
Research Article | DOI: https://doi.org/10.31579/2642-9756/138
1 Department of Public Health University of South Africa (UNISA)
2 Department of Public Health, Pharma College of Health Sciences
*Corresponding Author: Amenti Teka Geferso. Department of Public Health, Adama General Hospital and Medical College.
Citation: Derese Desalegn Buta, Amenti Teka Geferso, Muluadam Abraham (2023), Knowledge, Attitude, Practice and Assocaited Factors of Trachoma Among Women at Shalla District Oromia Region, Ethiopia, 2021, J Women Health Care and Issues. 6(2); DOI:10.31579/2642-9756/138
Copyright: © 2023, Amenti Teka Geferso. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 January 2023 | Accepted: 16 February 2023 | Published: 07 March 2023
Keywords: attitude; Ethiopia; knowledge; oromia region; practice; shala district; rachoma
Background: Trachoma is caused by the bacterium Chlamydia trachomatis, which is the commonest infectious cause of blindness in our globe. It can be transmitted by the discharge from infected eyes of individuals and transferred by fingers, eye-seeking flies or by clothes to the eyes of non-infected ones. Trachoma is one of the major health problems in Shalla Woreda Oromia Region, Ethiopia.
Methods: Data were collected from Shalla district community base Cross-sectional study design was conducted. Dependent Variables were Knowledge, attitude and practice of women. Simple random sampling technique were used to select the total of 661 participants based on their population. Study subjects are women age group greater than equal to eighteen years. A multivariable logistic regression analysis model was fitted to identify factors associated with the outcome variables.
Result: In this study, a total of 661 respondents were included, 554 (83.8%) had good knowledge, 213 (32.2%) had favorable attitude and 303 (45.8%) of respondents were had proper practice on trachoma prevention and control program. Primary level education AOD=18.83, 95% CI = 8.53-41.57 were had good knowledge than no formal education. Those individuals who had primary educational level status AOD= 20.2, 95% CI=4.91-25.06 were have favorable attitude about trachoma prevention when compared to no formal educational. Age group 35-44 years old were also significantly associated with favorable attitude than age group of people. Those individuals who had clean environmental (AOR, 16.37, 95% CI 9.8-27.38) were have proper practice about trachoma prevention than who had unclean environmental and regarding to latrine individual who had latrine (AOR, 2.36, 95% CI 1.71-3.26) were have proper practice about trachoma prevention than who had no latrine.
Conclusion: Considerable numbers of people have poor knowledge, unfavorable attitude and improper practice about trachoma infection. Educational level of respondents obtained as associated factor of both favorable knowledge and attitude. Similarly, age group of 35-44 years was factors of having favorable attitude while having clean environment was obtained as factors of proper practice. Improving educational status should be provided to increase knowledge and changing attitudes that contribute for good practices towards trachoma prevention and control among communities.
1.Background
Trachoma is the most common infectious cause of blindness. Repeated episodes of infection with Chlamydia trachomatis in childhood lead to severe conjunctiva inflammation, scarring, and potentially blinding in-turned eyelashes to the eye ball (trichiasis or entropion) in later life[1]. Improvement in socioeconomic and living conditions, availability of antibiotics, and introduction of National Trachoma Control Program reduced the prevalence of trachoma in developed countries, but it was persisted in resource-poor settings of Asia and Africa include Ethiopia. In 2016, as per the WHO report, trachoma is restricted to 42 countries, causing blindness/visual impairment for about 1.9 million people[2].
Infection is transmitted within ocular and nasal secre¬tions that are passed from person to person on fingers, fomites (such as cloth¬ing) and eye-seeking flies (particularly Musca sorbens). In trachoma endemic communities, children are frequently infected with Chlamydia trachomatis due to their tendency to have close contact with others and to not keep their faces free of secretions; however, the blinding effects of repeated infection generally do not develop until adulthood and it’s responsible for the visual impairment and irreversibly blind [3].
Trachoma is an ancient disease and has previously been a significant public health problem in many areas of the world including parts of Europe and North America. Today, however, trachoma is largely found in poor, rural communities in low-income countries, particularly in sub-Saharan Africa. In 1998, the WHO established the Alliance for the Global Elimination of Blinding Trachoma by 2020 (GET 2020). This promotes trachoma control through the SAFE Strategy: surgery for trichiasis, antibiotics for chlamydia trachomatis infection, facial cleanliness and environmental improvement. Where control measures have been implemented encouraging reductions in the prevalence of trachoma have been found[4]. Face washing with water and wiping with a hand might be insufficient to remove chlamydia trachomatis from the faces of children in two-thirds of cases, whereas washing with soap may be more effective for chlamydia trachomatis–positive children[5].
The multiple approach, settings-based health promotion should be continued and community engagement and leadership increased, for sustainable, behavior change for trachoma elimination. Longer term, the social determinants contributing directly to trachoma, including poorly functioning bathroom facilities and overcrowded housing, must be addressed at every level of government. These environmental improvements must be supported by health education for community-wide benefit and reduction in transmission of infection.[6].
The multi-faceted interventions for trachoma health promotion were established in the settings where people engaged in daily activity, with the aim of attaining synergistic effects and sustained population-wide behavior change. There is renewed interest in the settings-based approach to facilitate health promotion and public health action and it was anticipated that embedding trachoma related KAP in work settings may redress a previous finding that trachoma was not considered a priority in remote health services[6].
However, there are no data on knowledge, attitudes, and practices on trachoma prevention and control among rural communities in Oromia region of zones and different woredas of districts and areas with high burden of trachoma such as West Arsi Zone Shalla Woreda rural district area need to assess knowledge, attitudes, and practices of trachoma among rural communities. Therefore, this study intends to provide a broad understanding of community’s level of knowledge, their attitudes and their practices towards the available services. Therefore, a strengthened health education about trichiasis, in the health institutions of the study area as well as their referral sites, should be given for the community. From this study will enable the concerned stakeholders improve the currently existing interventions towards prevention and control of the blinding disease and in effect bring down the prevalence towards elimination of the disease in the region.
1.2 Statement of the problem
The WHO reported that trachoma was a major public health problem in most socioeconomically underdeveloped countries of the world in Africa, Central and South America, Asia, Australia, and the Middle East. Ethiopia is estimated to be the most trachoma-affected country in the world(7). As per the 2018 report of WHO weekly epidemiologic record, the number of people living in districts where active trachoma was a public health problem was 157.7 million, 88% of which in Africa and 50% of which in Ethiopia[3].
The national prevalence of active trachoma (either TF or TI) for children in the age group 1-9 year is 40.14%. Considerable regional variations are observed in the occurrence of active trachoma; the highest prevalence is in Amhara (62.6%), Oromia (41.3%), SNNP (33.2%), Tigray (26.5%), Somali (22.6%) and Gambella (19.1%). The rural prevalence of active trachoma is almost fourfold compared to the urban (42.5% rural Vs 10.7% urban). The national prevalence of trachomatous trichiasis (TT) is 3.1% with the highest prevalence in Amhara regional state (5.2%). Trachomatous trichiasis is higher in females compared to males (4.1% Vs 1.6%). Over 9 million 1–9-year-old children live with active trachoma, and 1.3 million people 15 years and older have trachomatous trichiasis. Active Trachoma and trachomatous trichiasis are concentrated in the regions of the country with high population density, namely the Amhara, Oromia, and SNNP regional states. The prevalence of trachoma is three to four fold in rural residents and among females [8]. Trachoma is highly endemic in Oromia region, of Ethiopia, especially in Arsi, Bale and Borena Zones. Prevalence of trachomatous inflammation follicular (TF) among children aged 1–9 years in the enumeration units encompassing Arsi, Bale and Borena Zones in different woreda districts area ≥ 23.8 %, ≥ 42.4% and ≥ 38.9 respectively[9].
Trachoma disease is exacerbated by various community-based practices and environmental factors. Some of the risk factors predisposing communities to the disease include; women who care for children putting them frequently in close contact with children who are the sole reservoirs of the disease-causing bacteria, water scarcity in arid and semi-arid areas where trachoma disease is mostly endemic reducing use of water for personal hygiene purposes such as facial cleanliness, utilization of sanitary facilities and indiscriminate defecation in bushes and proximity of livestock corrals to the households resulting in high fly population and the household general sanitary conditions such as poor dusting of earthen floored households acting as fomites for transmission of the disease-causing bacteria to the human eye. These predisposing factors have an impact on the prevalence and burden of trachoma disease in trachoma endemic regions [10].
The target for eliminating trachoma as a public health problem can be achieved if the SAFE strategy is properly applied. However, trachoma still remains one of the major health problems in the world. Several factors are associated with increased risk of trachoma. These include lack of water, poor personal hygiene, and environmental sanitation. Furthermore, poor knowledge, and unfavorable socio-cultural status of the community [11].
Trachoma is found in remote communities burdened with poverty, overcrowding and poor hygiene. Lack of culturally appropriate health promotion, a small trachoma workforce and lack of awareness and support for trachoma elimination in general, were early barriers. Shalla woreda is one of highest prevalence of trachoma area. For knowing of the gap of KAP of trachoma is important to preventing or reducing the prevalence of trachoma in the community and identify community perceptions on hygiene, decision maker will likely notice current practices that already reduce the transmission of infectious disease. The study on KAP provided high utility with difficult to reach participants in a program with very limited resources.
1.3 Significance of the Study
Trachoma indicating the need for enhanced interventions to ensure effective control and treatment of the eye disease to bring down the prevalence of the disease. Several studies have been done regarding the risk factors of trachoma disease in different parts of the world where trachoma is endemic. A lot more has also been documented regarding the interventions put in place to prevent and control the eye condition in communities affected by the disease. However, despite the documentation of all these information’s, the prevalence of trachoma in many areas including Kajiado County remains above the World Health Organization threshold (Trachomatous Follicular <10>
Responsibility for child care includes the washing and bathing of young children, which is usually performed by mothers, other female relatives, or young girls. Hygiene should be understood from a gender perspective. Gender informs hygiene behaviors, which place men and women at different risks. Although women are responsible for the hygiene of their children, they may not be empowered to make decisions about the allocation of household resources (e.g., money, time) for hygiene purposes. This includes access to water, soap, towels, or washcloths (if used) and the time to teach hygiene to children. Decision-making freedom is generally even more limited in areas or times of scarcity. Gender also informs the division of labor and household tasks, which affects exposure to trachoma [12].
The three aspects of knowledge of the available eye care services, attitudes towards the services and practices of the community play a significant role in determining use of eye care services. The demand for trachoma mass treatment with Azithromycin, provision of lid surgery to correct trachomatous trichiasis, and the need to improving hygienic conditions is enormous. The findings obtained from the study area of paramount importance for health providers and program managers in planning and implementing to improve prevention and control of trachoma among communities. Moreover, it is useful to policy makers to formulate appropriate interventions for implementation of the SAFE strategy.
1.4 Research Questions
1.5 Conceptual framework
A conceptual framework of determinants of KAP of trachoma among women adopted and modify from literature review, and this assisted to construct the conceptual framework for this study. Figure 1 below shows the relationships of the independent variables and dependent variables that will be studied.

Figure 1: Conceptual framework, as developed by the researcher
2.1 General Objective
The general objective of this study is to determine level of Knowledge, Attitude and Practices of trachoma and its associated factors among women in Shalla district community, Oromia regional state, Ethiopia, 2021
2.2 Specific Objectives
3.1 Study area
Shalla Woreda is one of the 12 districts in West Arsi Zone of Oromia National Regional State. The woreda had a total of 39 Kebeles, and all each kebeles had three different zones. The administrative center of this woreda is Aje (21). According to the 2007 national census reported a total population for Shalla woreda of 149,804, of whom 74,930 were men and 74,874 were women; 7,680 or 5.13% of its population were urban dwellers and the majority 142,124 or 94.87% of the population were living on rural area of the woreda [21]. But as updated information of the woreda administration was used a total population of 853,545.
3.2 Study design
A community based cross-sectional study design was conducted to assess knowledge, attitudes, and practices of trachoma and associated factors among rural communities in Shalla woreda district of Oromia Region, Ethiopia.
3.3 Population
3.3.1 Source and Study population
The study population for this study was a women closed contact to children and who would be willing to take part in activity, were interviewed. The survey was conducted by door-to-door visits and the data collector conducted interviews of willing participants. Houses would select randomly in the selected kebele. Only one individual was selected from each house based on selection by lottery method.
3.4 Inclusion and Exclusion Criteria
3.4.1 Inclusion criteria
Women from the selected a household member greater or equal to age of eighteen.
3.4.2 Exclusion criteria
A person from the selected age of less than eighteen, women who are unable to undergo interview due to serious medical or mental illness. Women with her child/children with critical ill was excluded
3.5 Sample Size and Sampling Technique
3.5.1 Sample size
The sample size was calculated by using EPi–info software with a single population proportion formula. The assumptions used were p = a proportion of previous study 50 % from a study done previously in Tigray region(11) CI = 95% confidence interval, d= 4% margin of error, 1.0 design effect and 10% non- response rate.
It was calculated as n = sample size

For the second objective sample size was calculated by using Epi info 7 StatCalc function considering the following assumption; a total population of 853,545 95% CI and 80% power was calculated about 246.
After comparing the sample size calculation from both objectives and considering 10% non-response rate, the largest sample size became 661
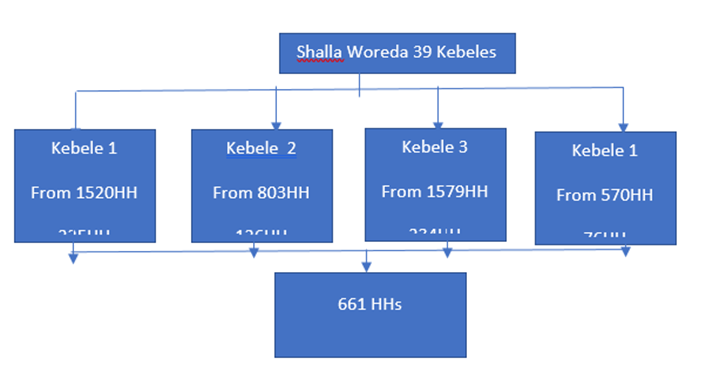
Figure 2: Schematic presentation of sampling procedure of the study participants.
3.5.2 Sampling Technique and Procedure
The study respondents kebeles in Shalla woreda district was selected by using simple random sampling by using Microsoft Excel was used to generate random numbers adding up to the required sample size from four Kebeles by giving equal chances for all kebeles in the Woreda by simple random sampling method applied in the selection of respondents within kebeles depending on their availability and willingness to participate in the study. From the selected households in their respective sub-locations and villages was used to interview the study participants. Only the women in the household member but their absence caregiver of children from household member aged eighteen years or older was interviewed. Women in the households of each kebeles were selected, the names of all the household heads of each category in each kebeles were registered separately, and representative households were selected from each of four kebelesby using systematic random sampling method. The number of respondents selected from each of a given kebeles was in proportion to the number of households categorized in to that status in that specific kebele. This is to mean that selection at level was based on Probability Proportional to Sample Size.
3.6 Study Variable
3.6.1 Dependent Variable
Knowledge, Attitude and Practice of women
3.6.2 Independent Variables
Occupation, education status
3.7 Data Collection Technique
Respondents will be interview through an interviewer-administered questionnaire developed by principal investigator. This tool obtained information on respondents’ knowledge, attitudes and their seeking practices of the trachoma. The primary questionnaire was in the English language, then translate into Afan Oromifa separately by a local senior educator as well as by the principal investigator. The two versions were then combined and finalized with an agreement on the translated version, using local language for a better understanding by participants where needed. Data would be collected by face-to-face interviews and by observations for some practice-related questions through Open Data Kit (ODK) application using smart phone. The data collectors were interview women about socio-demographic information, knowledge, attitudes, and practices on trachoma. Their responses on some practice- related questions will be verified by observational technique (availability of latrine and utilization, house compound cleanliness, having separated human and animal dwellings, and solid and liquid waste disposal methods). Enumerators who know the culture and language of that community will be selected and trained on methods of data collection and systematic approach in gathering data.
3.8. Data Quality Control and Management
During data collection, all the activities of the work will be carefully monitored and supervised. The data collectors were native to the study area. The training was given for two consecutive days by the principal investigator. The training may include an explanation of all the questions, ODK usage and practical session. Supervisor and the principal investigator were conducted intensive supervision. 5% of the sample was be pretested out of study area and all necessary correction was done accordingly before data collection. Data were cleaned & entered by the principal investigator.
3.9 Data processing and Analysis
Data were collected from server (google sheet) and then interred the data by using SPSS 20 software for processing and analysis research data. Data cleaning and editing was carried out before analysis. Bivariate analysis was done to determine the associations between each independent variables and outcome variables. All associated factors with P-value less than 0.25 during bivariate analysis were entered into a multivariable logistic regression model. Odds ratio with 95% confidence intervals were used to see the strength of association between different variables. P-value and 95% confidence interval (CI) for odds ratio (OR) were used in deciding the significance of the associations. Before inclusion of independent factors, multicollinearity was checked using cutoff points variance inflation factor (VIF) <10>0.05.
3.10 Ethical Considerations
Ethical approval of the study was obtained from the Pharma College of Health Science Research Ethical Review Committee before proceeding with actual data collection under reference number PCHS-558/13 on 11/14/2013. The Research Ethical Review Committee wrote the letter of approval to the West Arsi Zone Health Bureau and the formal letter was written to the Shalla District Administration Health Office. Respondents were given detailed information about intent, potential benefits and side effects, the right to continue or withdraw from the interview, and the aim of the study, and they were given consent to read it for those who could, and the interviewers read it for those who couldn't. Each respondent was informed that their data would be treated confidentially. Respondents had complete freedom to withdraw from the study or refuse to complete questionnaires at any time.
3.11 Operational Definition
4.1 Socio-demographic Characteristics of Study Participants
A total of 661 participants were included in the study. Of this number, 109 (16.5%) were aged 18-24 years, 281 (42.5%) were aged 25-34 years, 205 (31%) were aged 35-44 years and 66 (10%) were aged 25-34 years. The mean age of the respondents was 32.53 with a standard deviation of 8.527. Most of the participants 610 (92.2) were married and lives together with their husband, 48 (7.3%) were windows and the remained 3 (0.5) were unmarried. Almost all 655 (99.1%) of the study participants the main occupation of their family was farming and while the rest 6 (0.9) were merchant. The level of education was also assessed in this population and it was found out that up to 375 (56.7%) had no formal education. There were 178 (26.9%) and 108 (16.3%) with primary and secondary education level respectively. All of the participants in study were Muslim in their religion.
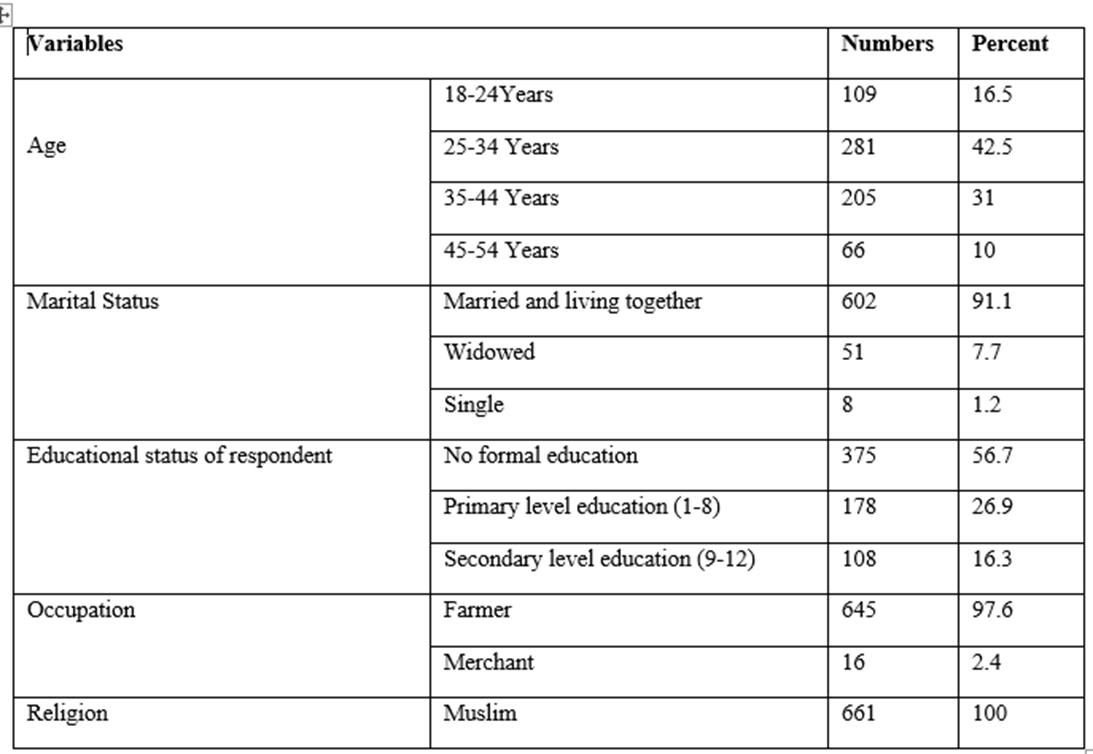
Table 1: Socio-demographic characteristics of study participants on knowledge, attitudes, and practices on trachoma in West Arsi Shalla woreda of Oromia Region, Ethiopia, 2021 (N=661).
4.2 Knowledge on Trachoma Prevention and Control
Most 537 (81.2%) of respondents had ever heard about trachoma and knew that trachoma can be transmitted from person to person 470 (71.1%) and answered correctly that trachoma can be transmitted by dirty fingers 480 (72.6%), flies 474 (71.7%), and by using contaminated towel 458 (60.3%). The majority, 463 (70.0%), of respondents knew trachoma as a preventable disease, 490 (74.1%) of respondents knew that trachoma can lead to blindness and 484 (73.2%) of participants knew trachoma can be prevented by keeping personal hygiene. Majority, 465 (70.3%) and 468 (70.8%) of participants knew trachoma can be prevented by using latrine and by improving environmental sanitation respectively.
Those whose knowledge with mean value and below were categorized into poor knowledge while whose knowledge with more than mean value were grouped into good knowledge. The mean score of respondents on knowledge was 7.25 with 3.42 standard deviations (SD). 435 (65.8%) of respondents were scored above the mean score and classified as having good knowledge on trachoma infection (Table 2)

Table 2: Knowledge of study participants on trachoma in West Arisi Zone Shalla Woreda of Oromia Region, Ethiopia, 2021 (N=661).
This study assessed knowledge, attitudes, and practices on trachoma in Shalla districts West Arsi Zone of Oromia Region, Ethiopia. Furthermore, good knowledge was significantly associated with good practices towards trachoma prevention and control. In this study, 88.7% of respondents had ever heard about trachoma. This result was almost the same with the studies conducted in Northern Ethiopia (89.2%), Southern Ethiopia (92.6%), and Bangladesh (86%) and Indigenous Northern Territory communities (88%). However, it is higher than the report in Kenya (65.7%) of participants had heard about trachoma [22]. The discrepancy could be due to the differences in social mobilization activities in different sites and studies methods. The current study shows that 78.7 % of respondents knew trachoma can be transmitted from person to person. The respondents mentioned that trachoma can be transmitted by contaminated fingers, flies, and contaminated towels. Similar studies from Kenya and Ethiopia reported that the most reported mode of trachoma transmission was contact with that the majority (84.5%) of respondents knew trachoma as preventable disease [6, 10, 11]. The participants responded that trachoma can be prevented by using latrine, improve environmental sanitation, not using common towel, and washing hand and face with soap. Having knowledge on washing face, not sharing towels, and environmental sanitation was important on prevention of trachoma infection respondents correctly answered the cause of trachoma.
Regarding attitudes of respondents in the current study, the majority the total of, 84.4% of respondents strongly agree and agreed that taking mass drug administration is important to prevent and control trachoma and 78.4% of the respondents took mass drug administration. This result is almost comparable with the other reports from Amhara and Tigray regions, and the coverage of mass drug administration ranged from 76.8% to 93.3%[16,22 ]. On the other hand, 55.8% and 18.3% of respondents strongly agreed and agreed that trachoma can be prevented by utilizing latrine respectively. However, only 39.9% of households were utilizing a latrine. The finding on latrine utilization was almost the same as previous studies in Tigray region, Ethiopia (37.1%) [11].
Regarding to practice of respondents in this study, the majority 78.4%, of respondents took mass drug administration, and 76.2% of households had separated human and animal dwellings, 39.9% were utilizing a latrine and 75.2% had clean house compounds. Out of 358 (54.2%) of the study participants had a proper practice toward trachoma infection. This result is almost similar but some result was different due to the differences in social mobilization activities in different sites and studies methods with the study conducted in Northern Ethiopia Tigray the majority 88.1%, of respondents took mass drug administration, and 76.8% of households had separated human and animal dwellings. However, only 37.1% were utilizing a latrine and 30.4% had clean house compounds. Out of (35.6%) of respondents were classified as having good practices towards trachoma prevention and control [11].
This study showed that education of the respondents was significantly associated with knowledge of the women about trachoma. Those study subjects had no formal education level 46.4 % was had poor knowledge on trachoma than primary 82.6% and secondary 94.2% of educational level. This is almost with the study in Arbaminh Southern Ethiopia, whose had no educational level 66% had poor knowledge than other primary 84% and secondary educational level 88%[18]. The current study revealed that mothers who have good knowledge on trachoma was significantly associated with good practices on trachoma prevention and control. This is supported by a study from Kenya, reported that knowledge was significantly associated with trachoma prevention and control practices[10]. Increasing knowledge of trachoma transmission and prevention (e.g., F&E-related preventive behaviors) is important to improve practices of trachoma prevention and control[23]. This might be due to the reason that if someone knew benefit of personal hygiene and environmental sanitation, women could practice to prevent and control trachoma[12].
This study showed that education of the respondents was significantly associated with attitude and practice on trachoma. Those study subjects who had no formal education educational level had likely to have unfavorable attitude and unproper practice on trachoma prevention program when compared to their counterparts, respectively. This result is consistent with a study done in Kenya in which a significant proportion of individuals who had no formal or primary education had inadequate knowledge, attitude and practice regarding trachoma[10]. The possible explanation of this finding would be the fact that people who a higher educational background had had better for getting adequate knowledge, attitude and apply proper practice for prevention and control program of trachoma.
6.1 Conclusion
In this study implies that areas with high burden of trachoma need to improve communities’ knowledge, attitudes, and practices on trachoma prevention and control in order to eliminate trachoma as a public health problem. Improving educational status should be provided for rural community increase good knowledge and changing their attitude that contribute to behavioral changing and increase good practices towards trachoma prevention and control among communities.
6.2 Recommendation
Therefore, based on this study findings, recommend that
7. Data Availability
The data used to support the findings of this study are available and can be accessed from the primary author on reasonable request.
8. Funding statement
This research was conducted without the financial support from other organizations or funding agency and it was covered by the authors.
9. Additional Points
9.1 Limitation of the study
This study has several limitations. First, this study followed a cross-sectional study design. Therefore, causal inferences may not be established and compared with face-to-face interviews. There might be missed some factors that could influence knowledge, attitudes, and practices that were not considered in the model. I used a limited number of questions to measure the level of knowledge, attitude, and practice. Thus, additional assessments would be important, using all aspects of KAP towards trachoma, to determine the actual extent of KAP in the general population. Additionally, the unstandardized and inadequate assessment of knowledge, attitudes and practices towards trachoma should be developed via focus group discussion and in-depth interviews and constructed as multi-dimensional measures.
9.2 Strength of the study
In terms of strengths, to begin with, this study consisted of face-to-face interviews by trained data collectors that ensure completeness and validity of data collection. Furthermore, face-to-face interviews remove ambiguities among the general population and are helpful in describing the purposes of research activities. However, data collection was carried out by trained and diligent data collectors, and was cross-checked for completeness and thoroughness by the PI and this study has very important findings for strengthening the prevention and control of trachoma in the study area and areas with similar set up.
10. Conflicts of the interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
11. Author Contribution
The authors contributed significantly to the work of this study and the correspondent participated in its drafting, revision/review. All authors agree to be responsible for the content of the work. The agreement was made with the journal to which the article was sent for publication.
12. Acknowledgement
My sincere appreciation will also go to the Pharma College, College of Medicine and Health Science, School of Public Health for giving me this opportunity.
I would like to express my deepest gratitude and appreciation to my advisors for their unreserved all-rounded support and enriching comment which have been very helpful in improving and guiding the whole research proposal and thesis development period.
Lastly, but not least, I would like to congratulate different Pharma College Department of Public health coordinator for support me for all things and Shalla Woreda Health office who provided me background information about the district.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
