
Case Report | DOI: https://doi.org/10.31579/2692-9406/089
1 Professor and Head/Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy, No. (1) Defence Services General Hospital, Myanmar.
2 Senior Consultant Physician, Department of Medicine, No. (2) Defence Services General Hospital, Myanmar.
3 Associate Professor and Consultant Neuro Physician, Department of Medicine, No. (1) Defence Services General Hospital, Myanmar.
4 Senior Consultant Physician/Nephrologist, Department of Medicine, No. (2) Defence Services General Hospital, Myanmar.
5 Senior Consultant Physician, Department of Medicine, No. (1) Defence Services General Hospital, Myanmar.
6 Dip. Med. Ed, Lecturer, Department of Chest Medicine, Defence Services Medical Academy, Myanmar.
7 Assistant Lecturer, Department of Medicine, Defence Services Medical Academy, Myanmar.
8 Assistant Lecturer/Haematologist, Department of Medicine, Defence Services Medical Academy, Myanmar.
9 Assistant Lecturer, Department of Medicine, Defence Services Medical Academy, Myanmar.
*Corresponding Author: Khin Phyu Pyar, Professor and Head/Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy, No. (1) Defence Services General Hospital, Myanmar.
Citation: Khin P Pyar, Sai A Hla, W Myint, Win K Shwe, Soe W Hlaing. (2022). Intractable/ Persistent Hiccups Due to Acute Subdural Haemorrhage as a Result of Prolonged Inr in a 55 Year Old Man with Rheumatic Mitral Valvular Heart Disease and Atrial Fibrillation: A Case Report. Biomedical Research and Clinical Reviews. 6(1); DOI: 10.31579/2692-9406/089
Copyright: © 2022 Khin Phyu Pyar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 October 2021 | Accepted: 28 December 2021 | Published: 10 January 2022
Keywords: coma; headache; acute subdural haemorrhage; rheumatic mitral valve disease; atrial fibrillation; warfarin; INR; intractable hiccups; burr hole surgery
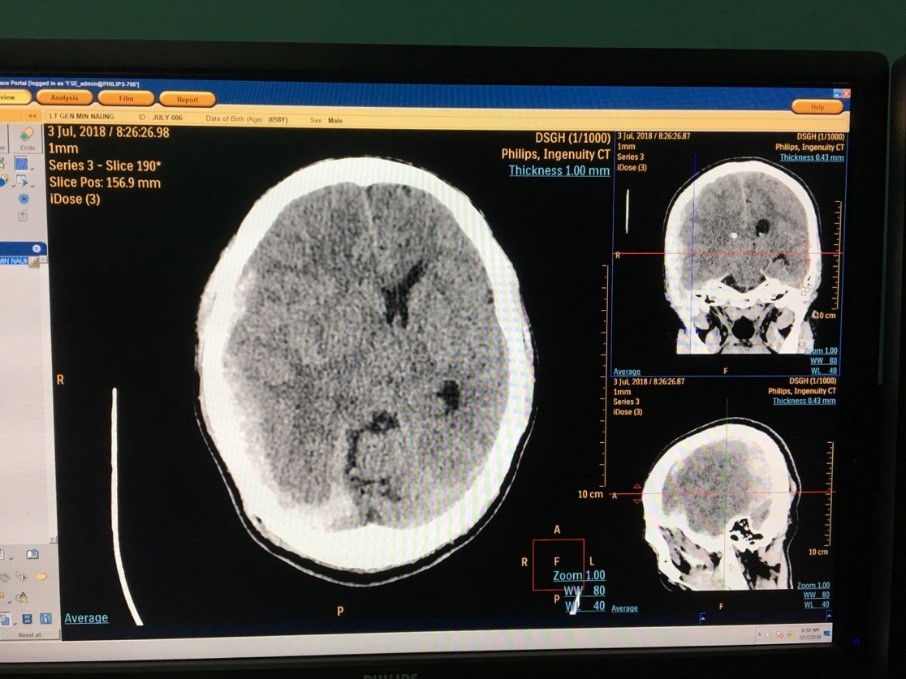
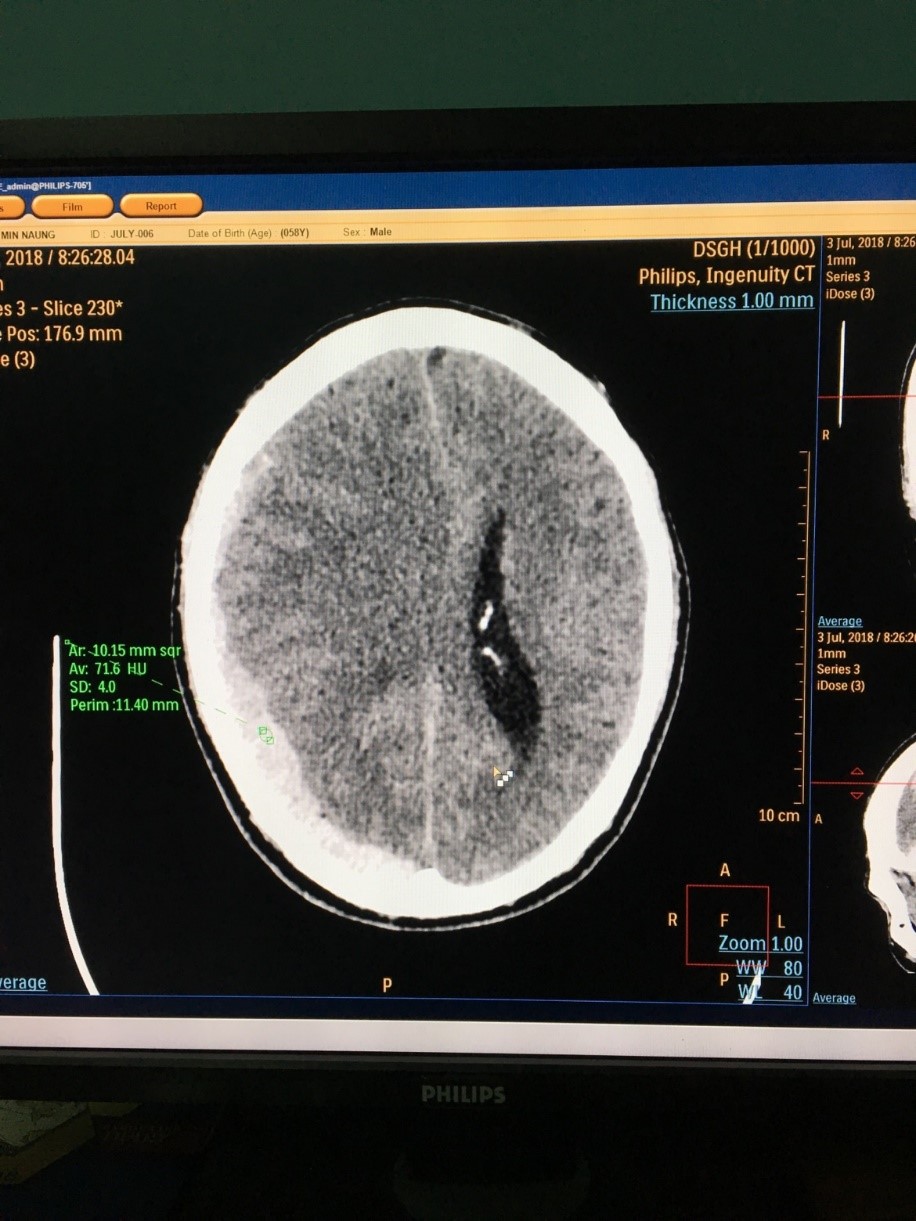
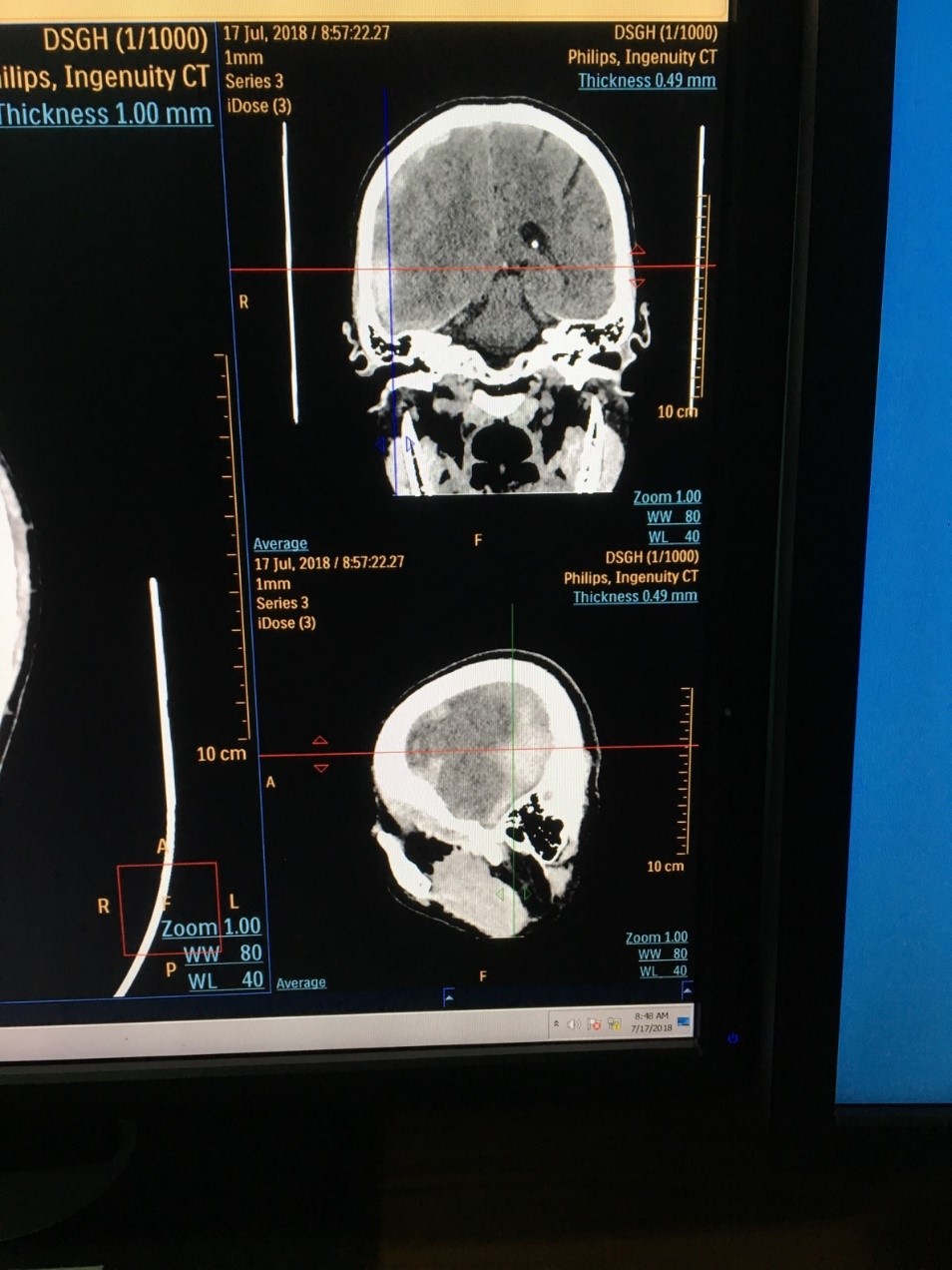
A 58 year old man was brought to hospital in state of deep coma following severe headache for one day. His GCS was 3/15 and had flaccid all 4 limbs with equivocal planter response on both sides on arrival. NECT head showed acute subdural haemorrhage with surrounding cerebral oedema, mid-line shift and corning of brain stem. After giving mannitol and dexamethasone, four hours later, he became fully conscious and orientated; his motor power returned to normal. He was on warfarin 3mg daily for rheumatic mitral valvular heart disease with atrial fibrillation and his INR on arrival was 3.5. He had intractable hiccups once he regained consciousness. Both pharmacological and non-pharmacological measures were tried for distressing hiccups; there was no therapeutic success. His hiccups disappeared completely only after removing the haematoma by burr hole surgery.
Hiccups is caused by involuntary contraction of diaphragm followed by the rapid closure of vocal cords. Though most of the people experience hiccups from time to time; they usually resolve without treatment within few minutes. If a bout lasts more than 48 hours; it is generally considered as persistent hiccup. And if it is longer than one month; it becomes intractable one. Intractable hiccups may result from many etiologies: structural or functional disturbances at medulla; afferent nerves or efferent nerves to the respiratory muscles; metabolic disorder; endocrine disorder; drugs; general anesthesia and emotional problems. Thus; several reports mentioned structural lesion near medulla producing persistent hiccups; aneurysm; haemorrhage or benign tumor (Musumeci et al.; 2000) (Nagayama et al.; 2004) (Li et al.; 2000) (Hatae et al.; 2014) (Gambhir et al.; 2010) (Chon et al.; 2020) (Al Deeb et al.; 1991). However; one report mentioned supratentorial lesion- chronic subdural haematoma; far away from medulla; may give rise to hiccups (Takemoto et al.; 2015).
One of the fatal side effects of warfarin is haemorrhage in the brain: intracerebral haemorrhage; cerebellar haemorrhage and subdural haemorrhage; and the mortality rate is very high. Several reports mentioned both pharmacological treatment (Lee et al.; 2010) (McGrane et al.; 2015); surgery (Tariq et al.; 2021) and non-pharmacological treatment for intractable hiccup. Among them; one patient with chronic subdural haematoma; intractable hiccups disappeared completely after surgical removal of haematoma (Takemoto et al.; 2015).
A 58 year old gentleman had severe headache for one day and was found unconscious in bed when his colleagues tried to wake him up in the morning. He vomited twice on the way to hospital. He was known to have rheumatic mitral valvular heart disease (mitral stenosis and mitral regurgitation) with atrial fibrillation and he was on warfarin 3mg OD; penicillin V 500 mg BD; digoxin 0.5 mg OD; telmisartan 20 mg OD and frusemide 20 mg OD cm alternate day.His previous INR were varied between 2 to 3; but it was never above 3.However; he did not check INR for 3 weeks as he was busy. There was no history of fever or head injury.
On arrival; his Glasgow Coma Scale was 3/15 and had flaccid all 4 limbs with equivocal planter response on both sides. He was afebrile; his SaO2 was 95% on air; his blood pressure was 140/90 mmHg; and his pulse rate 62/min with irregularly irregular in character. He had both pansystolic murmur and mid diastolic murmur in mitral area and there was no features of heart failure or infective endocarditis.
NECT head showed acute subdural haemorrhage with surrounding cerebral oedema; mid-line shift and corning of brain stem. (Figure 1) Four hours later; after giving mannitol and dexamethasone; he became fully conscious and orientated. Motor power returned to normal. His INR on arrival was 3.5. Therefore; the rapid reversal of anticoagulation was done; warfarin was withheld; and parenteral vitamin K 10 mg was given.The coagulation status became normal after infusion of fresh frozen plasma and 10 mg vitamin K replacement.Haemostatic agent (tranxenamic acid) was given too. Twenty-four hour after rapid reversal of anti-coagulation; the patient did not suffer headache and clinical signs of raised intracranial pressure (blood pressure and heart rate) settled down. He had intractable hiccups once he regained consciousness.
Blood for complete picture (Haemoglobin 12.5 gm%; Total WBC 7.0X109/L; neutrophil 75%; lymphocyte 22%; monocyte 3%; plateleta 350X109/L); blood urea and electrolytes; random blood sugar; blood cholesterol and liver function tests were normal. Blood culture was sterile. ECG revealed absent “p” wave; varying R-R interval with right ventricular hypertrophy. Chest radiograph showed mild cardiomegaly. In echocardiogram; there was no clot in left atrium and mitral valve orifice was 4 mm2 with some calcification.
We had to try for the best for both; prevention of clot in left atrium and cessation of further bleed in the brain. He received 20 mg enoxaparin subcutaneously 10 hours after the operation; and afterward at least 40 mg enoxaparin was administered daily for thromboembolism prophylaxis.
Hiccups was disturbing his eating and drinking: even he could not sleep. Various pharmacological (diazepan; metoclopramide; haloperidol) and non-pharmacological measures (drinking ice water; application of ice pad; breath holding; distraction of attention; Valsalva maneuver) were tried but to no evil.
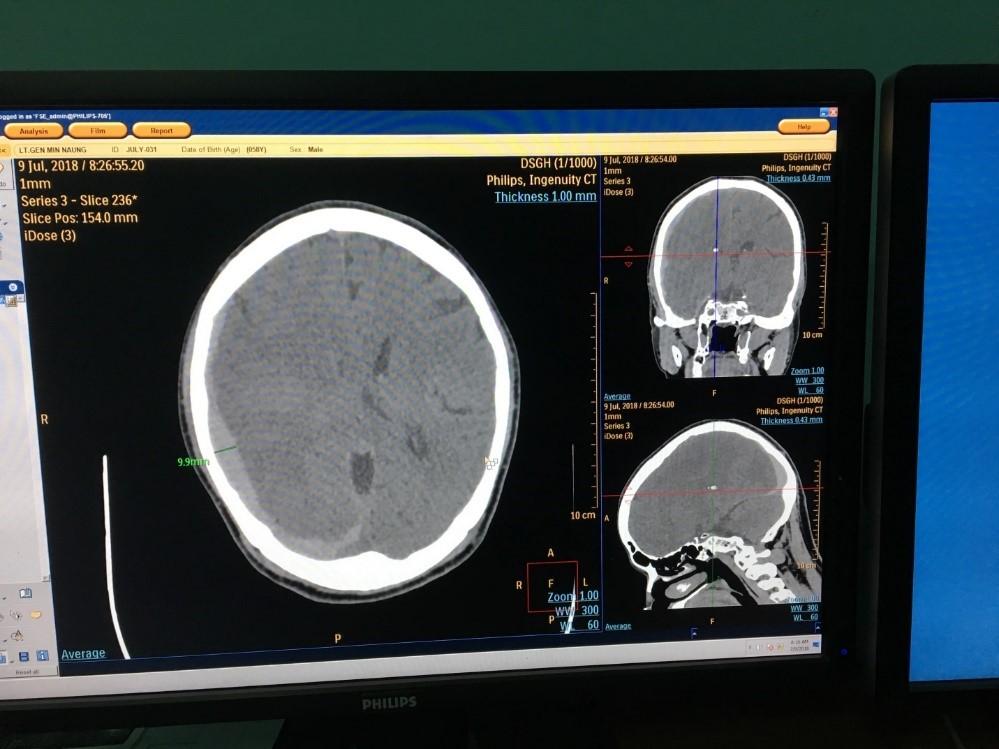
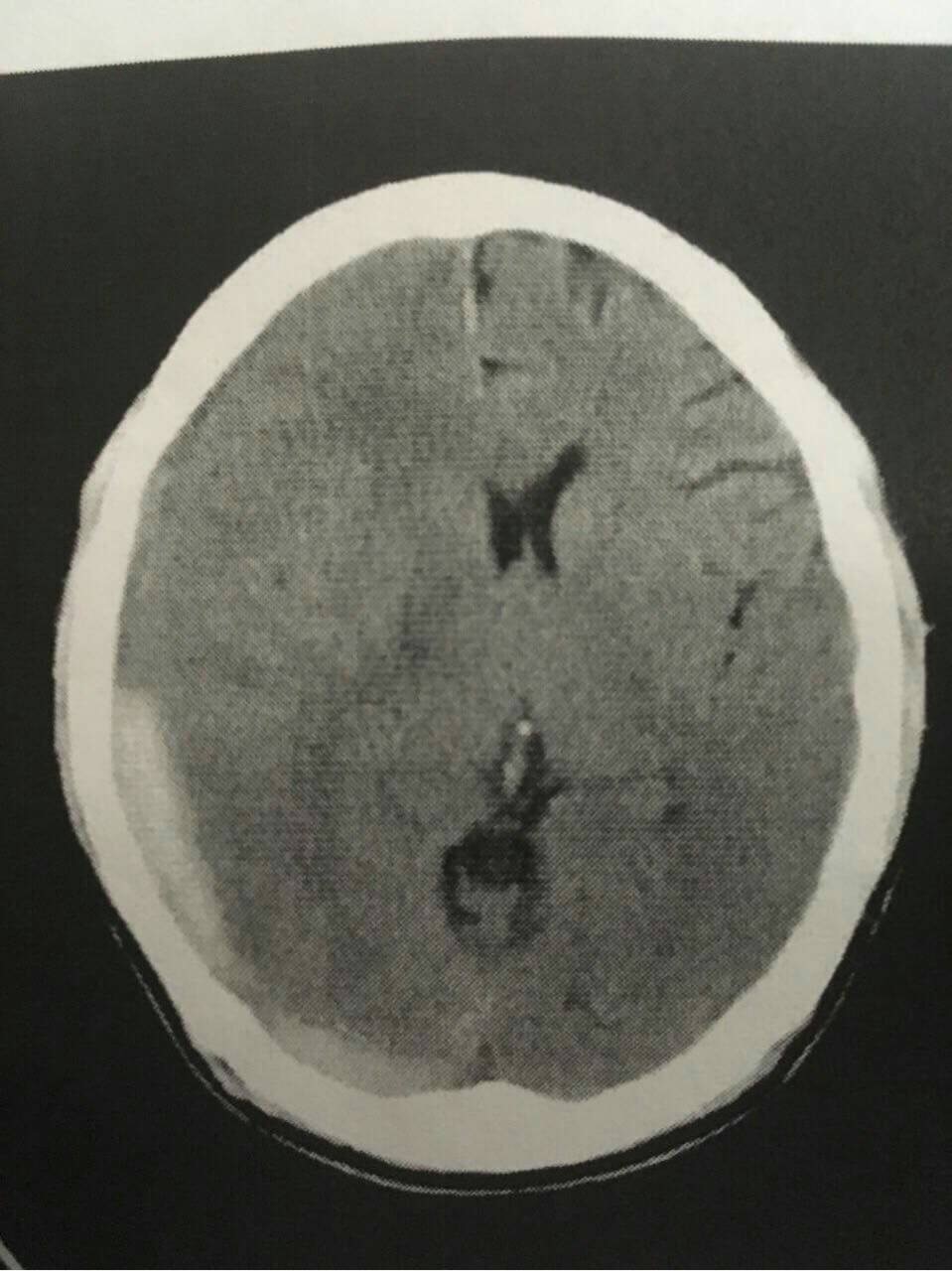
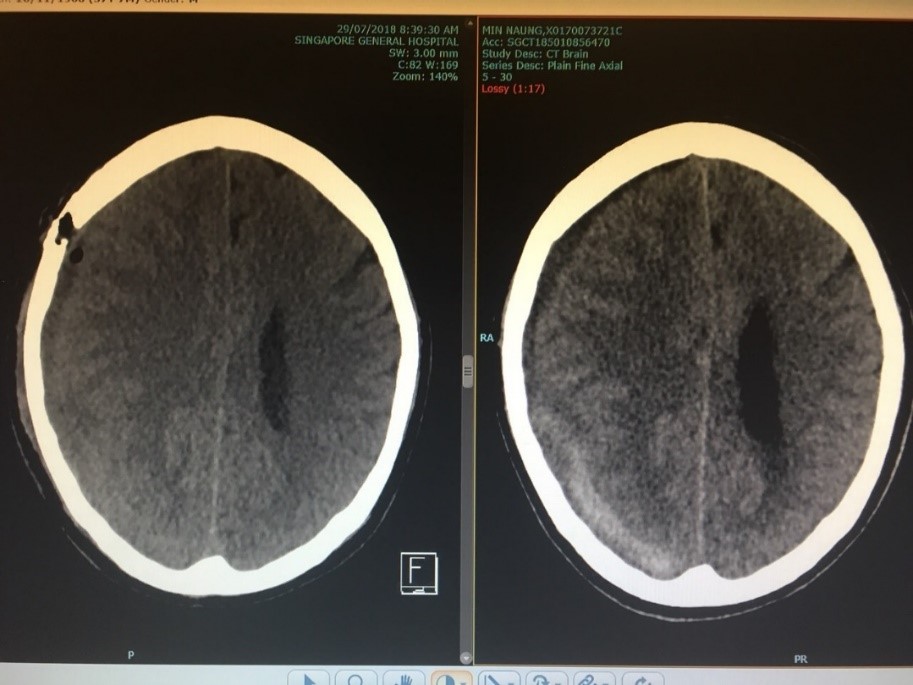
He was completely free of hiccups only after evacuation of blood by burr hole. CT head after evacuation showed reduction in volume of haematoma and resolution of cerebral oedema. And there was no mid-line shift. (Figure 2) The post-operative period was uneventful.
We planned for mitral valve replacement for his underlying mitral stenosis and mitral regurgitation and advised to continue penicillin for prevention of further rheumatic activity. We remind the patient not to miss “the warfarin clinic” again.

Hiccups was well known for one of the features of lateral medullary syndrome and there were several case reports on it (Sampath et al.; 2014). And the structural abnormalities near the medulla leading to intractable hiccups was also reported in some cases having vascular or tumor lesions close to medulla (Musumeci et al.; 2000)(Nagayama et al.; 2004)(Li et al.; 2000)(Hatae et al.; 2014)(Gambhir et al.; 2010)(Chon et al.; 2020)(Al Deeb et al.; 1991).
However; hiccups was seen as one of presenting symptoms in a case with chronic subdural haematoma and the patient was free of symptom after evacuation of blood (Takemoto et al.; 2015).Thus; it is possible that supratentorial areas involve in the either stimulation or suppression of the hiccups centers though these areas are far away from medulla. None of the report explained about distressing hiccups in acute subdural haematoma. Thus; it was the main reason for presenting this case.
Moreover; the role of warfarin was essential in this case to prevent thrombus formation in left atrium though it was not seen in transthoracic echocardiogram. On the other hand; limitation of further expansion of acute subdural haemorrhage was paramount importance for neurological sequelae. Thus; appropriate timing for evacuation of haematoma with minimum bleeding risks was also the art of medicine. It was another reason to share our knowledge. Lin et al (2017) pointed out that the mortality rate of patients with acute subdural haematoma already on long warfarin therapy was nearly double than those who were not on warfarin. Thus; this case was one of the rare cases.
Furthermore; after surgery; monitoring for prevention of rebleeding was very delicate as many case reports mentioned high rebleeding risks (Gonugunta & Buxton; 2001). Restarting warfarin therapy was done 2 weeks after burr hole surgery. He has no evidence of rebleed till now- 18 months after surgery.
Health education - “importance of warfarin clinic” was extremely crucial as missing one appointment led to torrential fatal event.
Both prevention of thromboembolism in high risks patient- atrial fibrillation in mitral valve disease with anti-coagulation and retardation of extension of acute subdural haemorrhage are difficult therapeutic dilemma in this patient. Initially; rapid reversal of anti-coagulation saved the life. Timing and preparation for evacuation of haematoma is critical. After evacuation; prevention of rebleeding is also important. However; the main concerned from patient point ie the most distressing symptom was persistent hiccups which disappeared completely after surgery.
The authors would like to thank the patient for giving consent to this article. Also; to all doctors and nursing team for making great efforts in caring him. The authors acknowledged the following team; cardiac medical team – Dr Win Thaw; neuro surgical team - Dr Thant Lwynn San; intensive care team - Prof Yu Aye Latt; Dr Chan Myae & Dr Nay Myo Lwin; Laboratory team – Professor Tin Moe Mya; radiological team- Professor Kyaw Za Ya; administrative support - Prof Soe Win; Prof Soe Hlaing and Prof Myint Zaw.
Declaration of conflict of interest
The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting cases.
Funding
The authors received no financial support for publication of this article.
Informed consent
The informed consent for publication in this article was obtained from patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
