151 | 6.676 | < .001 | 0.710 | 1.300 | 1.005 | 1.091 | 1.091 | ||||||||||
| 2023 | 1.174 | 0.183 | 6.433 | < .001 | 0.817 | 1.532 | 1.174 | 0.919 | 0.919 | ||||||||||
| 2024 | 0.625 | 0.191 | 3.270 | 0.001 | 0.250 | 0.999 | 0.625 | 0.595 | 0.595 | ||||||||||
Table 2: Residual variances
If the means of the factors and the variances of the residuals suggest differences at the beginning and end of the training process, then the relationships between the variances (covariances) should be close to unity, but rather they are negative or approach zero (see Table 3). Such results are interpreted as not so significant differences between the beginning and the end of the process. Consequently, learning about the use of anti-pandemic devices is not so different from the beginning and end of the pandemic in the sample surveyed.
| Table 3. Implied covariance matrix | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2020 | 2021 | 2022 | 2023 | 2024 | |||||
| 1.989 | |||||||||
| -0.129 | 1.887 | ||||||||
| -0.204 | -0.144 | 0.921 | |||||||
| -0.278 | -0.151 | -0.024 | 1.278 | ||||||
| -0.353 | -0.158 | 0.036 | 0.231 | 1.050 | |||||
Table 3: Implied covariance matrix
Like the covariances involved, the residual covariances also suggest not so significant differences between the beginning and the end of the use of anti-pandemic devices (see Table 4). In other words, the learning is not that significant.
| Table 4. Residual covariance matrix | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | 2021 | 2022 | 2023 | 2024 | ||||||||||
| 0.025 | ||||||||||||||
| -0.475 | -0.117 | |||||||||||||
| 0.233 | 0.327 | -0.086 | ||||||||||||
| -0.083 | 0.210 | -0.235 | 0.073 | |||||||||||
| 0.017 | 0.259 | -0.327 | 0.210 | 0.022 | ||||||||||
Table 4: Residual covariance matrix
In fact, the curves are greater than zero and reflect an increase in the latent growth of the use of anti-pandemic devices, but for the most part there are
decreases relative to 2021 (see Figure. 1). That is, the sample surveyed learned preventive use of anti-pandemic devices, but in subsequent years he unlearned those basic prevention measures.
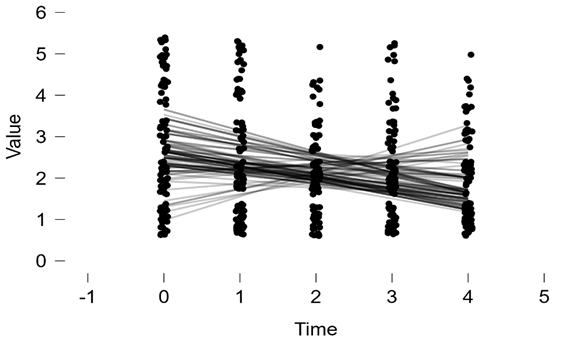
Figure 1: Curve Plot.
The fit and residual values ⌠
The contribution of this work to the state of the art lies in the contrast of a model that explains the latent growth curve around learning to use anti-pandemic devices. The results show a difference, but it is not significant because the covariance values are misleading or tend to approach zero. In this sense, the results of the present study adhere to the findings that report a transition from the use of anti-pandemic devices towards stigma and health recommendations (Bhanot et al., 2021). Prevention transformed into stigma is a growing phenomenon in confined samples (Turner-Musa, Ajayi & Kemp, 2020. The policies of confinement and distancing fostered stigma towards anti-pandemic recommendations (Ramaci, et al., 2020). In this way, the present work converges with studies on stigma towards anti-pandemic policies. Therefore, it is recommended to extend the study towards the impact of anti-pandemic policies with respect to learning preventive measures, including the use of anti-pandemic devices.
However, the limits of the study relative to sample size not only inhibit the generalization of the results to a population. Furthermore, the covariances indicate that the differences are minimal and as time progresses, there is an unlearning of preventive measures. Consequently, the study of stigma would explain a greater percentage of variance since 40% of it has been explained in the present study and could increase substantially.
The implications of the present study in the formation of intellectual capital are. 1) anti-pandemic policies asymmetrically impacted the preventive use of anti-pandemic devices. 2) Confinement and distancing foster a stigma towards anti-pandemic policies which is reflected in the learning and
unlearning of the use of anti-COVID devices. 3) Health promotion and self-care in the expertise of using anti-pandemic devices can be reversed. 4) The
training of talents with self-care can be distorted into a stigma towards health policies.
The objective of the present study was to demonstrate a latent growth curve around learning about COVID-19 prevention. The results suggest an unlearning of the use of anti-pandemic devices after a prolonged lockdown. Such findings suggest the study of stigma towards anti-health crisis policies, although the sample size limits the generalization of the results and the covariances indicate rather spurious differences. It is recommended to extend the study to the observation of stigma as a latent factor in the process of learning preventive measures.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
