
Case Report | DOI: https://doi.org/10.31579/2641-0419/126
Federal University of São Paulo – Brazil
*Corresponding Author: Miguel Maluf, Federal University of São Paulo - Brazil.
Citation: Miguel Maluf, (2021) Late follow-up of Persistent Truncus Arteriosus, after one-stage Repair, with Right Ventricular Remodeling. J. Clinical Cardiology and Cardiovascular Interventions, 4(5); Doi:10.31579/2641-0419/126
Copyright: © 2021 Miguel Maluf, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 January 2021 | Accepted: 13 March 2021 | Published: 24 March 2021
Keywords: right ventricle; remodeling; bicuspid; prosthesis; pulmonary valve
We report long-term outcome after one-stage, surgical repair, in a two months-old girl with persistent truncus arteriosus type I, II. The operation was carried out with the remodeling of the right ventricle, using a swine bicuspid pulmonary prosthesis. Twenty-six years later, the patient is in excellent clinical condition, CF I (NYHA), with normal peripheral oxygen saturation.
Recent invasive and not invasive imaging show: absence of intracardiac shunt and growing of the right ventricle outlet tract and discrete double lesion of the pulmonary valve. The pulmonary flow directed uniformly for both lungs. In selected cases, the long-term prognosis of patients with persistent truncus arteriosus, undergoing early surgical repair, avoiding the use of valved conduit, makes for an excellent evolution, without new interventions. Endovascular procedures, now well standardized, for the implantation of a pulmonary valve stent, through a catheter, will allow an effective approach, in the presence of late obstructions, in patients who have undergone right ventricular remodeling, without the use of valved conduits.
Persistent truncus arteriosus represents less than 3% of all congenital heart defects.
Rapid evolution of pulmonary hypertension and congestive heart failure, is the main reason for indication, for surgical correction, in the neonatal or lactating phase.
It is the main point of question, due to the type and diameter of prosthesis chosen.
The remodeling of continuity between the right ventricle and the pulmonary artery is usually carried out with the implantation of a synthetic or biological valved conduit, appropriate to the patient's weight and body surface. [1]
This model of prostheses, will require its early replacement, in growing patients, to avoid the mismatch and mineralization process, that occurs in practically all pediatric patients
The remodeling of the right ventricular outflow tract, eliminating the use of valved conduits, was described by the author2, using a monocuspid biological prosthesis. Despite the ingenious conception of this technique, there has been an increasing number of reoperations, due to stenosis of the prosthesis employed.
Our Group at the Federal University of São Paulo, has been using the right ventricular remodeling technique since 1990, using swine valve prostheses (bicuspid prosthesis). [3].
Case presentation
A 26-year-old woman, height: 1.66m, weight: 67 kg, BMI: 20.1, return to annual control of a late follow-up of surgical correction persistent truncus arteriosus, operated at 2 month – old.
Our preference, in the correction of persistent truncus arteriosus type I, II, is the right ventricular remodeling, since 1990, without the use of valved conduit.
In this 2-month-old patient, the principle of the technique described by the author [2].
The technique consists of the disconnection of the pulmonary artery from the ascending aorta and closure of the aortic wall, with biological patch, avoiding distortion of the truncal valve.
Right ventricular remodeling surgery, was performed, with direct anastomosis between the RV and PAs or through the interposition of the left auricle, in case this anastomosis is under tension, for the construction of the wall posterior part of the RV outflow tract.
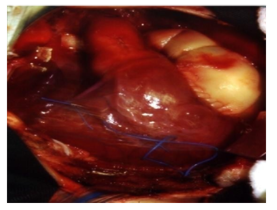
In the anterior phase of the right ventricular remodeling, a swine bicuspid prosthesis was used, to reconstruct a pulmonary neo valve. Figure 1.
The patient is in functional class I (NYHA), without restrictions to perform scheduled physical activity, by her personal trainer, such as daily aerobic exercises and 45 min runs, 3 times a week, with monitoring of cardiopulmonary parameters, being well tolerated by the patient. On physical examination, the patient has a good general condition and normal weight-bearing development, her percent SO2 = 96%.Cardiovascular system examination: Cardiac auscultation was performed during the clinical examination and observed the presence of rude, systolic and diastolic murmur in pulmonary focus. Following the postoperative control protocol, the patient underwent non-invasive and invasive imaging exams to assess hemodynamic and cardiopulmonary functional performance.
Investigations
Chest X-ray: 50% cardiothoracic index, enlargement of the upper mediastinum, with reference to elongation of the ascending area and rectification of the pulmonary silhouette; Lungs with normal parenchyma and circulation.
ECG: Sinus rhythm, HR: 75 b x min, QRS axis: 120°, right bundle branch block. Transesophageal echocardiogram: Systolic function and segmented, biventricular contractility. Pulmonary valve presents mild insufficiency, moderate stenosis, with a mean gradient of 36 mmHg, (maximum 76 mmHg) and pulmonary valve ring of 1.7 cm2 (1.2 cm2 at the pulmonary trunk-pulmonary artery junction). Competent, trivalvular aortic valve, with preserved morphology and mobility. Holter study: Sinus rhythm, without pauses, right bundle branch block, HR: 56 to 143 b x min. Ergospirometry test: Cardiopulmonary fitness, classified by oxygen consumption: VO2 = 25.0 ml x kg x min-1, was considered weak when compared to individuals of the same age and sex [4] and comparison of this with the anaerobic ventilatory threshold of 16.3 ml x kg x min-1, allow classifying the index as Class C [5]
The Ventilatory reserve (37% of MVV) was considered normal, not being a limitation on the quality of the effort made. Angio CT: Dilated right ventricle and moderate degree with pressure overload. Pulmonary prosthesis in the right ventricular outflow tract (proximal anastomosis, diameter 27.7mm). Signs of pulmonary valve calcification (diameter 23.3 mm) and slight restriction in the anastomosis at the origin of the pulmonary arteries (diameter 15.3 mm). RPA: 33 mm, LPA: 17.8 mm. Figure 2.

Figure 2. A- Angio TC imagen, (patient operated at 2 months of age). with a 26th follow-up to correct truncus arteriosus. B- Contrast image looking at 2 stenosis sites (arrows), in the prosthesis used in right ventricular remodeling.
Nuclear Magnetic Resonance: Left Ventricle with preserved contractility. Presence of anterior systolic movement of the anterior mitral valve leaflet, without obstruction in the left ventricular outflow tract.
Hypertrophic right ventricle with slight dilation and preserved contractility. Right ventricular outflow tract, with mild restrictive stenosis at the level of the prosthesis pulmonary valve and pulmonary artery – prosthesis anastomosis.
Cardiac catheterization: The hemodynamic study of the right cavities showed: RV: 55 x 2 mmHg, proximal AP: 35 x 12 and distal AP: 17 x 10 mmHg. RV - PA gradient: 20 to 38 mmHg, LV: 118 x 4 mmHg; Aorta: 120 x 75 mmHg.
The moderate stenosis in 2 locations of the outflow tract, were underwent to valvuloplasty with 25 mm balloon catheter, achieving a 50% reduction in the RV-PA gradient. Figure 3.
In persistent Truncus Arteriosus, pulmonary circulation is under the systemic pressure regime, due to the fact that pulmonary arteries originate from the ascending aorta and absent pulmonary valve.
The direct transmission of the systemic pressure to the lung, during ventricular systole, predisposes to early pulmonary hypertension. Reports made at the Mayo Clinic, document these findings, and confirm the need for indication of surgical correction in childhood.
Ebert et al [1], showed that there were technical conditions for surgical correction in the first 6 months of life, using d conduits, for right ventricular remodeling.
More recently, authors [6,7] reinforced the indication of correction of truncus arteriosus in the neonatal phase and demonstrated the technical conditions of repair in the neonatal period.
The first question refers to whether the technique used in surgical correction in the neonatal phase and childhood. The right ventricular remodeling, through the interposition of a valved conduit, between RV and PA, in neonates and childhood, will evolve, in a short period of follow up, with mismatch, requiring one or more reoperations, to replace the valved conduit, until reaching adulthood.
Our right ventricular remodeling technique, employing bicuspid swine prosthesis3, from 1990, always carried out on young infants, eliminating the need for valve conduits.
Our patient, after 26th years of follow-up, without any reoperation, imaging exams and hemodynamic evaluation showed growth of the pulmonary ring and right ventricular outflow We also have to highlight that the ventricular remodeling with the reconstruction of the pulmonary valve, allowed the preservation of the right ventricular function and the evolution of the patient in functional class I (NYHA), without restrictions for her physical activity, during the long follow-up.
Endovascular procedures, now well standardized, for the implantation of a pulmonary valve stent, through a catheter, will allow an effective approach, in the presence of late obstructions, in patients who have undergone right ventricular remodeling, without the use of valved conduits. tract, following the patient's body surface, however appearing mild stenosis, at the level of the bicuspid valve of the prosthesis and in the anastomosis of its, with Aps with a moderate RV - AP gradient. (Figure 3A) These 2 restriction sites were dilated employing balloon catheter, with success. (Figure 3B)

After the procedure, moderate residual pulmonary insufficiency will be the subject of clinical follow-up, scheduling the implantation by catheter of a pulmonary valve stent, in the near future.Figure 3. A- Angiographic image, of the right ventricular remodeling, observing 2 stenosis sites (arrows). B- Angiographic image, after dilation of the stenosis sites, with a balloon catheter (arrows).
The patient is in Functional Class I (NYHA), with no limitations for moderate daily aerobic exercise and 45 min runs, three times a week, with cardiopulmonary monitoring.
As it is an uncommon heart disease, there are few publications on late follow-up of surgical correction of Truncus Arteriosus, but the number of reoperations that patients had to undergo to replace valved conduits, is noteworthy in all publications, due to mismatch.
Similar published that his study [8], aims to analyze long-term results after correction of persistent truncus arteriosus in all patients operated in one institution over 28 years. Between 1981 and 2009, 83 patients, median age 54 days, underwent repair of truncus arteriosus. Twenty-five (30%) patients are alive with their original conduit 7.5 ± 5.2 years after correction. Twenty- eight patients required 41 re-operations for conduit dysfunction with first replacement at mean 5.8 ± 4.1 (range 0.1–14.1 years) years after correction. Nine (11%) patients required 12 truncal valve replacements. Eleven (13%) patients required balloon dilatation or stent for conduit obstruction, pulmonary branch stenosis.
Other published [9] with 36 children, underwent repair of persistent truncus arteriosus, in the period from January 2011 to December 2018, in two institutions. Surgical re-intervention was required in 8 patients (22.86%), and 11 patients (30.56%) had catheter-based reintervention.
Freedom from reintervention was 86% at 1 year, 75% at 2 years and 65% at 3 years. Survival at 1 year was 81% and at 3 years was 76%.
A new right ventricular remodeling technique, in the persistent truncus arteriosus, without the use of valved conduit, was published10, performed the anteriorization of the APs, in front of the ascending aorta, using the Lecompte maneuver [11], to construct the connection RV-PAs.
A cylindrical segment incorporating both pulmonary artery branches was sleeve-resected from the truncal artery. The cylindrical segment was cut in the middle and two truncal arterial flaps, were combined to form the posterior floor of the new pulmonary arterial trunk. The edge of the floor was attached directly to the superior margin of an oblique incision made in the left-anterior wall of the right ventricle.
A polytetrafluoroethylene (PTFE) monocuspid was attached to the lower half margin of the right ventricular incision. A large glutaraldehyde-treated pericardial patch was used to form the anterior hood of the new right ventricular outflow tract.
During follow-up (36-60 months, median 54 months), only one reoperation was necessary to widen a pulmonary artery stenosis of the left branch. Follow-up echocardiography showed pulmonary regurgitation (mild two, moderate seven, and severe one) and slight acceleration of flow in the left pulmonary artery branch and right ventricle-pulmonary artery connection in one case.
We consider that the late follow up of our patient (26 years), without reoperations, to replace the pulmonary prosthesis, evolving in Functional Class I (NYHA), without restrictions on physical activities, is the result of the technique employed and the implanted of swine bicuspid prosthesis, (in place of monocuspid), avoiding mismatch during patient development.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
