
Research Article | DOI: https://doi.org/10.31579/2641-0419/227
Central Clinical Hospital of the Ministry of Interior and Administration, Woloska 137 Str. 02507 Warsaw, Poland
*Corresponding Author: Katarzyna Byczkowska, Central Clinical Hospital of the Ministry of Interior and Administration, Woloska 137 Str. 02507 Warsaw, Poland
Citation: Katarzyna Byczkowska, Agnieszka Pawlak, Robert Gil. (2021) Katz Frailty Syndrom has no Predictive Value in Low-Risk Patients Undergoing Transcatheter Aortic Valve Implantation Katarzyna Byczkowska, Agnieszka Pawlak, Robert Gilw. J. Clinical Cardiology and Cardiovascular Interventions, 4(16); Doi:10.31579/2641-0419/227
Copyright: © 2021 Katarzyna Byczkowska, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 27 September 2021 | Accepted: 06 October 2021 | Published: 12 October 2021
Keywords: severe aortic stenosis; frailty syndrome; TAVI
Background: Aortic stenosis is a disease of the elderly people, with multiple comorbidities and often with the frailty syndrome. Therefore, we decided that frailty as a clinical factor requires precise characterization as it is a valuable supplement to the risk stratification in transcatheter aortic
Valve implantation (TAVI).
Objective: The aim of our study was to evaluate the prognostic value of the Katz frailty scale in patients undergoing TAVI in relation to the risk of mortality assessed with the STS scale.
Material and methods: The study included 105 patients with severe aortic stenosis (AS) treated with TAVI at the Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior. In our group, the Katz frailty syndrome confirmed in all patients, and 48% in the advanced stage.
Results: Statistical analysis showed a significant difference between survival and Katz frailty score before TAVI. Analysis using Cox's model confirmed a significant prognostic value for the Katz frailty syndrome before TAVI. Patients with moderate to severe frailty on the Katz score (values ≤ 4) had a 13,68 times higher risk of death per year compared to the group with Katz frailty syndrome ≥ 5. Multivariate regression analysis indicated that Katz frailty score and STS score were prognostically significant factors of cardiovascular death in patients undergoing TAVI.
Conclusion: The Katz frailty score had a significant prognostic value in the high- and intermediate risk patients. Katz frailty score and STS risk score significantly correlated with the risk of death from cardiovascular causes in frailty patients undergoing TAVI.
Aortic stenosis (AS) is the most commonly diagnosed valve disease in the world [1,2]. Pharmacotherapy is associated with a poor prognosis [3] and a mortality rate of 30-50% within 2 years of the onset of clinical symptoms [4-6]. AS is a disease of the elderly, with multiple comorbidities and often the frailty syndrome. Approximately 30% of patients are disqualified from cardiac surgery [7,8].Classic risk scores have been developed to predict mortality and periprocedural complications in patients undergoing cardiac surgery [9-12]. However, they do not include factors such as cognitive decline and difficulties in independent daily activity, and have limitations in predicting mortality in the population of patients undergoing transcatheter aortic valve implantation (TAVI). Several studies have shown that frailty is associated with higher morbidity and all-causes mortality in patients undergoing cardiac surgery or TAVI [13-17]. In our group, the frailty syndrome concerned all patients, and 48% in the advanced stage. Therefore, we decided that frailty as a clinical factor requires precise characterization as it may be a valuable supplement to the risk stratification of TAVI. So far, it has not been possible to establish one universally accepted scale of frailty syndrome that would be the reference for better prognosis in patients undergoing TAVI.
Objective
The aim of our study was to evaluate the prognostic value of the Katz frailty scale in patients undergoing TAVI in relation to the risk of mortality assessed with the STS scale.
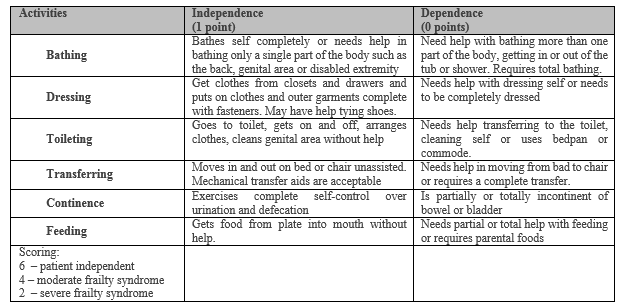
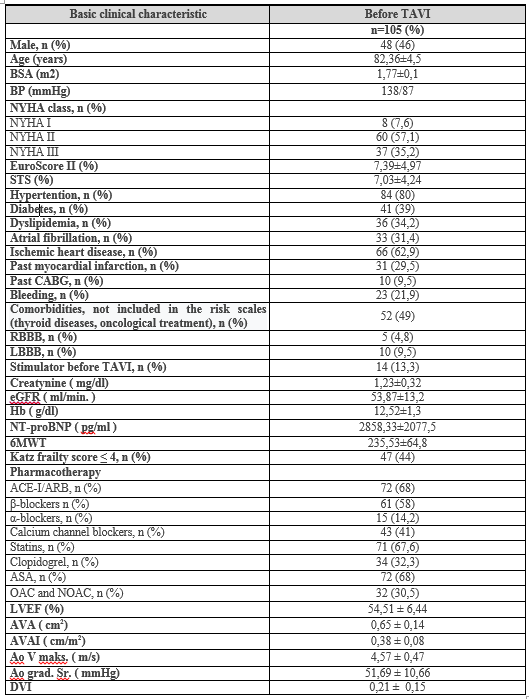
Study populationThe study included 105 patients with severe aortic stenosis (mean age 82,36±4,5; 46% men) and the Katz frailty syndrome treated with TAVI in the Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior and Administration. Inclusion criterion was severe high gradient aortic stenosis treated with TAVI. Severe AS was diagnosed on the transthoracic echocardiography and determined by the following parameters: AVA <1> 40 mmHg. The decision on qualifying patients for TAVI, vascular access and the type of valve was made by an interdisciplinary heart team. All patients underwent laboratory tests, ECG, echocardiography and was assessed based on the STS scale and the Katz frailty scale (Table I) (11).
We were used five types of bioprothesis - Medtronic CoreValve 43,8% (n=46), Medtronic Evolut R 31,4% (n=33), Edwards Sapien 7,6% (n=8), Symetis Accurate 13,3% (n=14), and St. Jude Medical Portico 3,8% (n=4). The following access were used: transfemoral in 88,6% (n = 93) patients, trans-apical in 6,7% (n = 7), trans-aortic in 1,9% (n = 2) and trans-clavicular in 2,9% (n = 3). Follow-up observations were carried out at 1 month and 1 year.
In order to assess the normality of a change in the application of the Shapiro-Wilk test. In the absence of normal use, the Mann-Whitney test. In the study mode of the Kaplan-Meier method of survival, and the survival functions were compared using the log-rank test. The Cox hazards model was used as a multi-feature condition that is important to indicate which variables are significant factors influencing survival. To assess the influence of the investigated explanatory possibilities on the dichotomous variable, one-dimensional and multi-dimensional logistic regression were used. The critical significance level (α) for all tests was 0.05 (α = 0,05). Statistical analysis was performed with the use of Statistica v.12.5 (StatSoft).
General characteristics of the studied population
The mean STS score was 7,03 ± 4,24% (STS ≥ 8% – 23,6% of patients, STS 4-8% - 40%, STS ≤ 4% - 36,4%). The Katz frailty syndrome, grade ≤ 4, was found in 44,8% of patients. The clinical characteristics of patients qualified for the TAVI procedure are presented in Table II.
Katz frailty syndrome
Mild or moderate and severe frailty in the Katz scale was observed in patients in 55,2% or 44,8%, respectively (Table III). The greatest reduction in the number of patients with Katz frailty score ≤ 4 was observed in the high-risk patients (p ≤ 0,05) after 1-month follow-up and in the intermediate- and high-risk patients after 1-year follow-up (p ≤ 0,05, p ≤ 0,05 respectively). These relations were not observed in low-risk patients (p > 0,05) (Table III).


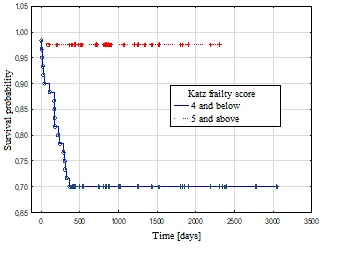
There was a statistically significant difference between survival and the Katz frailty syndrome assessed before TAVI (log-rank test, p = 0,0008) (Figure 2). The median survival time was 817 days (Q1, Q3: 408 days, 1,229 days) in patients with Katz scores ≤ 4 and 867 days (Q1, Q3: 389 days, 1,249 days) in patients with Katz scores ≥ 5. 1-year mortality of patients with moderate and severe Katz frailty syndrome was 30%, and with mild Katz frailty syndrome was 3% (p ≤ 0,001).
One-month and 1-year all-causes mortality after TAVI in high- and intermediate-risk patients was a significantly dependent on Katz frailty score (p ≤ 0,05, p ≤ 0,05 respectively). There was no significant change (p > 0,05) in the low-risk patients (Table III).
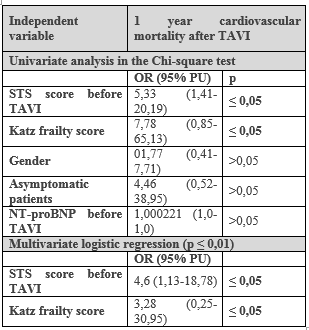
The Cox proportional hazard model confirmed a significant prognostic value for the Katz frailty syndrome prior to TAVI (p ≤ 0.05). Patients with moderate to severe frailty (values ≤ 4) had a 13,68 times higher risk of death (Table IV).

The multivariate logistic regression model indicated the Katz frailty syndrome and the STS risk score before TAVI were prognostically significant factors of cardiovascular death in patients undergoing TAVI (p ≤ 0,01). Patients with moderate and severe Katz frailty syndrome (values ≤ 4) had a risk of cardiovascular death 3,28 times higher than those with Katz frailty scores ≥ 5 (p > 0,05). When switching the surgical STS risk category before TAVI from low to intermediate, the risk of death from cardiovascular causes increased 4,60 times, while if the surgical STS risk category was changed from intermediate to high, the risk of death from cardiovascular causes was higher 21,16 times (p ≤ 0,05) after TAVI (Table V).
The optimal selection of patients with severe aortic stenosis for the TAVI procedure, taking into the frailty syndrome, remains the subject of many studies and analyzes [5-8,11–14,16]. Our study shows that the stage of Katz frailty syndrome is an important parameter in the assessment of patients before TAVI and has a prognostic value in assessing the risk of death after TAVI, also in depending on the risk in STS score. Our analysis indicate that the Katz frailty score had a significant prognostic value, especially in intermediate- and high risk patients, but no in low-risk patients. Moreover, together with the STS risk scale predicts the risk of death from cardiovascular causes after TAVI.Our data confirm that the Katz frailty syndrome is a significant indicator of mortality in patients after TAVI and these data are consistent with the results presented in previous publications and meta-analysis [11,13-16,18-20]. At the same time, we showed that 1-year all-causes mortality after TAVI in high-risk and intermediate-risk patients was a significantly dependent on Katz frailty score.
In recently published studies, survival after TAVI was significantly associated with the advancement of the Katz frailty syndrome, and the frailty turned out to be an independent predictor of mortality [20-26]. Moreover, in a study by Rogers et al. it was shown that the frailty syndrome, both independently and by adding it to the risk assessment on the classic STS scale, predicted an all-causes 30-days and one-year mortality after TAVI [9].
There are single studies analyzed the effect of the frailty syndrome on cardiovascular mortality after TAVI. In the Li et al. study, the assessed of geriatric parameters, including the Katz frailty scale, were significantly associated with all-causes and cardiovascular mortality one year after TAVI [18]. Frailty was one of the most important predictors of all-causes mortality, but also of myocardial infarction and stroke in a 9-month follow-up. In our study, we showed that patients with severe SA and the stage of Katz frailty scale ≤ 4 show significantly higher cardiovascular mortality in one-year follow-up after TAVI. Additionally, multivariate regression analysis indicated that the model of the Katz frailty score and the STS risk scores was a prognostic factor of cardiovascular death in frailty patients undergoing TAVI (p ≤ 0,01).
The use of the Katz frailty scale before TAVI to assess high-risk patients in the STS risk scale allows us to further refine the prognosis of patients undergoing TAVI. This has been demonstrated in the above-cited works as well as in the present publication. Interestingly, the Katz frailty scale allows us to differentiate the prognosis of patients with moderate risk in the STS risk score, reaching statistical significance in 1 year follow-up (p≤ 0,05). In contrast, patients with low risk of STS scale showed no differences in prognosis depending on the Katz frailty scale. In low-risk patients in our study, regardless of the Katz frailty scale, no deaths were observed either in one-month or one-year follow-up. Other researchers, such as Bo et al. also showed the best prognosis of patients with low risk of STS scale, and the Katz score ≤ 4 did not differentiate the prognosis despite the fact that deaths were reported in this group (3% vs. 0% and 4% vs. 0%, respectively) [27].
Frailty syndrome may be a consequence of severe SA, but also severe SA seems to exacerbate the symptoms of frailty. We observed a statistically significant reduction in the symptoms of the Katz frailty syndrome in a 30-day and one-year observation (Figure 1). Our data indicate the possibility of interrupting the progressive impairment of mobility and loss of independence in elderly patients, which may have a significant impact on improving the quality of life in TAVI population of patients.
Our study complements the growing amounts of evidence supporting the need to assess the frailty syndrome in patients undergoing TAVI. However, in future post-TAVI mortality prediction tools, a standardized assessment of the frailty scores should be largely considered.
Limitations
The strength of our study is assessment of the relationship of the Katz frailty syndrome with the classical STS risk score and their impact on the clinical results after TAVI. However, there are a few limitations to consider. First, we had a small population. Second, the observation time was relatively short. Third, in the study population, different types of bioprotheses were used during TAVI procedure, which may affect the results obtained.
The stage of the Katz frailty syndrome turned out to be significantly associated with one-year mortality after TAVI, both all-causes and cardiovascular. The demonstrated reduction in the number of patients with moderate and severe frailty syndrome, as well as the reduction of the symptoms of the frailty syndrome indicate the possibility of interrupting the progressive limitation of mobility in patients with severe aortic stenosis treated with TAVI. Therefore, the TAVI procedure can be considered an appropriate therapeutic intervention. The predictive value and compliance of the risk stratification at the patient level was significantly improved by considering the simultaneous STS and Katz frailty scores. The Katz frailty score had a significant prognostic value, especially in intermediate- and high-risk patients, but no in low-risk patients. Therefore, estimating the stage of the Katz frailty syndrome before TAVI qualification can`t help stratify risk in low-risk patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
