
Case Report | DOI: https://doi.org/10.31579/2641-0419/263
1,2 Shahid Gangalal National Heart Centre, Bansbari, Kathmandu, Nepal.
1,2 Department of Cardiac Surgery.
*Corresponding Author: Marisha Aryal, Shahid Gangalal National Heart Centre, Bansbari, Kathmandu, Nepal.
Citation: Marisha Aryal, Rabindra Timala (2022). Late Aortic Insufficiency After Ventricular Device Closure: A Case Report. J. Clinical Cardiology and Cardiovascular Interventions, 5(6); DOI:10.31579/2641-0419/263
Copyright: © 2022 Marisha Aryal, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 April 2022 | Accepted: 06 May 2022 | Published: 13 May 2022
Keywords: ventricular septal defect; device closure; aortic insufficiency; aortic regurgitation; amplatzer device occlude; case report
Device closure of isolated ventricular septal defect is taking precedence over surgical closure in current era. However, device closure in perimembranous and subarterial VSD is complicated by procedural acute aortic regurgitation. In this report we found late aortic regurgitation after four years of device closure of ventricular septal defect. This incident needs one to reconsider the choice of device in patients with perimembranous or subarterial ventricular septal defect as the rim of the occluder device is near the aortic cusp. Early intervention after the development of significant aortic regurgitation is beneficial for the patient.
Ventricular septal defect is the commonest congenital anomaly requiring surgical intervention. As transcatheter interventions have been advanced, device closure is used for most isolated VSDs. Immediate post-procedural complications of device closure include aortic regurgitation, right bundle branch block, residual shunt and device emboli. [1,2] Late onset of aortic regurgitation has been mentioned in literature and this mandates finding patients who are at risk of developing it.[3] This case report is of a patient who developed late aortic regurgitation due to perforation of the right coronary cusp following VSD device closure. High index of suspicion for aortic valve injury is necessary for patients with device closure developing late aortic regurgitation. This also mandates analyzing and deferring patients who are at risk. [4]
Ethical Statement
Patient’s guardian had been informed about the nature of study. Informed written consent has been obtained for the publication of the case. Approval of the Institutional review board has been obtained.
A twelve-year-old boy was referred to surgical outpatient clinic after noticing new aortic regurgitation (AR) of moderate severity in a follow-up transthoracic echocardiogram after VSD device closure. Patient had undergone VSD device closure 4 years back with amplatzer duct occluder (10/8mm). There was no AR in the previous follow-op echocardiography. Suspecting the device to be the culprit for the new onset significant aortic regurgitation patient was admitted for surgical retrieval of the device with VSD patch closure and repair/replacement of aortic valve.
Pre-operative transthoracic echocardiogram showed VSD device in-situ with no residual leak with moderate aortic regurgitation with any impingement of the aortic cusps.
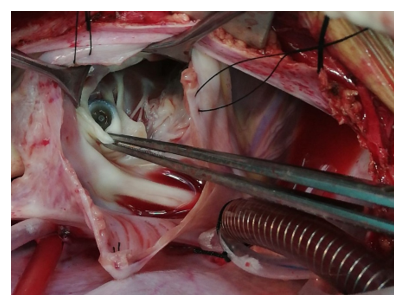
After standard anesthesia and lines placement, transesophageal echocardiography (TEE) was done. The findings were similar to the pre-operative echo. After establishing cardiopulmonary bypass and cardioplegic arrest, right atriotomy was done. Device was in-situ. (Figure 1) Oblique aortotomy was done. There was a 4x4 mm perforation in the right coronary cusp (RCC). (Figure 2)
VSD device was carefully extracted through right atrial approach. The ventricular septal defect was closed with PTFE patch. The perforation in the RCC was patched with pericardium. After weaning off bypass, there was no aortic regurgitation in TEE. Postoperative hospital stay was uneventful. Three months follow-up showed no aortic regurgitation in transthoracic echocardiography.

Isolated congenital ventricular septal defect can be treated either surgically or by percutaneous transcatheter approach. As studies have
shown low mortality and morbidity with the percutaneous approach, device closure of VSDs has been gaining more attention. [4,5] With the availability of different devices, the range of closure had been expanded from muscular to perimembranous and subarterial VSDs. Among various complications associated with device closure, aortic regurgitation is
considered to be rare. [6] Though retrospective studies comment on procedural AR leading to abandonment of the procedure, data regarding late AR development is scarce. [1] In this study, the patient had developed aortic regurgitation of moderate severity 4 years after the device implantation with only mild AR in prior annual follow-up. This late development of AR due to perforation of right coronary cusp (RCC) is unusual. There are reports of involvement of RCC after device closure either diagnosed incidently for management of hematuria or IE. [3,7] In patients with perimembranous VSD, subaortic rim is short or deficient. This increases the risk of immediate aortic insufficiency after device placement. Late aortic regurgitation should prompt the physician to rule out cusp-related etiology to plan for early intervention.
Early management of aortic regurgitation should be done to prevent the detrimental effect of volume overload in left ventricle. This also decreases the possibility of replacement of aortic valve, when repair can be done at early stage [7].
Timely intervention on this child saved him from further damage to the aortic valve cusps, which might have resulted in aortic valve replacement otherwise.
Device closure of VSD has negated the complications related to cardiopulmonary bypass. However, the short distance between the VSD device in perimembranous position and right coronary cusp might increase the risk of aortic regurgitation due to cusp injury. A study involving the size of the perimembranous VSD, choice of device and its outcome in terms of aortic regurgitation would be beneficial for proper patient selection. Once the device is inserted, patient should be closely monitored and intervened if needed.
The patient’s guardian and Institutional Review Committee have granted consent for publication of this case report.
none declared.
The authors received no financial support for the research, authorship, and/or publication of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
