
Research Article | DOI: https://doi.org/10.31579/2690-1919/313
Teaching Assistant, Nursing Campus Nepalgunj Tribhuvan University, Institute of Medicine, Nepal Registered Nurse, Nepal Nursing Council.
*Corresponding Author: Nisha Ghimire, Teaching Assistant, Nursing Campus Nepalgunj Tribhuvan University, Institute of Medicine, Nepal Registered Nurse, Nepal Nursing Council.
Citation: Nisha Ghimire. (2023). Knowledge Regarding HIV & AIDS among Opioid Substitution Client of Banke, Nepal, J Clinical Research and Reports, 13(3); DOI:10.31579/2690-1919/313
Copyright: © 2023, Nisha Ghimire. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 March 2023 | Accepted: 25 March 2023 | Published: 01 April 2023
Keywords: hiv aids; knowledge; opioid substitution client; nepal
The issue of HIV and AIDS in substance and drug users is of significant concern, necessitating interventions to improve knowledge about the disease among individuals undergoing opioid substitution therapy. This study aimed to assess the existing knowledge of HIV and AIDS among opioid substitution therapy clients in the Banke District of Nepal. A descriptive, cross-sectional study was conducted among 50 respondents selected using non-probability purposive sampling techniques from the Methadone Maintenance Treatment Program at Bheri Zonal Hospital in Nepal. Data was collected using a semi-structured interview schedule and analyzed using both descriptive and inferential statistics. The findings indicated that 58.0% of respondents recognized HIV and AIDS as a communicable disease, and all respondents identified unsafe sexual contact and intravenous drug use as the primary modes of transmission. Additionally, 96.0% of respondents identified multiple sex partners as a high-risk group, and 100% and 98.0% of respondents recognized that avoiding sharing needles and using condoms during sex, respectively, could prevent transmission. The study also found that the primary source of information for respondents was peer groups. The findings indicate that respondents had a moderate level of knowledge about HIV and AIDS and its treatment. The study also revealed that there were misconceptions and insufficient knowledge regarding HIV and AIDS transmission, prevention, and treatment among intravenous drug users.
Background
Acquired immunodeficiency syndrome (AIDS) is the most severe manifestation of a range of illnesses related to human immunodeficiency virus (HIV) infection. HIV transmission occurs through exposure to bodily fluids via high-risk behaviors, such as heterosexual intercourse with an HIV-infected partner, injection drug use, and male homosexual relations. Additionally, individuals who received blood or blood products contaminated with HIV, infants born to mothers with HIV infection who were breast-fed, and health care workers exposed to needle-stick injury from an infected patient are at risk [1].
The World Health Organization (WHO) designates Acquired Immunodeficiency Syndrome (AIDS) as the ultimate stage of Human Immunodeficiency Virus (HIV) infection. HIV is a retrovirus that infects cells of the immune system, compromising their functionality and rendering the individual more susceptible to infections. Despite efforts to combat the spread of HIV, the AIDS epidemic continues to expand, with global estimates indicating that over 40 million people are infected [2].
HIV remains a significant public health concern worldwide, having resulted in the deaths of more than 35 million individuals to date. In 2015, there were approximately 1.1 million deaths (940,000–1.3 million) attributed to HIV-related causes globally. The number of people living with HIV at the end of 2015 was approximately 36.7 million (34.0–39.8 million), with 2.1 million (1.8–2.4 million) newly infected individuals reported globally in the same year. Presently, only an estimated 54% of individuals with HIV are aware of their status. In 2014, around 150 million children and adults across 129 low- and middle-income countries received HIV testing services [3].
The Human Immunodeficiency Virus (HIV) epidemic in Nepal exhibits significant heterogeneity with respect to the most-at-risk populations (MARPs), geographic distribution, and risk factors in different geographic regions. The epidemic is concentrated among key populations such as female sex workers (FSWs), people living with injecting drug (PWID), men who have sex with men (MSM), and some migrants. Effective prevention interventions need to be scaled up among MARPs and their direct sexual partners. However, Nepal's poverty, political instability, gender inequality, low levels of education and illiteracy, and the stigma and discrimination surrounding HIV and AIDS make the task challenging. The first case of AIDS in Nepal was reported in 1988, and as of December 15, 2011, 19,118 cases of HIV infection were officially reported. However, due to limitations in Nepal's public health surveillance system, the actual number of infections is thought to be higher, with an estimated 50,200 people living with HIV as of 2011, and approximately 60% of those infected are unaware of their sero-status [5].
Furthermore, despite the adult population estimated HIV and AIDS infection rate being below the 1% threshold that is considered "generalized and severe," the prevalence rate marks a concentrated epidemic among at-risk populations such as FSWs, IDUs, MSM, and migrants. The National Center for AIDS and STD Control (NCASC) estimates the number of HIV cases in Nepal to be closer to 70,000 in 2012, with 6.8
Research Design
A descriptive cross sectional study design was used to gather information on knowledge regarding HIV & AIDS among drug users.
Research Setting and Population
This research was conducted at OST, setting as OPD, delivering Methadone Maintenance Treatment at BHZ at Banke, a tertiary level hospital in Midwestern region of Nepal.
Population was included client attending OST department.
Sampling Technique & Sample size
Non Probability Purposive Sampling technique was used.
Sample size was 50.
Research Instrumentation
The research instrument consists of semi structured interview by the researcher herself. The research instrument was designed in both English & Nepali version.
The Questionnaires consist of two parts-
Part I: Questions related to Socio-demographic variables.
Part II: Questions related to Knowledge regarding HIV & AIDS.
Validity and Reliability of Research Instrument
Content validity was established by extensive literature review, consulting with research advisors, statistician, subject matter experts and valuable suggestions from colleagues.
Reliability was added by pre-testing.
Ethical Consideration
Prior to data collection, formal administrative approval was obtained from research committee of Bheri Zonal Hospital,Nepal.
Informed written consent was taken from each respondent after explaining objectives of the study.
The participation in the study was voluntarily, they have the right to ask questions and that they could withdraw from the study at any time without having to give a reason.
The collected data was kept confidential and used only for research purpose.
Data Collection Procedure
Permission letter was obtained from Bheri Zonal Hospital (BHZ) & Change Team (CT) before conducting research.
Purpose of the study was explained to respondents before collection of the data.
Informed written consent was obtained from the respondents prior to data collection.
The data was collected from face to face interview schedule technique.
The average time required to complete interview was about 15-20 minutes.
Confidentiality of the respondents was maintained by using code number & information collected was used only for study purpose.
Data analysis procedure
Collected forms werechecked, edited, coded, and analyzed for its completeness and accuracy. Data was stored safely. Data was analyzed using Statistical Package for the Social Sciences (SPSS) version 20. Analyzed data was interpreted by using descriptive and inferential statistical method. Findings of the study were presented in tabular form.
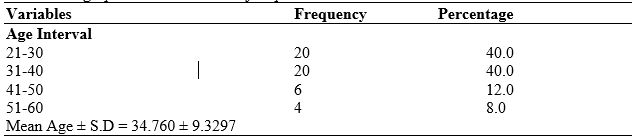
Table 1: Socio Demographic Characteristics of respondents
Table 1 shows that nearly half of the respondents (40%) were from age group 21-30 years & 31-40 years, followed by 41-50 years (12%) & 51-60 years (8%).
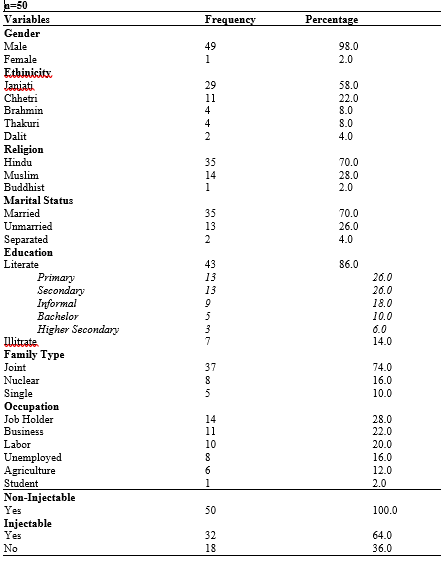
Table 2: Gender, Caste, Religion and Ethnicity of Respondents
Part II: Knowledge Related HIV & AIDS
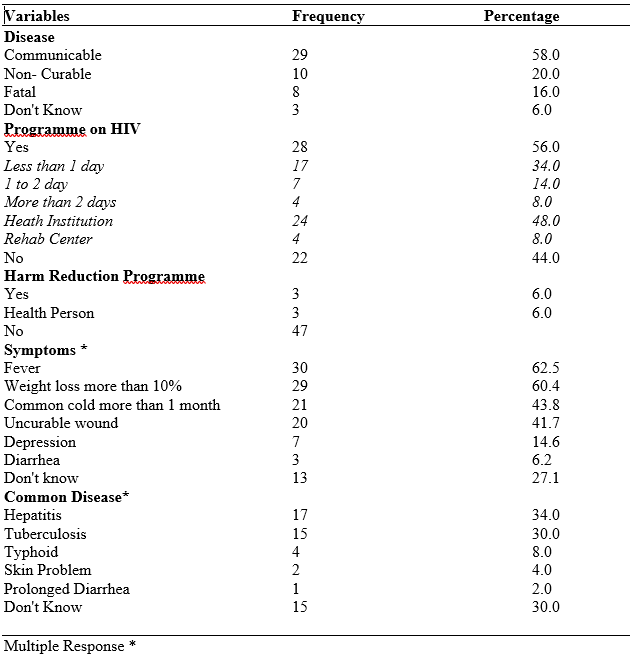
Table 3: Knowledge on HIV & AIDS, Programme, Symptoms &Common disease
Table 3 shows that out of total respondents 58% respondent represent that HIV is communicable disease, followed 20% as a non- curable disease, 16% as a fatal disease while 6% reported they don't know about HIV. Among all respondents 56% were involve in HIV programme at different session & at different place where as 44% were not involve in any programme related to HIV. It also shows that majority 94% didn't know about harm reduction programme while only 6% were known about harm reduction programme. 62.5% respondent said fever is common symptoms followed by 60.4% weight loss , 43.8% common cold, 41.7% uncurable wound, 14.6
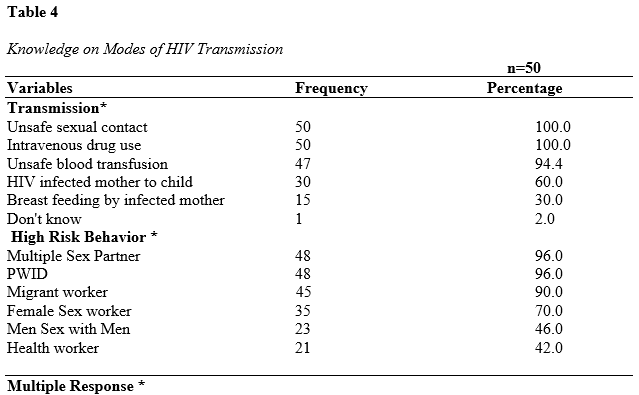
Table 4 shows majority of respondent told that major way of HIV & AIDS transmission is unsafe sexual contact 100%, same as intravenous drug use 100%, followed by unsafe blood transfusion 94.4%, mother to child 60.0% & breastfeeding 30.0% while 2.0% don't know about transmission. While 96.0% respondents believed high risk behavior of HIV transmission is person with multiple sex partner & people living with using intravenous drugs.
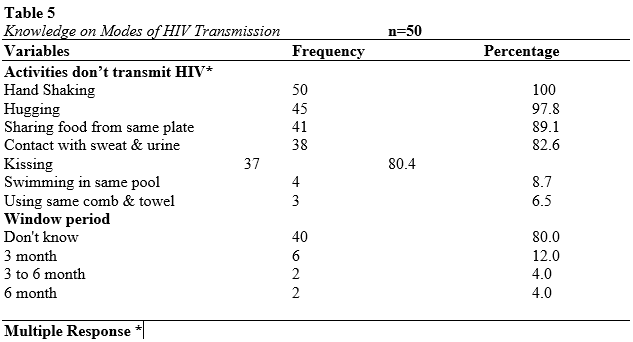
Table 5 shows, 100% respondents told hand shaking with infected person doesn't transmit HIV. Among all respondents, 80% didn't know about window period of HIV.
Table 6
Knowledge on Prevention of HIV & AIDS
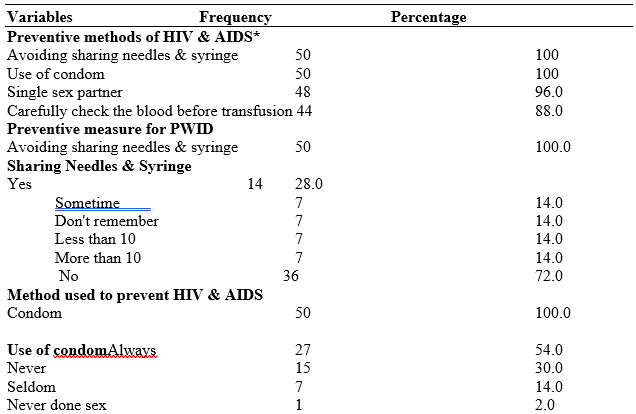
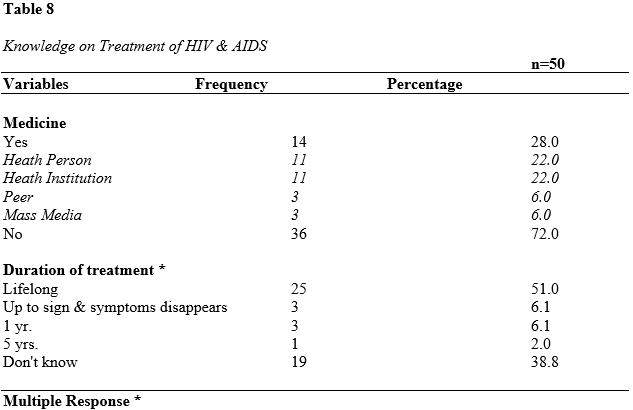
Table 8 represents out of 50 respondents, 28.0% knewabout ARV among them 22% knew through health person & health institution, 6.0% through peers & mass media. More than half (51.0%) of respondents knew about period for talking medicine of HIV & AIDS is lifelong.
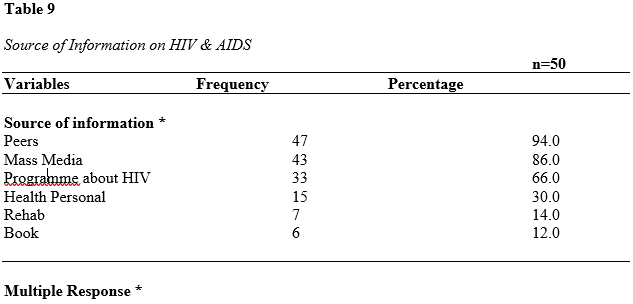
Table 9 shows majority 94.0% respondents knew about HIV & AIDS through peers, followed by 86.0% through mass media, 66.0% through programme about HIV , 30.0% through health personal , 14.0% rehab & 12.0% book .
Regarding the knowledge of HIV & AIDS, more than half 58.0% told that HIV & AIDS is communicable disease. Almost 56.0% of respondents had involved in educational programme on HIV & AIDS. Only 6.0% of respondents knew about harm reduction programme. In regarding to disease most common symptoms 62.5% of respondents answered fever, similarly about 34.0% of respondents believed hepatitis as a common disease that occur in people infected with HIV & AIDS. Different than present study, cross sectional survey by Baifeng et all (2016) stated that 93.4% had HIV & AIDS knowledge[13].
In present study 100% respondents told hand shaking with infected person doesn't transmit HIV followed by 97.8% by hugging, 89.1% sharing food from same plate, 82.6% through contact with sweat & urine of infected person, 80.0% through kissing. Similar study by Gaashet all 2003, most of the respondents believed that HIV& AIDS could also spread through handshake (82.22%), eating with the victim or sharing cups & utensils with him (64%), or use of fomites (52%). Only a few had the (4.67%) knowledge that sharing toothbrushes orblades of patients could transmit the infection to others; the majority (76.22%) was ignorant while a sizeable proportion (19.11%) did not comment at all [14].
In present study 96.0% respondents believed high risk behavior of HIV transmission is person with multiple sex partner & people living with using intravenous drug. Among all respondents (i.e.50), 80% didn't know about window period of HIV. Similar study by Gupta P et all 2013 high-risk groups, 29.4% girls and 32.7% boys opined that prostitutes were high-risk group for HIV/AIDS followed by adolescents and homosexuals (23.5% girls and 22.1% boys; 23.5% girls and 20.3% boys, respectively). Only less than 1.0% girls and 4.4% boys felt that truck drivers were high-risk group for HIV/AIDS[15].
In relation to HIV & AIDS prevention most of the respondent had knowledge about preventive way of HIV as avoiding sharing needles & syringe & use of condom was 100% & 98.0% respectively. Cent percent respondents knew the preventive way of HIV transmission on PWID. Among all respondents, 28.0% respondents told that they used to share needle & syringe. All respondents believed use of condom helps to prevent HIV & AIDS transmission. Similarly, 54.0% always used condom with his/her sexual partner, 30.0% never used condom while 14% seldom used condom during sexual contact. A snowball sample of 1127 eligible injection drug user by Chikovaniet., all (2011) shows that majority of IDUs had knowledge about how HIV is transmitted and how its transmission can be prevented. Most (99.4%) knew that sharing syringes increases the risk for contracting HIV; 97% reported that they could get new, unused syringes when needed; and 94.9% mentioned drug store as a prime source of syringes. Similar study conducted in 2006/7 with a convenience sample of 295 illicit drug users in Rio de Janeir by Bertoni.N et all (2011) almost 40% of drug users reported having never used condoms and more than 60% reported not using condoms under the influence of substances. Most drug users (80.6%) correctly answered that condoms make sex safer, but incorrect beliefs are still common (e.g. nearly 44
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
