
Case Report | DOI: https://doi.org/10.31579/2768-2757/175
1Adiyaman University School of Medicine, Department of Cardiovascular Surgery, Adiyaman, Turkey.
2Adıyaman University Faculty of Medicine Department of Cardiovascular Surgery.
*Corresponding Author: Cengiz Güven., Adiyaman University School of Medicine, Department of Cardiovascular Surgery, Adiyaman, Turkey.
Citation: Abuzer D. Sürücü, Cengiz Güven, (2025), Large Artery Thrombosis in a possible Covid-19 Patient; is Surgical Treatment always Necessary? Journal of Clinical Surgery and Research, 6(5); DOI:10.31579/2768-2757/175
Copyright: © 2025, Cengiz Güven. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 May 2025 | Accepted: 23 May 2025 | Published: 10 June 2025
Keywords: arterial thrombosis; brachiocephalic artery thrombosis; possible covid-19; medical treatment
Increased thromboembolic complications are common in COVID-19 with various mechanisms. Most thromboembolic events manifest as venous and pulmonary embolisms. Arterial embolism, which manifests itself with different additional complications, is rare. Although we have referred to it as a suspected Covid-19 case, our primary objective was to draw attention to our treatment approach for large artery thromboses, regardless of the cause, and to the human body's capacity for self-repair. The tendency of surgeons today to resort to surgical options for such cases without considering the severity of complications can sometimes lead to serious sequelae. In this case report, our treatment approach is discussed for Brachiocephalic Artery Thrombosis in a possible COVID-19 patient accompanied by the literature data.
Brachiocephalic Artery Thrombosis (BCAT) is a rarely described condition in the literature and usually requires emergency surgery, after presenting to the hospital with symptoms of right upper extremity and/or cerebral ischemia1. COVID-19 infection might progress with coagulopathy, the major organ involved being the lung. Frequent venous thromboembolic events, and rarely, arterial thrombosis have been reported.2 However, isolated BCAT has not been defined. Contrast-Enhanced Thorax and Upper-Right Extremity CT Angiography performed on the patient who applied to our hospital emergency department with complaints of pain in the 4th fingers of the right hand revealed mural thrombus at the brachiocephalic artery exit. The patient was accepted as a possible COVID-19 patient based on laboratory test results and Thorax CT findings. Our treatment approach in this case was discussed in light of the literature data. The patient agreed to have all laboratory data and images published.
A 49-year-old female patient applied to our hospital’s emergency department with a complaint of circulatory disorder in the distal part of the right 4th finger and stated that this complaint started 3 weeks ago and she had pain from time to time. The patient, who had no history of any traumas, had a serious lower respiratory tract infection approximately one month ago and was hospitalized for 3 days with a diagnosis of pneumonia. Laboratory tests revealed D-Dimer 5248 mcg/liter, CRP 3.76 mg/dL, fibrinogen value 457 mg/dL, interleukin-6 value 6587 pg/mL, and ferritin value 1496 ng/ml. Contrast CT scans of the thorax and right upper extremity were performed on the patient whose PCR test was found to be negative. Increased bilateral subpleural ground glass density was observed on thorax CT (Figure 1A). A partial thrombus that partially allowed flow was seen in the aortic outlet of the truncusbrachiocephalic artery in the upper extremity contrast-enhanced CT (Figure 1 B,C).
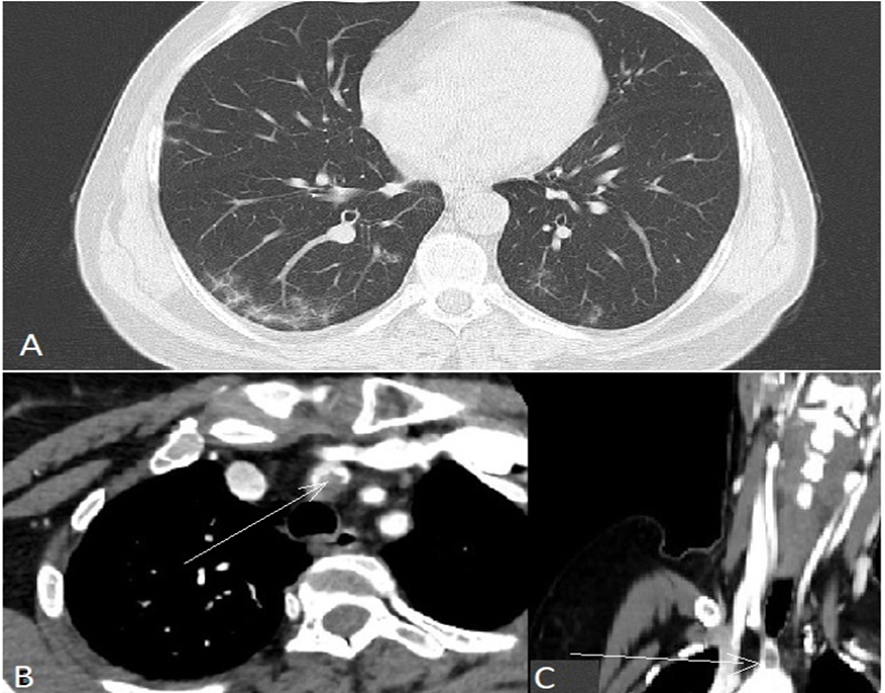
Figure 1: Figure 1 Chest CT taken one month ago (A). Thrombus at the origin of the brachiocephalic artery (B,C-Arrows).
No major embolism findings were detected in the distal arteries of the right upper extremity. The patient was accepted to have a possible COVID-19 infection. There were no major clinical findings in the patient other than minimal color change and tenderness in the right 4th finger. The capillary refill in the 4th finger was good. Neurological and other system examination results were normal. Surgical treatment was recommended to the patient first. The possible risks of surgical treatment and the undesirable situations that could occur in the absence of surgery were explained. However, the patient did not consent to surgical treatment and was discharged with recommendations and started on 100 IU/kg/12 hours of Enoxaparin for 2 weeks and 20 mg Rivaroxaban for 3 months at the treatment dose. In the follow-up examination one month later, it was observed that no additional complications developed, and the thrombus was completely cleared in the contrast-enhanced CT (Figure 2).
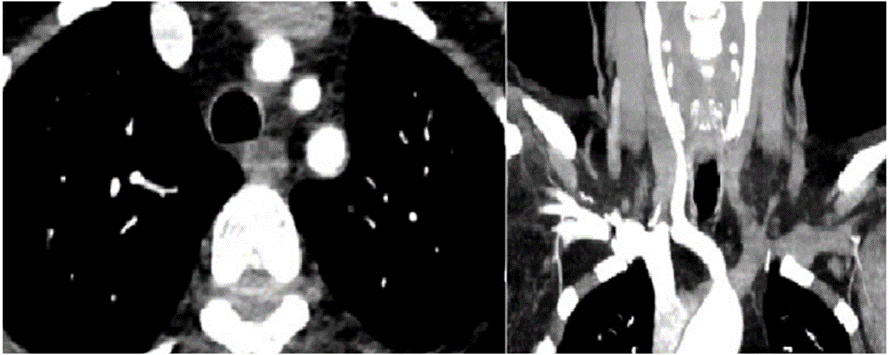
Figure 2: Contrast-enhanced CT one month after treatment.
Mural thrombi are thrombi adhering to one side of the vessel and do not occlude the lumen partially blocking blood flow and are seen in large-diameter arteries (e.g., aorta, carotids, a. iliaca).3 Large artery mural thrombi are rare pathologies with high mortality and morbidity. These rare conditions, which are detected without atherosclerosis, sometimes develop based on aneurysmdissection, but COVID-19, which was declared a pandemic in March 2020, managed to take its place among the first pathogens.4 Isolated BCAT is a rarely defined pathology in the literature and usually requires emergency surgery after diagnosis and presents with right upper extremity and/or cerebral ischemia findings.1 In the literature review, no BCAT was detected in a COVID-19 patient. The patient’s PCR test result was negative upon arrival. However, considering that the mean PCR test remained positive for 8.8 ± 3.1 days, the current findings led us to a possible COVID-19 diagnosis. Typical thoracic CT results and laboratory data also supported this diagnosis.5 Although the cause of thromboembolic events in COVID-19 is not clear, the virus’s invasion of the vascular endothelium, activation of the coagulation cascade, cytokine storm, and increased acute phase reactants are blamed.2 In large artery thrombosis, the generally accepted treatment is emergency surgery. However, complications of surgical interventions must not be ignored. The most important of these is distal embolism6. When our case applied to us, approximately 1 month had passed and during this time, there were microembolism attacks in the fingers of the right hand. Considering that the thrombus had organized in the meantime, perhaps the surgical treatment option would have led to more complications than the current pathology. The patient was completely cured with a two-week treatment with Rivaroxaban supported by Enoxaparin. In conclusion, medical treatment must not always be considered a secondary option in selected patients with large artery thrombosis. The human body is programmed to repair itself.7 Considering the seriousness of surgical trauma and its complications, we believe that this fact, supported by medical treatment, must not be ignored.
Informed consent was obtained from the patient
No conflict of interest.
ADS: Data acquisition and analysis, interpretation, drafting, critical revision, final approval.
CG: Data acquisition and analysis, interpretation, drafting, critical revision, final approval.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
