
Research Article | DOI: https://doi.org/10.31579/2641-5194/021
1 University of Queensland, School of Medicine, Rural Clinical School, Toowoomba, Australia, Medical Officer – Qld Health, Australia.
2 Department of Internal Medicine, Toowoomba Hospital, Toowoomba, Australia
*Corresponding Author: James Elliott, University of Queensland, School of Medicine, Rural Clinical School, Toowoomba, Australia, Medical Officer – Qld Health, Australia.
Citation: Elliott J. and Gaffney L., (2021) Is being a prisoner, indigenous or having a psychiatric illness an acceptable limitation to treatment access for chronic hepatitis c infection? J. Gastroenterology Pancreatology and Hepatobilary Disorders. 5(2) DOI: 10.31579/2641-5194/021
Copyright: © 2021, James Elliott, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 March 2021 | Accepted: 10 March 2021 | Published: 08 April 2021
Keywords: psychiatric illness; psychiatric illness; chronic hepatitis c virus
170 million people worldwide are infected with chronic hepatitis c virus (HCV) [1]. There are an estimated 226700 people infected in Australia and it is the most common indication for liver transplantation in this country [2]. Despite this, overall treatment uptake remains low at <2% of patients infected undergoing treatment per year [3]. Rates of admission to hospital with decompensated liver cirrhosis are expected to increase by 190% by 2030 [4]. Cure of chronic HCV infection requires complex treatment regimens for several months.
170 million people worldwide are infected with chronic hepatitis c virus (HCV) [1]. There are an estimated 226700 people infected in Australia and it is the most common indication for liver transplantation in this country [2]. Despite this, overall treatment uptake remains low at <2>
This is a retrospective cohort study of patients treated for chronic HCV infection at the Toowoomba Liver Clinic over a 3 year period (2010-2012). Inclusion criteria was all patients who received any treatment for their HCV infection during the 3 year period. Treatment was mainly “dual-therapy” and consisted of subcutaneously administered pegylated-interferon and ribavirin tablets for 12 months. There were 23 patients who had “triple therapy” which consisted of dual therapy + oral telepravir or bocepravir and this treatment course was 6 months duration. There was no exclusion criteria. Data were collected including treatment setting (i.e. prison vs community), HCV genotype, indigenous status, comorbidities, contact with psychology services, treatment interruptions/discontinuations, and follow up rates to confirm cure (defined as sustained virological response (SVR) 24 weeks after treatment completion). The mean/median/mode number of visits with a physician was just 2, with treatment delivered predominantly via a full-time hepatitis nurse over the phone or face-to-face. Patients could also have their care delivered via a GP shared-care model, and had access to psychologist service provided by the hospital. The primary outcome was treatment completion, and secondary outcome SVR, and so the particular treatment regimen received by each patient was of secondary importance and did not influence the main results of the study.
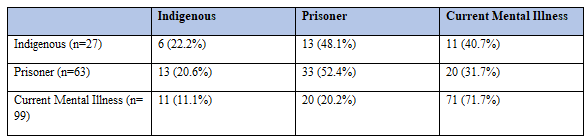
Of the 243 patients who received treatment, 74 were prisoners and 169 were community-based. The vast majority of patients included in the study were male, smokers, and had genotype 1 or 3. See table 1 for patient characteristics of all patients who were available for follow-up (183 patients). 49 prisoners completed treatment (66.2%) versus 117 community-based patients (69.2%). 31 treated patients were indigenous and 212 were non-indigenous. 22 indigenous patients completed treatment (71.0%) versus 144 non-indigenous patients (68.0%). Regarding psychiatric diagnoses, 105 had a current psychiatric illness and 138 did not. 69 patients with a current psychiatric diagnosis completed treatment (65.7%) versus 97 patients without (70.3%). See table 2 for treatment completion rates. Unsuccessful completion of treatment was common (31.7%). Of the 243 patients included in the study, all had dual therapy (pegylated-interferon plus ribavirin) treatment, and 23 patients had triple therapy (dual therapy + telepravir or boceprevir). A subgroup analysis was performed due to 14 patients having their care transferred to another treatment centre. In this patient cohort of 229, there were 81 patients (35.4%) who were neither indigenous, mentally ill, or prisoners (see table 3 for further breakdown and overlap of these “at-risk” groups). There was no statistically significant evidence that being indigenous, a prisoner, or having a current mental illness is an independent risk factor for unsuccessfully completing treatment (see table 4). There was evidence, however, that prisoners were over twice the risk of being lost to follow up (OR 2.095; p= 0.040) and that indigenous patients were at similar risk of being lost to follow up (OR 2.343; p = 0.058) (see table 5).



Chronic HCV is a global problem1-2 and the leading cause of liver fibrosis, cirrhosis, and liver-related morbidity and mortality in the world. Restriction of treatment occurs unconsciously through delivery modality biases even in our modern health care systems. In Australia, there is new data demonstrating an increased burden of chronic HCV infection among specific priority populations, with the incidence ratio of hepatitis c among Aboriginal and Torres Strait Island people increasing between 2015-2017, and 12% of all new chronic HCV diagnoses occurring in correctional facilities 7.
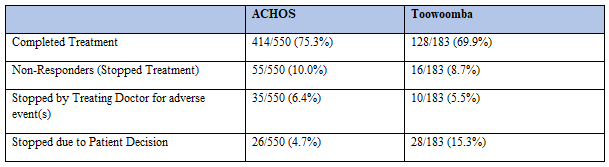
In the Australian Chronic Hepatitis C Observational Study (ACHOS), the overall SVR was 59.5% (327/550)8. This institution’s SVR (for patients not lost to follow up) was 60.1% (110/183) which is comparable. ACHOS cohort excluded patients who had previously received treatment, and also those lost to follow up. Their SVR was a 12-week post treatment completion blood test, rather than the standard 24-week post treatment blood test recommended (and used at this institution). In comparison, despite the lost-to-follow up rates at this institution, there was robust data in this single-centre cohort study to support the offering of treatment to a wide-range of patients who are both vulnerable and often perceived to be unlikely to achieve a cure.
These results indicate chronic HCV sufferers can achieve equal treatment completion rates regardless of the treatment setting, indigenous status or whether they have a current mental illness. This is despite the data in this study showing that prisoners and indigenous patients were more likely to be lost to follow up. These results contradict misconceptions about patients’ suitability for treatment, reinforcing the need for expanded treatment settings for infected patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
