
Case Report | DOI: https://doi.org/10.31579/2641-0427/26
1 Department of Trauma & Orthopaedics, Royal Cornwall Hospitals NHS Trust, Treliske, Truro, TR1 3LQ.
*Corresponding Author: I Pengas, Department of Trauma & Orthopaedics, Royal Cornwall Hospitals NHS Trust, Treliske, Truro, TR1 3LQ.
Citation: I Pengas, C Brennan, M Flintoft-Burt and a Gough, (2022). Isolated popliteal tendon avulsion: favourable outcomes following surgical repair. Journal of Orthopedics and Surgical Sports Medicine. 4(1). DOI: 10.31579/2641-0427/26
Copyright: © 2022 I Pengas. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, providedthe original work is properly cited.
Received: 11 November 2021 | Accepted: 23 December 2021 | Published: 06 January 2022
Keywords: popliteus tendon; postero-lateral corner; knee
The Popliteus tendon forms part of the postero-lateral corner complex responsible for stability to varus stress and restraining external rotation movements of the knee. It also prevents anterior translation of the femur on the tibia.In a crouched position Popliteus is the only muscle preventing the femoral condyles gliding forward on the tibia and, as the only tendinous structure in the postero-lateral corner, it also has an important proprioceptive role in the knee.In addition, the Popliteus tendinous bands along with the ligaments of Humphry and Wrisberg protect the lateral meniscus from being distorted during rotation by allowing it to follow the lateral condyle of the femur.It was initially postulated that a Popliteus tendon injury could not occur in isolation without the involvement of the posterolateral corner complex (PLC),however subsequent reports have countered this by demonstrating that isolated Popliteus tendon avulsion is a possible, albeit a truly rareinjury.
The Popliteus tendon forms part of the postero-lateral corner complex responsible for stability to varus stress and restraining external rotation movements of the knee. It also prevents anterior translation of the femur on the tibia [1]. In a crouched position Popliteus is the only muscle preventing the femoral condyles gliding forward on the tibia and, as the only tendinous structure in the postero-lateral corner, it also has an important proprioceptive role in the knee [1,2]. In addition, the Popliteus tendinous bands along with the ligaments of Humphry and Wrisberg protect the lateral meniscus from being distorted during rotation by allowing it to follow the lateral condyle of the femur [3].It was initially postulated that a Popliteus tendon injury could not occur in isolation without the involvement of the posterolateral corner complex (PLC) [4], however subsequent reports have countered this by demonstrating that isolated Popliteus tendon avulsion is a possible, albeit a truly rareinjury[5–11].
In the paediatric, skeletally immature, population the number of cases reported in the literature are very low [5,7,12]. We present a case of an isolated Popliteus femoral avulsion in a skeletally immature patient that was identified and treated acutely with surgical repair. The patient was followed-up with PROMs, clinical and radiological assessment until full return to pre-injury sporting activity level. The patient and his parents have consented to presentation, publication and medical photography.
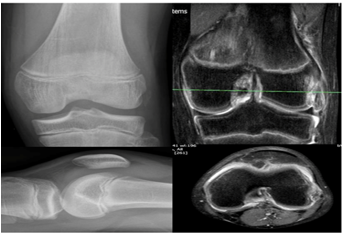
A skeletally immature male patient aged 14 presented to our UK trauma unit following a twisting injury to his left knee whilst playing rugby. He was subsequently unable to complete the game due to pain and there was significant knee swelling within the first 24 hours. The injured knee continued to be painful and examination in the acute knee clinic demonstrated a stable knee with mild laxity of his lateral collateral ligament (LCL). He had tenderness over the lateral joint line and the lateral femoral condyle. Dial test was negative but there was a block to flexion beyond 90 degrees. Initial radiographs demonstrated an avulsion fragment from the lateral femoral condyle and a lipohaemarthrosis. Urgent MRI scan of the knee confirmed a displaced bony avulsion fragment from the femoral popliteal attachment with no other intra-articular injury (image 1).
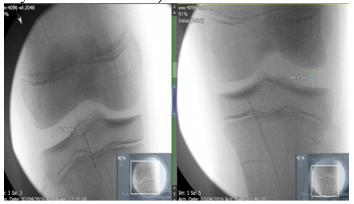
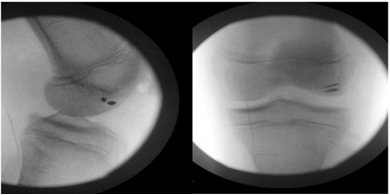
Surgical repair was undertaken 18 days after the initial injury. Examination of the knee under anaesthesia confirmed a stable knee with mild laxity on varus stress but with a firm end point. This was compared to the contralateral knee which demonstrated equal laxity, confirmed on fluoroscopic imaging. Both knees under varus stress demonstrated an equal gap (image 2 -performed by the senior author IP).
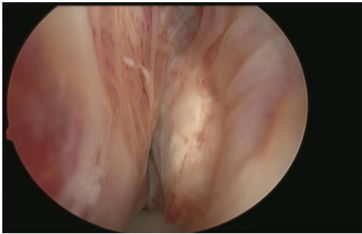
There was a mechanical block to flexion resulting in a 20 degree flexion deficit compared to the contralateral knee. Diagnostic arthroscopy confirmed the MRI findings of normal intra-articular structures with an isolated avulsed femoral condyle fragment from the popliteal tendon attachment. This was retracted posteriorly but still contained within the lateral gutter (image 3).
An arthroscopically assisted ‘mini open’ repair was performed under image intensifier guidance (image 4).
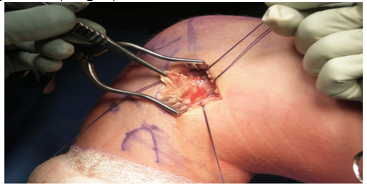
The lateral collateral and anterior lateral ligament were identified and preserved during the dissection. The anatomic position of the avulsed fragment bed was determined using arthroscopic visualisation and marked using an 18 gauge needle. Fluoroscopic imaging confirmed the needle’s position. The repair was performed using two 3.5mm anchors inserted into the bed of the avulsed popliteus tendon with the tendon end anatomically reduced and stabilised. This was done under image intensifier guidance, avoiding the physis and any damage to articular cartilage (image 5).
Post-operative rehabilitation initially focused on swelling reduction with strict cryotherapy sessions. The patient was allowed to fully weight bear immediately following surgery, but the knee was immobilised in a hinged brace locked in extension for the first 2 weeks. Closed chain exercises commenced from 2 weeks post operatively with the brace unlocked 0 – 90 degrees of flexion, though it remained locked in full extension for mobilisation. This was the case for a further 4 weeks. Radiographs were performed post-operatively at 4 weeks to assess the integrity of the repair, which showed the repair remained well situated. This was followed by an MRI scan confirming anatomical reduction of the repair and healing.
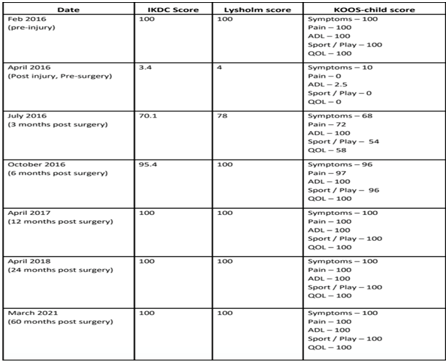
Throughout the rehabilitation period IKDC, Lysholm and KOOS-child scores were used to monitor progress. The patient had returned to his pre-injury levels of sporting activities, including full contact rugby and snowboarding, by 12 months after surgery. All PROM scores at 12 months had returned to 100% and remained so at 5 years post operatively (Table 1).
.
This case discusses the rare presentation of an isolated popliteal tendon avulsion in a skeletally immature patient and has highlighted that successful outcomes can be achieved following surgical management.
The injury was identified following clinical suspicion and examination. The initial radiographic findings and MRI scan supported the clinical findings. An anatomical surgical fixation was performed using suture anchors into the epiphysis with care taken to avoid injury to the physis or articular cartilage. This is similar to a technique as described by J. N Liu et al [13].
The reported incidence of isolated PLC injuries in the literature is less than 2% and the incidence of an isolated popliteus avulsion within this subgroup is expected to be even lower than that [14,15]. The sentiment for treatment of an un-displaced and isolated PLC injury in the adult population, in the absence of instability, is still non-operative management [15–17]. Treatment of this injury pattern in the paediatric population has little evidence base in the current literature where only a couple of case series exist. These all have low patient numbers and have reported successful outcomes with both non-operative management as well as surgical repair. Often they do not report any long term follow up or PROMs data, which can be missing entirely [8,18].
One case report [10], consisting of 2 patients treated non-operatively for isolated popliteus tendon avulsion, highlighted successful return to normal function however no PROMs data was obtained and there was no long term follow up beyond a phone call to each patient, at 2 years and 6 months respectively. Non-operative management of other knee ligamentous injuries in the paediatric population, such as anterior cruciate ligament (ACL) injuries demonstrated up to100
In the absence of instability and with the knee exhibiting a full range of motion there perhaps is an argument for truly un-displaced isolated popliteus avulsion injuries to be treated non-operatively. However, early surgical repair of the avulsed tendon can be safely performed and may provide a more predictable outcome. In this case with displacement of the avulsed fragment and a mechanical block to flexion, surgical intervention is recommended. Lack of surgical intervention would expose the patient to the potential risk of permanent altered knee kinematics, instability and the risk of growth disturbance.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
