
Case Report | DOI: https://doi.org/10.31579/2578-8868/171
Institute of Neurology and Neurosurgery of Cuba Department of Neurosurgery Spinal Surgery Working Group 29th street to D Vedado, La Habana 10400 Cuba.
*Corresponding Author: Norbery J. Rodríguez de la Paz, MD, Institute of Neurology and Neurosurgery of Cuba Department of Neurosurgery Spinal Surgery Working Group 29th street to D Vedado, La Habana 10400 Cuba.
Citation: Norbery J. Rodríguez de la Paz, Oscar Quiroz Osorio, Emmanuel Batista Geraldino, Alfredo Daniel Alemán Bacallao, Mercedes Rita Salinas Olivares, Calixto Machado (2021) Intradural Dorsolumbar Disc Herniation: Case Report and literature Review. J. Neuroscience and Neurological Surgery. 8(4); DOI:10.31579/2578-8868/171
Copyright: © 2021 Norbery J. Rodríguez de la Paz, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 13 March 2021 | Accepted: 27 April 2021 | Published: 06 May 2021
Keywords: intradural disc herniation, herniated lumbar disc, magnetic resonance imaging; laminoplasty; discectomy
Intradural disc herniation is a rare entity, representing between 0.26% and 0.30% of all herniated discs. 92% of cases occur in the lumbar spine, more frequent at the L4-L5 level. The diagnostic and therapeutic conduct performed in a 61-year-old male patient who came to the office with a one-year and six-month history of dorsolumbar pain is described, accompanied by sensory alterations in the lower limbs. In view of the exacerbation of symptoms, a simple magnetic resonance study was performed, observing an intraspinal, intradural, extramedullary lesion at the D12-L1 space. An intradural disc herniation is suspected. After being evaluated the case in the group of Neurosurgeons (Group of Spinal Surgery) of the Institute of Neurology and Neurosurgery of Havana, it is proposed to carry out surgical treatment, which consisted of the extraction with microsurgical technique of the Herniated disc, preserving the vertebral anatomy through the laminoplasty technique, an open book variant. The patient evolved satisfactorily after three months of follow-up. It is concluded that intradural disc herniation should be included among intradural, extraxial lesions of the spine. By means of the magnetic resonance study, a group of imaging signs that support the preoperative diagnosis of this lesion can be described. Surgery is the definitive therapeutic method and allows an accurate diagnosis of spinal herniation to be established.
Herniated discs represent a common manifestation of degenerative spinal disease. They originate from a tension failure of the annulus fibrosus to contain the nuclear portion of the disc in gel form1. Intradural disc herniation (IHD) constitutes a condition where the nucleus pulposus moves into the dural sac, separating from the intervertebral disc, previously passing through the posterior common longitudinal ligament (LLCP) [2]. In 1942 Dandy published the first case of a patient with HDI, since then only a low percentage of them have been reported in the medical literature. This entity represents between 0.26% and 0.30% of all herniated discs, 3% occurs in the cervical region, 5% in the thoracic region, and 92% occurs in the lumbar spine, more frequent at the L4- level. L5. There is a predominance in males, during the fifth and sixth decades of life. The patient frequently presents a picture of chronic back pain with acute exacerbation of pain accompanied by a rapidly onset focal motor defect [2,3].
Magnetic resonance imaging (MRI) with or without contrast can demonstrate the level of herniation and its possible intradural location, but only intraoperative findings confirm intradural disc extrusion. Surgical treatment for spinal disc herniation is usually subsequent open surgery with standard durotomy to remove herniated disc fragments, with good to fair results. In cases of late presentation, a worse result occurs [4].
Due to the low incidence of intradural disc herniation, less than 1%, the difficulties in its diagnosis and the complexity of the surgical treatment, a case of a patient with a D12-L1 HDI is presented, with the aim of describing the diagnostic and therapeutic conduct based on a review of the literature.
PRESENTATION OF THE CASE
61-year-old male patient with dorsolumbar pain of one year and six months of evolution, pain of mild to moderate intensity, with irradiation to the gluteal region, with transitory improvement after the administration of analgesics and antineuritics. Later it begins with a burning sensation, cramping and numbness in the posterior region of the thighs and legs. In the last 2 months the pain becomes intense and persistent, making it impossible for him to walk and making defecation difficult as it is very painful. He experienced no relief despite drug treatment, rectal ozone therapy, and nerve blocks.
On physical examination, antalgic left dorsolumbar scoliosis was observed. The flexion-extension and lateralization movements of the trunk, gait, the sitting position (more than 5 minutes) and the Valsalva maneuvers cause intense pain in the dorsolumbar region. Palpation of paravertebral muscle masses is painful (D10-L5). Presence of hyposesthesia and dysesthesia in the gluteal region, posterior thigh and legs bilaterally. Normal patellar and achillian osteotendinous reflexes.
In high field magnetic resonance study (3T) (Figure. 1). In sagittal view (in T2 weighting) hypointense image of 1 x 1 cm is observed, of intra-spinal, intradural, extramedullary location at the level of the intervertebral space D12-L1, at the point of transition from the medullary cone to the cauda equina, which with fragment of intervertebral disc. In axial section (T2 weighting) the lesion in the form of a “hawk beak” is observed, anterior to the nerve structures, which produces compression of these. Signs of channel narrowing are seen from L2 to S1, more accentuated at the level of L5-S1.


Given the clinical and imaging findings, an intradural disc herniation is diagnosed at the D12-L1 level, without ruling out other intradural, extramedullary entities. A surgical approach is followed through a posterior approach to the thoracolumbar spine. In the prone position, with the upper extremities extended, under general anesthesia, a 7cm incision is made at the level of the midline, centered on the D12-L1 interspace, dissected by planes until identifying the thoracolumbar fascia, which is opened in line media, preserving the supraspinatus ligament, the paravertebral musculature is deiostized and laminoplasty is performed in the open book variant, cutting the right D12-L1 sheets bicortically and the left ones monocortically at the laminophacete junction. The dural sac is exposed and under microscope visualization a 2 cm long right paramedian durotomy is performed. A greyish-white lesion is immediately observed, with few adhesions to the sac and nerve structures, it is carefully dissected from caudal to cephalad, until its extraction (Figure. 3 A and B). We proceed to repair the ventral potion of the sac and close the durotomy (hermetic durorrhaphy). The D12-L1 sheets are repositioned and fixed (Figure. 3 C) and the closure is completed by planes to the skin.

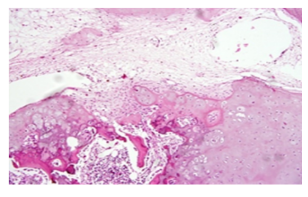
The diagnosis of intradural disc herniation is confirmed by pathological study that reports fibrocartilaginous tissue with myxoid degeneration and calcifications, ossification of part of the bone marrow formation tissue and areas of cartilage necrosis compatible with nucleus pulposus (Figure. 4).
The patient had a hospital stay of 5 days, evolving favorably, with considerable improvement in symptoms at discharge. A regular outpatient follow-up was carried out, recovering fully 3 months after surgery.
Intradural disc herniation represents a rare entity in spinal surgery, it can be considered a complication of an intervertebral disc herniation where perforation of the posterior common longitudinal ligament (LLCP) and dura mater occurs [5]. The location at the level of the lumbar spine is the most frequent (92%), with the following distribution: L4 – L5 (55%), L3 – L4 (16%), L5 – S1 (10%) [3]. In the reviewed studies, no cases were reported with location of the IHD at the dorsolumbar level (T12-L1) as described in this patient.
Its etiopathogenesis is not yet clear, several authors have described a group of factors responsible for its occurrence: a) adhesions between the fibrous ring, the CLL and the dura mater (congenital or acquired), b) congenital stenosis of the spinal canal, with reduction of the epidural space, c) congenital or iatrogenic thinning of the dura mater [6].
Patients with this condition generally describe a history of chronic back pain, with severe exacerbation of the condition and a progressive neurological defect7. At the level of the lumbar region, it may present as a Cauda Equina Syndrome in two thirds of patients or simulate the insidious installation of a spinal tumor [8].
HDIs are often misdiagnosed, confused with other extramedullary intradural lesions such as schwannomas, neurofibromas, lipomas, meningiomas, squamous tumor, arachnoid cyst, ganglioneuroma or metastasis [2,8,9]. In this case, preoperative diagnostic doubts were raised, not ruling out the possibility of other intradural injuries.
Improvements in advanced imaging techniques have made it increasingly possible to recognize lumbar disc hernias in symptomatic and asymptomatic individuals [1,2]. MRI with or without contrast is the method of choice for the diagnosis of IHD. The classic image is a mass originating from the intervertebral disc with signal hypointensity in T1 and T2 weights. Imaging findings include discontinuity of the LLCP, entry point of the disc into the dural sac, variable enhancement of the contrast of the herniated disc, the sign of "hawk beak" or "point of beak" in the axial T2 view (compressed triangular image laterally along the cartilaginous border of the annulus fibrosus) [3,6]. The latter has been found by different authors (Liu CC-20118, Aprígio RM-20193, Thohar-Arifin M-20202) as in our study.
In 2001, Mut et al. Proposed a classification of intradural disc herniation into: Type A - intradural disc herniation and Type B disc herniation in the nerve root sheath, which can only be diagnosed intraoperatively [3].
In several case studies (Wasserstrom R-199310, Aprígio RM-20193) the presence of contrast enhancement in the form of a ring on MRI with gadolinium has been highlighted, which occurs as part of a process of peripheral neovascularization and chronic granulation, and allows to differentiate a spinal disc from infections or tumors. The finding of this sign in the MRI performed on our patient supported the presumptive diagnosis of IHD.
At present, it has been reported that the use of high-resolution 3D magnetic resonance imaging CISS (constructive interference in steady state) sequences allows to accurately represent HDI. This sequence should be taken into account when IHD is suspected to optimally guide the surgical approach in complex cases [6].
The main treatment of IHD is surgical and consists of the removal of the herniated disc material. The dura and nerve roots require special care and attention during the examination. Challenges in exploring the dura of the anterolateral segments represent a common problem. Thick adhesions between the disc and the dura have been reported at the time of surgery while the dural sac tends to be rough, tight, and immobile. For these reasons, the microsurgical approach through a median or paramedian dural incision is recommended for better visualization of the hernia, avoiding damage to the nerve roots, these can be minimally stimulated to prevent neurological dysfunction [2].
In the case presented, microsurgical extraction of the herniated disc was achieved, protecting the nerve structures involved and preserving the vertebral anatomy through D12-L1 laminoplasty.
Kim HS et al. Used a transforaminal endoscopic treatment in a patient with intradural disc herniation at the L2-L3 level, they achieved endoscopic excision of the intradural disc fragments through the original rupture in the anterolateral aspect of the dura mater, performed the sealing with dural patch and Gelfoam without the need for lumbar drainage. The clinical results obtained were positive after a follow-up of 8 months [4]. The extension of endoscopic surgery to this condition offers new therapeutic options today.
HDI should be included among intradural, extraxial spinal injuries, despite being a very low frequency entity. By means of the MRI study, a group of imaging signs that support the preoperative diagnosis of this lesion can be described. Surgery is the definitive therapeutic method and allows an accurate diagnosis of spinal herniation to be established.
CONFLICT OF INTERESTS
The authors declare that they have no conflict of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
