
Case Report | DOI: https://doi.org/10.31579/2690-4861/621
1 McMaster University, Assistant professor, Department of Pathology and Molecular Medicine, Juravinski Hospital and cancer center, Hamilton, ON, Canada.
2 McMaster University, Professor, Department of Pathology and Molecular Medicine, Saint Joseph Hospital, Hamilton, ON, Canada.
*Corresponding Author: Nermeen Feltaos, McMaster University, Assistant professor, Department of Pathology and Molecular Medicine, Juravinski Hospital and cancer center, Hamilton, ON, Canada.
Citation: Nermeen Feltaos, Samih Salama, (2025), Langerhans Cell Histiocytosis Associated with Oral Cancer. A Case Report of Unusual Association, International Journal of Clinical Case Reports and Reviews, 22(1); DOI: 10.31579/2690-4861/621
Copyright: © 2025, Nermeen Feltaos. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 November 2024 | Accepted: 03 January 2025 | Published: 08 January 2025
Keywords: 1- Langerhans cell histiocytosis (LCH);2- Oral cancer; 3- Smoking
Langerhans cell histiocytosis (LCH) is rare, particularly the adult onset. The disease can present with wide-spectrum manifestations, ranging from an isolated lesion to life threatening multisystem involvement. The association of LCH with neoplastic conditions is documented in the literature. However, the co-occurrence of LCH and oral squamous cell carcinoma (SCC) is highly unusual and raises questions about the shared nature of both diseases. Herein, we present a rare case of an unusual co-occurrence of LCH and oral SCC. The patient, who has a long-standing history of smoking, underwent an excision for SCC. Microscopic examination revealed invasive well-differentiated SCC and an adjacent distinct nodule with morphological features and immunohistochemistry expression consistent with LCH. Most adult-onset LCH presents with multisystem involvement at diagnosis, and lesions in the oral cavity may precede evidence of LCH elsewhere. Although Somatic mutations have been identified as having a key role in the pathogenesis, a reactive process is not entirely excluded. Adult-onset isolated LCH lesions should prompt clinicians to look not only for multisystem involvement but also for association with other malignant neoplasia. In addition, the association of oral SCC with LCH raises the possibility of smoking-related pathogenesis.
Langerhans cell histiocytosis (LCH) is a disease characterized by clonal expansion of myeloid precursors that differentiate into CD1a+/CD207+. It is manifested with various degrees of systemic involvement, determining the risk stratification and treatment options [1]. Swelling and ulceration are the usual presentations of oral mucosal involvement, and ulceration is typically associated with LCH lesions of the underlying bone [2]. The annual incidence rate of LCH in the pediatric population is 5-9 new cases per 1 million, and in adults, 1–2 new cases per 1 million population [3]. Although the etiology of LCH is debatable, a clonal expansion leads to a neoplastic mechanism is favored [4]. Histologically, LCH cells are generally large, round to oval, with a complex nuclear contour and a coffee-bean nuclear groove. The diagnosis requires expression of the immunohistochemical panel of CD1a and CD207 (Langerin) to differentiate LCH from other histiocytic lesions [5]. Although electron microscopy was used in the past to detect Birbeck granules, CD207/langerin immunohistochemical stain is now the surrogate marker for the ultrastructure granules [6]. This article aims to highlight a rare association and explore the potential role of smoking as a contributing factor in the development of oral LCH.
We present a 75-year-old male patient with a history of prolonged smoking. The patient presented with a non-healing 'cold sore' like lesion for several months and underwent an excisional biopsy of the lower lip. Microscopic examination revealed invasive, well-differentiated keratinizing SCC at the mucosal side of the lip. A separate, distinct nodule adjacent to the carcinoma but at the cutaneous side of the lip demonstrated large cells with relatively abundant pale eosinophilic cytoplasm and lobulated/coffee bean-shaped nuclei with open chromatin and nuclear grooves. Mitotic figures were seen. The background showed macrophages, lymphocytes and rare eosinophils. The large Cells were strongly positive for S100, CD1a, and Langerin, with a faint or partial expression of cyclin D1 and CD68. The LCH cells were negative for MelanA, HMB45, HCK and MCK. The lymphocytes expressed CD20 and CD3 in the background. We performed molecular testing for BRAF; however, the mutation was not detected.

Figure 1: A low-power magnification demonstrates invasive SCC associated with a distinct nodule of LCH

Figure 2: Invasive well-differentiated SCC (A) 10x magnification. (B) 20x magnification

Figure 3: Nodular lesion illustrates large cells with relatively abundant pale eosinophilic cytoplasm and lobulated nuclei with open chromatin and nuclear grooves. (A) 10x magnification. (B) 40x magnification (C) 80x magnification
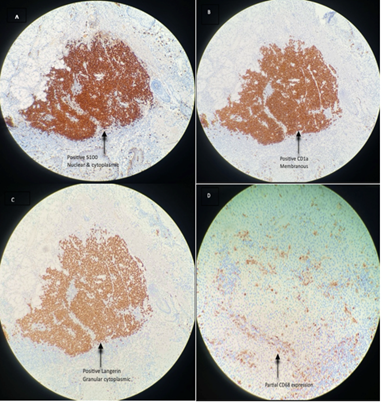
Figure 4: Immunohistochemistry of the LCH. (A) S100 (10x). (B) CD1a (10x). (C) Langerin (10x). (D) CD68 (20x)
Langerhans cell histiocytosis (LCH) remains poorly understood with heterogeneous clinical presentations [7]. LCH is a rare proliferative disorder, categorized into single- and multi-system types according to the number of involved organs [8]. Adult LCH usually presents after the fourth decade, and approximately two-thirds of patients have multi-system involvement at the time of diagnosis. Lesions in the oral cavity may precede evidence of LCH elsewhere and may include hypermobile teeth, gingival hypertrophy, or ulcers of the mucosa, tongue, or lips. [9]. Somatic mutations in CD1a dendritic cells and MAPK pathway, especially BRAF and MAP2K1, have been identified as having a key role in the pathogenesis of this disease [10]. On the other hand, developing LCH lesions as a fibroinflammatory process is still controversial, particularly in the lungs, in association with smoking [11]. Moreover, Suri et al. found that more than 90% of adult patients who developed pulmonary LCH smoked cigarettes or had second-hand smoke exposure [12].
The risk factors for developing lip SCC include ultraviolet (UV) radiation and tobacco smoking [13], which is in agreement with our case due to the prolonged smoking history. In addition, the presence of solar elastosis in the excision is consistent with the UV effect. It is unclear whether smoking and UV radiation possibly contribute to the development of the LCH as well.
The co-occurrence of LCH with other lesions is well documented in the literature. LCH may occur with non-neoplastic lesions; Jason et al. reported a case of LCH associated with vulvar lichen sclerosis (14). Furthermore, LCH association with other neoplastic diseases is common, especially other myeloproliferative neoplasms [15]. Although the association of LCH with carcinomas is encountered in different organs like the lung, thyroid, and kidney [16-18], to our knowledge and literature search, there are no reported cases of lip SCC and LCH association. This patient has no past medical or concurrent history of systemic LCH, and the lip LCH was incidentally removed with the invasive SCC. Since the treatment of LCH depends on the extent of involvement and the patient was diagnosed with a single-system disease, no further treatment was required. Although BRAF mutation was not detected in the specimen, only 60% of LCH patients harbor somatic BRAFV600E mutations localizing to CD207+ DCs within lesions [19].
Apart from this being a new rare co-occurrence of SCC and LCH in the lip, adult-onset isolated LCH lesions should prompt clinicians to look for not only multisystem involvement but also association with other malignant neoplasia. In addition, the association of oral SCC with LCH raises the possibility of smoking-related pathogenesis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
