
Review Article | DOI: https://doi.org/10.31579/2768-2757/142
Federal State Budgetary Educational Institution of Higher Education “Kazan State Medical University” of the Ministry of Healthcare of the Russian Federation.
*Corresponding Author: L.M. Mirolyubov., Federal State Budgetary Educational Institution of Higher Education “Kazan State Medical University” of the Ministry of Healthcare of the Russian Federation.
Citation: L.M. Mirolyubov, (2024), Kazan Version of the Congenital Heart Defects Classification of John Kirklin, Journal of Clinical Surgery and Research, 5(7); DOI:10.31579/2768-2757/142
Copyright: © 2024, L.M. Mirolyubov. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 September 2024 | Accepted: 21 October 2024 | Published: 31 October 2024
Keywords: cardiovascular surgery; diagnosis; cardiac surgeon
Complex cyanotic heart disease (CCHD) with balanced pulmonary blood flow, stable hemodynamics and stable hypoxemia is operated on in accordance with the Fontaine principle, not in 3, but in 2 stages, others - the tetralogy of Fallot, a double-chambered right ventricle, etc. - are operated on radically and instantaneously.
Congenital heart defects with a large left-to-right shunt and low pulmonary resistance begin to decompensate through a hyperkinetic heart syndrome, which is an indication for surgical treatment. These patients constitute about 17%.
The remaining majority of patients - 65-70% have the ability to grow up to a year or older. A grown child has a significantly lower overall surgical risk.
Organizational measures implemented in the recent decades in the field of cardiac and vascular surgery as part of special purpose programs of the Government of the Russian Federation and the Ministry of Healthcare of the Russian Federation directly supervised by the leading Cardiac Surgeon of the Ministry of Healthcare of the Russian Federation, academician L.A. Bokeria, led to a significant improvement in the situation in this specialty in Russia. In particular, regarding the treatment of the congenital heart disease (CHD), the number of surgeries in the Russian Federation (approximately 15 thousand per year) exceeds the number of children born with the congenital heart disease (12 - 13 thousand per year), as a result the need to prioritize surgical waiting lists will soon be eliminated, and over time the above-mentioned figures will even out. (L.A. Bokeria, R.G. Gudkova. Cardiovascular Surgery in Russia, 2015, p. 42.) In the Republic of Tatarstan, surgical prioritization with regards to the congenital heart disease was eliminated in 2005 courtesy of additional funding from the President of the Republic of Tatarstan M.Sh. Shaymiev. Since then, all children diagnosed with congenital heart disease are registered at birth and are operated on at the optimal time, which reduces the risk of postoperative complications and death. (Mirolyubov L.M. Congenital Heart Defects in the First Year of Life, 2008, p. 149.) It is a known fact that 70% of congenital heart defects have to be operated on within the 1st year of life, 28-30% of them in the neonatal period, and only about 30% of children with a congenital heart disease can be monitored for several years without fear of fatal complications. (Burakovsky V.I., Bokeria L.A. Cardiovascular Surgery, 1989, 1996, p. 58-66) In order to make it easier to understand the pathological processes occurring in the body of a CHD patient, as well as to streamline the thinking of practicing physicians, a multitude of classifications has been created: E. Taussig (1948), S. Marder (1953), I. Littmann and R. Fono (1954), A.N. Bakulev and E.N. Meshalkin (1955), P. Wood (1956), L. Jonash (1960), Bakulev NCCVS classification (1982), J. Kirklin (1984), J. Perloff (1991), International Classification and Congenital Heart Disease Nomenclature (2000), etc. Each of the aforementioned classifications is divided into congenital heart disease groups by anatomy, hemodynamics, and potential complications. These classifications help practicing physicians in the study of congenital heart defects, facilitate understanding of the processes that occur in a sick body, nevertheless, in our opinion, they are too cumbersome and contain insufficient regulatory information that can be part of the assigned diagnosis and serve as indications for surgery. The 1984 classification proposed by John Kirklin, one of the founders of global cardiac surgery, is considered the most renowned among the cardiologists and cardiac surgeons.
In this classification, patient groups and optimal timing of their treatment are clearly identified, which is very important in formulating a treatment strategy. However, this classification lacks names of defects and reasons-indications for surgical treatment. We decided to make up for this shortcoming based on the possible, probable, and the occurred hemodynamic disturbances, using virtually the same congenital heart disease groups. The first version is as follows (Figure 1).
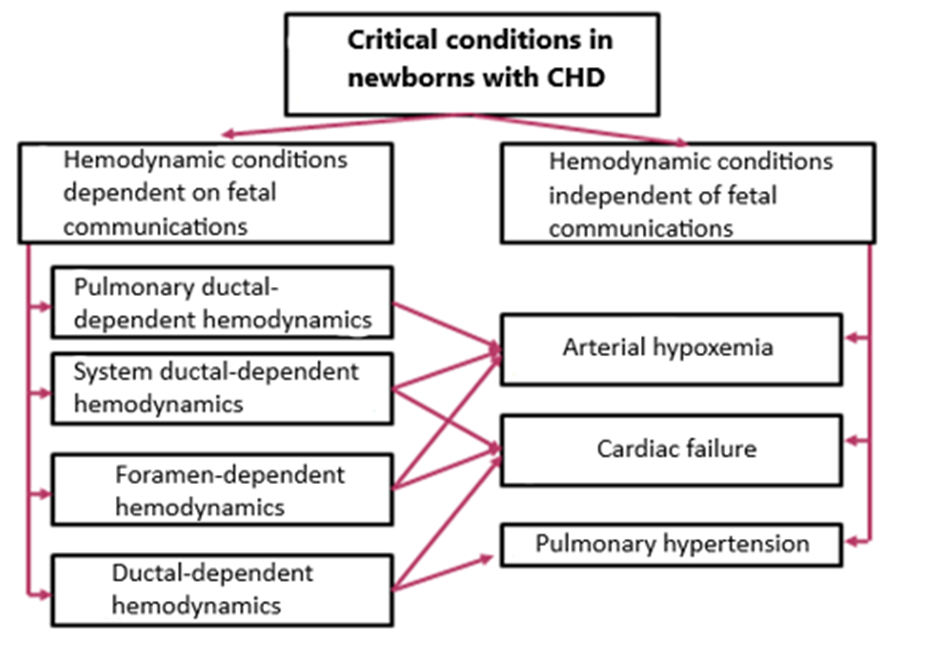
Figure 1: Prognosis of critical conditions in newborns with congenital heart disease.
The figure made by author.
Fetal communications - Arantziev duct, the foramen ovale and the open arterial duct provide blood circulation to the fetus, and should be closed spontaneously after childbirth. The unpredictability of their closure underscores the urgency of the operation.
Fetal echocardioscopy is a rather complicated examination and therefore cannot have a 100% reliability. The average indicators of reliability of the prenatal diagnosis of congenital heart defects in a fetus are 80-85%. In a number of cases, a delivered baby had an unanticipated heart defect. Future work on improving the classification led us to the need to decipher all the other cases of treatment of CHD patients, which are provided below (Figure 2).
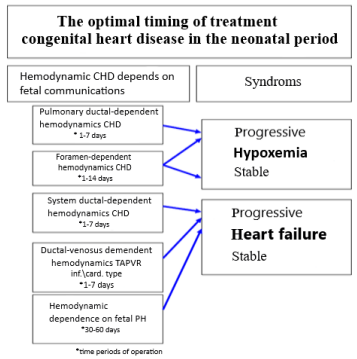
Figure 2: The optimal timing of treatment congenital heart disease in the neonatal period.
The figure made by author.
The so-called critical heart defects that occur in newborns account for 28-30% of all congenital heart diseases. If critical hypoxia or critical heart failure occurs even once (often they complement each other), the patient’s chances of survival are reduced manifold. From this point of view, obstetricians, neonatologists, local pediatricians and other related specialists should know the preventive and emergency measures to avoid such critical conditions. The group with pulmonary ductal-dependent hemodynamics includes malformations, where the only source of filling the pulmonary circuit is an open arterial duct (OAP), a.k.a ductus: pulmonary atresia, critical pulmonary stenosis, simple form of the transposition of the great arteries, tricuspid atresia, hypoplastic right heart syndrome, a critical form of tetralogy of Fallot. The group with systemic ductal-dependent hemodynamics includes malformations, where the only source of filling the greater circuit is an open arterial duct (OAP) (ductus): coarctation of the aorta, interruption of the aortic arch, critical stenosis of the aortic valve, hypoplastic left heart syndrome (HLHS) and their variations. In both patient groups, the open arterial duct determines the level of blood circulation in the lesser and greater circuits. Therefore, the first aid measures should consist of titration of prostaglandin E1 and the abolition of oxygen therapy, since oxygen has a spasmodic effect on the open arterial duct. The remaining part of the therapy is non-specific and aims to normalize the patient’s homeostasis. The foramen-dependent hemodynamics combines diagnoses where the blood flow through the foramen ovale is crucial for filling the lesser or greater circuits: the simple form of the transposition of the great arteries (after a few days, as the pulmonary resistance decreases), hypoplastic left heart syndrome (HLHS), tricuspid atresia (TA), supracardiac and intracardiac total anomalous pulmonary venous return (TAPVR). In these cases, the decreasing size of the foramen ovale determines the decompensation of blood circulation in the child’s body, which dictates the need for its expansion according to the endovascular method of Rashkind. Some critical defects have “dual subordination” of hemodynamics. Often it depends on the level of resistance of the pulmonary vessels. Hemodynamics of the ductus-venosus occurs in only one such case. In the event of infracardiac total anomalous pulmonary venous return (TAPVR), the aggravated heart failure is determined by the natural shrinkage and binding of the Arantziev duct, which connects the portal vein and the vena cava, which can prevent the outflow of blood from the lungs to the foramen ovale. In a newborn with an abnormal discharge of the left coronary artery from the main pulmonary artery, coronary circulation is compensated for with high pulmonary resistance. With a natural decrease in pressure in the pulmonary bed, the “steal” phenomenon is set into motion, i.e. reverse blood flow through the left coronary artery from the coronary bed to the pulmonary artery, which causes severe left ventricular heart failure due to hypoxia of the left ventricle and interventricular septum (Figure 3).
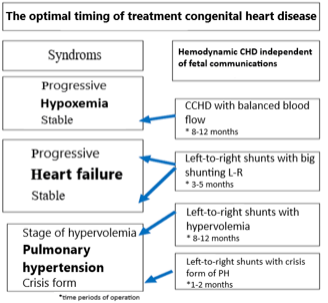
Figure 3: Optimal terms of treatment of congenital heart diseases.
The figure made by author.
The group of heart defects, where fetal communications do not affect hemodynamics, constitutes about 70% of congenital heart defects that “quietly” survive the neonatal period, and where hemodynamic indications for surgical treatment appear after the age of 1 month.
One of the most “troubled” patient groups is the one with left-to-right shunts complicated by the pulmonary hypertension crisis (PH). At the age of 1.5-2 months when the patient is suffering from pulmonary hypertension crisis or its analogues, surgical treatment is indicated. Options for one- or two-stage treatment are selected from the standpoint of collective experience and the reliability of the result. Such patients make up about 15%. Complex cyanotic heart disease (CCHD) with balanced pulmonary blood flow, stable hemodynamics and stable hypoxemia is operated on in accordance with the Fontaine principle, not in 3, but in 2 stages, others - the tetralogy of Fallot, a double-chambered right ventricle, etc. - are operated on radically and instantaneously. Congenital heart defects with a large left-to-right shunt and low pulmonary resistance begin to decompensate through a hyperkinetic heart syndrome, which is an indication for surgical treatment. These patients constitute about 17%. The remaining majority of patients - 65-70% have the ability to grow up to a year or older. A grown child has a significantly lower overall surgical risk. We have determined the recommended timeframe to provide surgical treatment for congenital heart disease based on the literature data and more than 20 years’ worth of clinical experience that culminated in the realization that the patient’s low weight and small age are in and of themselves factors that aggravate the already high risk of surgical interference. The long-term postoperative complications alone can be explained by the high hydrophilic properties of a newborn’ skin that has to be sewn up and the high growth rate of organs and systems in the first year of life. Based on this stipulation, we believe that the formula “the sooner the better” does not work for all heart defects.
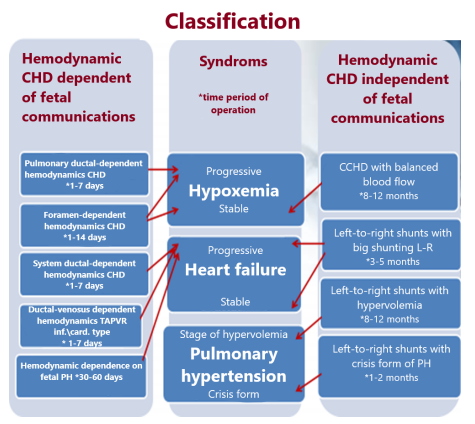
Splitting the patients into groups, i.e. making yet another attempt at classification was first proposed by the author and then presented at the public defense of a doctoral dissertation within the walls of the Bakulev Research Center of Cardiovascular Surgery (Academic Advisor - academician L.A. Bokeria) in April 2005. For convenience sake, both parts of the classification table can be merged into one, where syndromes are presented in the center, and groups of CHD patients can be found on the right and left sides. In 2002, this table used as a diagnostic and treatment algorithm was included in the order of the Ministry of Healthcare of the Republic of Tatarstan concerning the diagnosis and treatment of congenital heart disease. Since that year, it has been successfully utilized in both pediatric cardiac and cardiac surgical practice throughout the entire territory of the Republic of Tatarstan. Admittedly, the above-mentioned classification is just a small fraction of extensive organizational measures taken by the Ministry of Healthcare of the Republic of Tatarstan that led to consistent and highly effective provision of medical care to children with congenital heart defects not only in Tatarstan, but also in Privolzhsky Federal District. The unified platform for understanding congenital heart disease in our republic facilitated the dialogue between primary care physicians and specialists as a result of a clear cut division of patients that require generic treatment into groups of emergency, urgent, delayed and “scheduled” patients. The classification that we have devised does not contradict, but complements the globally recognized classification of John Kirklin, making a case for hemodynamically justified indications for surgery. In the past 15 years, since starting applying the classification table in Tatarstan, it has been put into practice in the Tyumen region, the Khanty-Mansiysk Autonomous District, and Kazakhstan. Following the modern trends in computerization of diagnostic and treatment processes, the proposed classification can serve as a foundation for creating electronic algorithms that will facilitate remote patient consultations. It is necessary to add to all these qualities well-grounded clarity surrounding the sequence of surgical procedures if a patient has multiple congenital anomalies, for example, congenital heart defects + pathology of the gastrointestinal tract, congenital heart defects + pathology of the genitourinary system, brain, etc.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
