
Case Report | DOI: https://doi.org/10.31579/2578-8965/134
1 Chang Gung Memorial Hospital, Linkou, Taiwan.
2 Department of Surgery, Chang Gung Memorial Hospital, Linkou, Taiwan.
3 Department of Obstetrics and Gynecology, Chang Gung Memorial Hospital, Taipei, Taiwan.
*Corresponding Author: Liang-Ming Lo, Department of Obstetrics and Gynecology, Chang Gung Memorial Hospital, Taipei, Taiwan.
Citation: Pin H. Lin, Keng H. Liu, Liang M. Lo. (2022). Re-print: Laparoscopic Excision of a Large Gartner’s Duct Cyst. J. Obstetrics Gynecology and Reproductive Sciences, 6(6) DOI: 10.31579/2578-8965/134
Copyright: © 2022 Liang-Ming Lo. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 September 2022 | Accepted: 20 October 2022 | Published: 30 November 2022
Keywords: abdominal mass; magnetic resonance imaging; wolffian duct
Gartner’s duct cysts (GDCs) are typically small remnants of the Wolffian ductsincidentally found during a gynecologic examination. We report a case of the second largest GDC ever reported.
Gartner’s duct cysts (GDCs) are typically small remnants of the Wolffian ductsincidentally found during a gynecologic examination [1]. We report a case of the second largest GDC ever reported [2]. This case highlights the first case in the literature of a GDC managed by laparoscopic excision.
A 43-year-old nulliparous woman presented with complaints of a lower abdominal palpable mass of 1-year evolution and voiding difficulties for 6 months. A pelvic magnetic resonance imaging (MRI) (Figure 1) revealed a paracervical cyst measuring 15.4 x 13.5 cm in the right paracervical region.
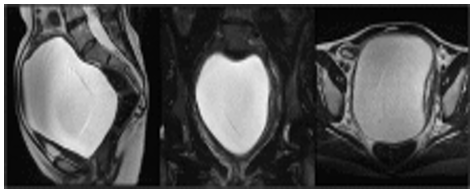
(A) Sagittal T2-weighted image demonstrated an enormous Gartner duct cyst, up to 15.4 cm in its greatest diameter in the paracervical and paravaginal region.
(B) An enhanced homogeneous cyst enclosed in a capsule on a coronal T2-weighted image.
(C) The cyst distorted the cervix onto the left side 80.
Figure 1: A magnetic resonance scan of the pelvis before the second operation.
Laparoscopic resection of the cystic lesion was planned and a myometrium was dissected by monopolar electrocautery. A well-demarcated enormous cyst with a thick capule was identified (Figure 2) and approximately 800 ml of clear serous fluid was aspirated. The cyst was carefully dissected from the uterus and then the myometrium was closed with 2-0 V-Loc™ (Covidien, Mansfield, Massachusetts). The patient was uneventfully discharged on postoperative day 2.

Figure 2: (A) Dissection of the myometrium performed by monopolar electrocautery.
(B) Intraoperative findings: A large Gartner’s duct cyst wasnoted with a thick capsule.
(C) Gross appearance of the Gartner’s duct cyst.
The pathology report revealed epithelial cells without mucin or cilia in the cyst surrounded by smooth muscle cells, compatible with a GDC (Figure 3).
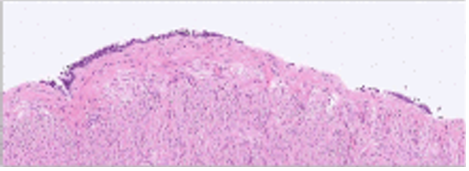
Figure 3: The pathologic image revealed the Gartner’s duct cyst wall by non-ciliated, non-mucinous epithelial cells; a surrounding smooth muscle layer was evident.
The surgical management of a GDC is controversial [3,4]. Vaginal excision has mostly been performed for enormous GDCs [5-7]. However, up to 11.4% recurrence was reported after vaginal excision [4] possibly due to incomplete excision.
Compared with the blind view during vaginal excision, laparoscopic excision for GDCs provides a direct vision of the anatomical details of internal structures in the abdomen and pelvis. Moreover, it provides a larger working space for the meticulous manipulation of surgical instruments. Furthermore, transabdominal approach provides advantages over vaginal excision for a GDC extending upward from the paravaginal region to the abdominal cavity. Therefore, we share our experience and recommend surgeons performing laparoscopic excision for GDCs in the future.
The authors have no conflicts of interest to disclose.
The authors did not receive funding for this work.
No prior presentation or publications and/or abstract/poster presentation of contents in this case report.
The dataset generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
