
Case Report | DOI: https://doi.org/10.31579/2690-4861/316
1 Gilbert and Rose-Marie Chagoury School of Medicine, Lebanese American University, Beirut, Lebanon.
2 Department of Medicine, Hospital Louis Mourier, Assistance Publique des Hôpitaux de Paris, Colombes, France.
3 Department of Medicine, University of Florida, Gainesville, FL.
4 Department of Medicine, University of Massachusetts Chan Medical School, MA.
*Corresponding Author: Andreas Filippaios, Department of Medicine, University of Massachusetts Chan Medical School, MA.
Citation: Fady E. Tom, Skaff Y., Melissa B. Malham, Mehawej J., Filippaios A., (2023), Intracranial Hypotension and Bilateral Isolated Cortical Vein Thrombosis: A Case Report and Literature Review, International Journal of Clinical Case Reports and Reviews, 14(1); DOI:10.31579/2690-4861/316
Copyright: © 2023, Andreas Filippaios. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 June 2023 | Accepted: 23 June 2023 | Published: 30 June 2023
Keywords: intracranial hypotension; isolated cortical venous thrombosis; cerebrospinal fluid; case report
Background: Intracranial hypotension (IH) is a clinical manifestation of low cerebrospinal fluid pressure with reports of isolated cortical venous thrombosis (ICVT) rarely described.
Case Presentation: A 23-year-old man presented with postural headache followed by blurry vision and horizontal binocular diplopia with extreme gaze. Patient workup showed diffuse thickening and enhancement of the dura suggestive of intracranial hypotension and biparietal superficial cortical vein thrombosis was noted on imaging. The patient was started on folate and therapeutic anticoagulation and his condition improved.
Conclusion: Patients with IH are at risk for CVT due to the dilation of the venous sinuses of the brain. Changes in the characteristics of the headache of the patient or the onset of new neurological symptoms should warrant further investigation. Prophylactic systemic anticoagulation might cautiously be indicated in high-risk patients with IH to prevent ICVT.
Intracranial Hypotension (IH), also known as low cerebrospinal fluid (CSF) pressure syndrome, is a rare condition that occurs when the pressure of the cerebrospinal fluid that surrounds the brain and spinal cord within the subarachnoid space decreases below 60 mm H2O [1]. IH manifests as a characteristic postural headache that worsens with upright positioning and improves while laying supine. In some cases, intracranial hypotension can also cause vision disturbances, tinnitus, and cognitive impairments [2]. Intracranial hypotension can lead to the formation of brain herniation [4], and in rare cases, it has been reported to cause intracranial cortical vein thrombosis (CVT), thought to be due to the dilation of the venous sinuses of the brain [5].
The frequency of CVT among patients with IH is documented to be around 2% which is significantly higher than the rate of 0.0005% in the general population. Even though CVT is known to be associated with multiple predisposing factors and comorbidities, little is known about the onset of CVT in IH; some mechanisms however have been postulated in the literature. CVT can result in intracranial hemorrhage, venous infarction, vasogenic edema, transtentorial herniation and even death in 3% of cases.
In the following, we report a rare case of IH complicated by CVT. In addition, we will report its pathogenesis and treatment. Reporting this complication of IH can enable prompt diagnosis and highlight the importance of early treatment.
A 23-year-old man presented with a severe headache radiating to his neck of 4 days duration and a high-grade fever of 1 day duration. The headaches were diffuse, throbbing in nature, and exacerbated by movement, standing up, and taking the stairs. The patient also reported occasional photophobia and nausea. He also noted a mild neck rigidity when the headaches were at their worst in addition to a burning pain sensation behind the eyes bilaterally. He started having febrile episodes 1 day prior to presentation with a maximum temperature reaching 39.5°C rectally and responding to antipyretics. The headaches were poorly refractory to analgesics and NSAIDs. The patient denied any previous history of headaches or migraines.
The patient’s past medical history was notable for essential tremor for which he takes propranolol 10mg once daily. He is a non-smoker, non-alcoholic, not sexually active, and no history of recent travels, hikes, or sick contacts.
On physical examination, the patient’s vital signs on admission were as follows: temperature was 37.8°C, respiratory rate was 18 breaths/min, heart rate was 100 beats/min, blood pressure was 127/75 mmHg, and oxygen saturation was 100% on room air. The patient was ill-appearing. Neurological exam was clear with 5/5 motor function and no neck rigidity. Cardiopulmonary auscultation was clear and within normal limits. Abdominal examination was unremarkable for guarding, distention, or rigidity. No genitourinary findings were reported. Peripheral pulses were positive, no skin manifestations were detected, and no edema was noted peripherally.
His initial workup upon admission is reported in Table 1 and showed an elevated CRP of 1.6 mg/dL and a mild normocytic anemia. His WBC count and differentials were within normal ranges. His urinalysis was normal. His blood culture was negative. A lumbar puncture was performed, and CSF analysis reported a mild elevation in WBC (10/mm3) and RBC (5/mm3), but the proteins and glucose levels were within normal limits (19 mg/dL and 69 mg/dL respectively). The patient had done a Brain CT one day prior to presentation which was normal and a COVID-19 PCR which was negative. As per infectious control protocol, he was scheduled for a chest X-Ray which also came back normal.
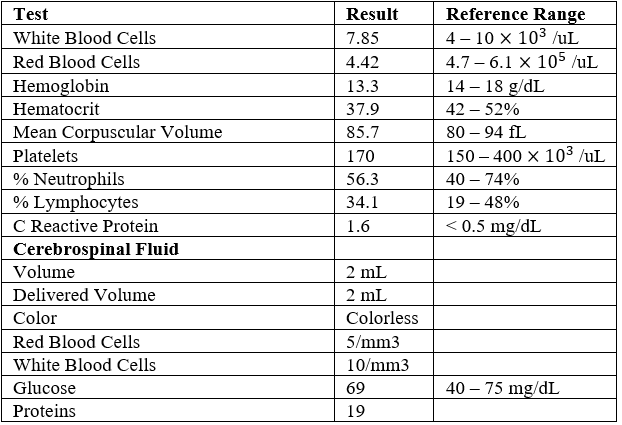
Table 1: Patient’s blood workup and CSF analysis on the day of presentation
On day 1 of admission, the patient was still complaining from continuous headaches with minimal response to analgesics and his vital signs reported some febrile episodes with his temperature reaching 38.3°C. He was empirically started on ceftriaxone 2g IV daily despite the negative CSF findings. The patient also noted that his headaches had changed in character with a new component of orthostatic pain that had set in. Brain MRI with contrast and Brain MRV (Figure 1) were performed to rule out a venous sinus thrombosis and/or CSF leak from his previous LP. MRI showed no acute intracranial process or abnormal parenchymal, leptomeningeal or parchymeningeal enhancement. MRV was also unremarkable. IV hydration was increased appropriately, and IV pethidine was added to his pain management.
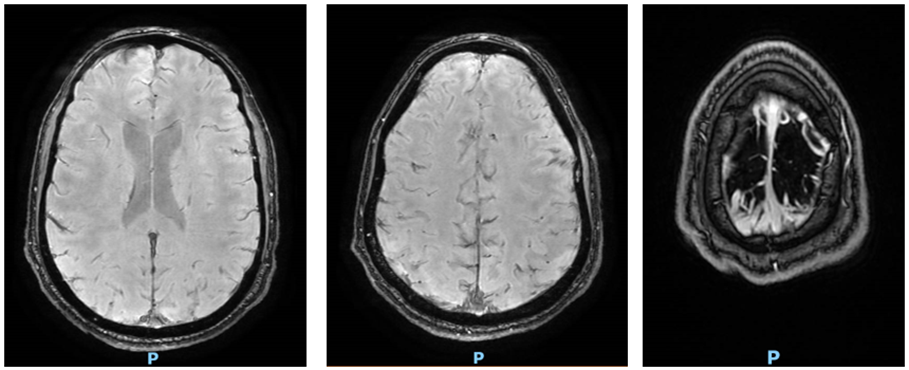
Figure 1: MRI of the Brain on Day 1 of admission.
Figures 1A and 1B are Axial SWAN sequences and Figure 1C is an Axial FSPGR + BRAVO Sequence.
On day 2 of admission, the patient reported the same continuous pain which led to 3 episodes of vomiting that morning. He was afebrile, on complete bed rest, and in supine position for his possible CSF leak. Infectious prodrome was suspected, speculating aseptic viral meningitis/encephalitis. Infectious workup was inconclusive. Influenza A/B and Adenovirus PCRs were negative. Wright test was negative for brucellosis and Widal test was ordered for typhoid fever.
On day 3 of admission, the patient was discharged home after improvement of his symptoms.
On day 10 of symptoms, the patient presented to the ophthalmology clinic for severe right eye pain worsening on movement of the eyeball and associated with blurry vision. Complete ophthalmologic and neurologic exam were done and were unremarkable. Patient was advised to continue his extensive hydration regimen with caffeine supplementation for his potential CSF leak which could be at the origin of his symptoms.
On day 11 of symptoms, the patient presented to the hospital for a new onset of double vision. Neurologic exam was done, and he was found to have horizontal binocular diplopia with extreme gaze, more pronounced on the right than the left. He did not have any ophthalmoplegia and denied any associated symptoms. His labs were normal (Table 2); WBC count, liver enzymes and CRP levels were within normal ranges. He was scheduled for a Brain MRI and MRV with Injection (Figure 2). He was found to have diffuse thickening and enhancement of the dura suggestive of intracranial hypotension, along with prominence of the CSF fluid surrounding the optic nerves when compared to the previous examination of a week ago. In addition, he was found to have blooming artifacts noted within the biparietal superficial cortical veins seen on SWAN and FSPGR sequences which, when correlated with the MRV, suggest a biparietal superficial cortical vein thrombosis.
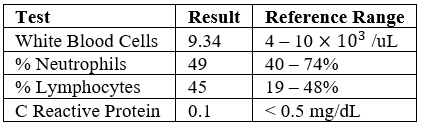
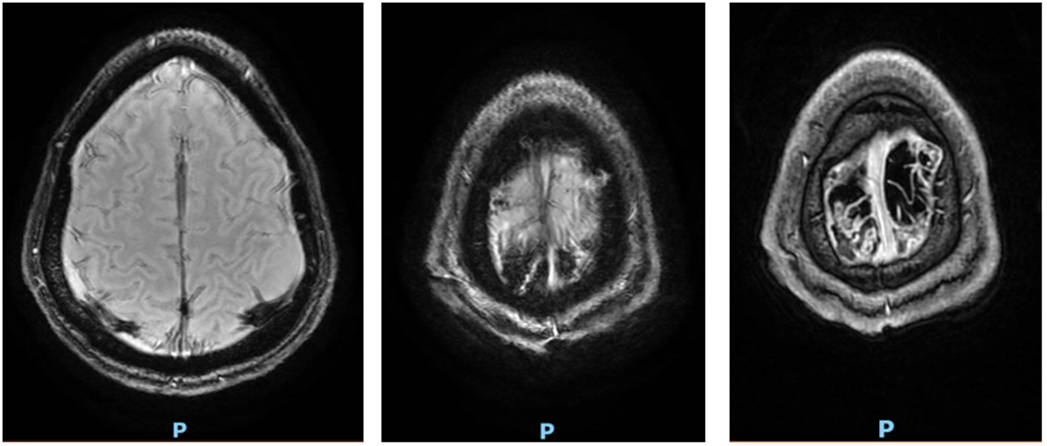
Figure 2: Patient's brain MRI and MRV on his 2nd admission revealing the biparietal filling defect of the superficial cortical veins.
Figures 2A and 2B are Axial SWAN sequences and Figure 2C is an Axial FSPGR + BRAVO Sequence.
When questioned, the patient reported a paternal family history of coagulopathies. He was started on Rivaroxaban 15 mg twice daily for 3 weeks and then 20 mg once daily for 1 year. The patient reported immediate improvement of his symptoms as of the first day of Rivaroxaban therapy.
On day 6 of Rivaroxaban therapy, a repeat MRI and MRV of the brain were ordered (Figure 3). The results showed an interval decrease in the blooming artifact and filling defect seen within the biparietal superficial cortical veins previously seen on SWAN and MRV, in addition to a complete resolution of the diffuse thickening and enhancement of the dura suggesting resolved intracranial hypotension.

Figure 3: Patient's MRI and MRV on Day 6 of anticoagulation therapy revealing an interval decrease in the blooming artifacts.
Figures 3A and 3B are Axial SWAN sequences and Figure 3C is an Axial FSPGR + BRAVO Sequence.
A blood coagulation panel was taken before the patient started his anticoagulation therapy and his results are illustrated in Table 3. A genetic panel of thrombotic risk was also ordered (Table 4) and came back positive for a homozygous A1298C mutation of the methylene-tetrahydrofolate reductase (MTHFR). Because of his borderline homocysteine levels and in-line with his homozygous MTHFR mutation, the patient was started on folate supplementation of 5mg once daily.

Table 3: Blood coagulation panel results of the patient before initiating his treatment of rivaroxaban and folate supplementation, as compared to 3 months after starting treatment.
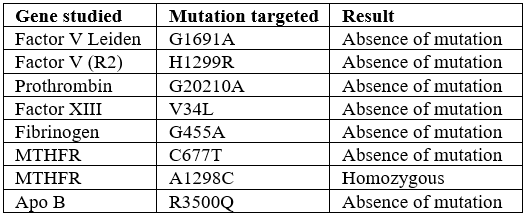
Table 4: Patient’s genetic panel results of thrombotic risk.
Three months after initiating the Rivaroxaban and folate therapy, a repeat MRI and MRV (Figure 4) showed an interval near complete resolution of the previously seen dural venous thrombi within the biparietal superficial cortical veins posteriorly, with a small residual non-occlusive thrombus at the left posterosuperior parietal cortical vein. A repeat blood coagulation panel was conducted and showed an interval decrease in the homocysteine levels with elevated protein C and S levels (Table 3).

Figure 4: Patient's repeat MRI and MRV 3 months after initiating treatment showing an interval almost complete resolution of the blooming artifacts indicative of the superficial cortical venous occlusions.
Figures 4A and 4B are Axial SWAN sequences and Figure 4C is an Axial FSPGR + BRAVO Sequence.
The patient is scheduled to have a control brain MRI and MRV one year after initiating the rivaroxaban therapy to determine if he would be eligible to discontinue his anticoagulation regimen or not.
We describe a case of isolated cortical vein thrombosis (ICVT) post lumbar puncture intracranial hypotension that presented with postural headache followed by blurry vision and horizontal binocular diplopia with extreme gaze.
CVT is a cerebrovascular disease that, contrary to arterial stroke, affects most commonly young adults and children with an annual prevalence of 3 to 4 cases per 1 million population and 7 cases per 1 million in children [7]. Women represent around 75 percent of the adult population, despite sex difference minimizing in patients older than 60 [8]. CVT is caused by the partial or total obstruction of the major cerebral venous sinuses or the tinnier nourishing cortical veins causing cerebral venous sinus thrombosis and cortical vein thrombosis respectively [9].
Several factors influence the presentation of the patient: the position and degree of thrombosis, extent of collateral venous system nearby the thrombosis, and existence of cortical lesions correlated [10]. Thrombosis of a solitary cortical vein might lead to focal sensory or motor deficits, while an extended thrombus in a great venous sinus will cause more general neurological symptomatology which involve headache, seizure, altered consciousness and signs of increased intracranial pressure [11]. This cerebrovascular disease can present as a single symptom or manifest as a syndrome made of several symptoms, all of which are unspecific, which makes diagnosing CVT challenging [12].
The pathogenesis of CVT caused by lumbar puncture can be justified by the Monro-Kellie hypothesis, namely the total amount of brain volume, CSF and intracranial blood is constant. Any change in one of the components will affect the other two by increasing or decreasing it [13]. In the case of lumbar puncture, when the CSF hypotension happens, the CSF volume and pressure remarkably decrease. Consequently, there will be increase in intracranial blood, mostly in the venous system at the detriment of stasis and distension of venous sinuses and cortical veins in the dura. These changes happen abruptly in the dura mater made of rough fibrous meninges that has no blood brain barrier which explains the extravasation on imaging [14]. Moreover, with the reduced CSF volume the brain as a whole will be relatively pulled, in addition to the dilation of the dural and cortical veins. All these modifications will ultimately affect the vascular wall. The described phenomenon abides by the Virchow criteria according to which the core triggers for thrombosis would be blood stasis in addition to alterations in the vessel wall and blood structure [15-16].
As CVT is a rare complication of cerebral hypotension, we compiled sixteen cases of cerebral venous thrombosis associated with post-diagnostic lumbar puncture intracranial hypotension in non-obstetrical population (Table 5). Patients’ age range was between 17 and 49 years and the male/female ratio, 1:7. Five of these patients were previously healthy, five patients were on oral contraceptive pills, four patients had a heterozygous prothrombin G20210A mutation, two patients had Factor V Leiden mutation in addition to other comorbidities like idiopathic focal epilepsy, optic neuritis, and lymphoblastic leukemia. Our patient was found to have a homozygous MTHFR A1298C mutation. Thirteen out of the sixteen cases had postural headache and ten of them had a change in the headache pattern. From the beginning of symptoms to diagnosis, the average time was 4.2 days in these cases. In our case, it was 7 days. The most common location of CVT was in the superior sagittal sinus while our patient presented a biparietal superficial cortical vein thrombosis. Good response to treatment was by anticoagulation +/- epidural blood patch.
Reference
| Age/ Sex | Comorbidities | Postural headache | Change in the headache pattern | Time to diagnosis | Imaging findings
| Treatment
| Response |
| Wilder-Smith et al, 1997 | 26/ F | Factor V Leiden mutation, oral contraceptive pill intake | Yes | Yes | 3 days | Superior sagittal sinus | Anticoagulation | Good |
| Aidi et al, 1999 | 30/ F | None | Yes | Yes | 2 days | Superior sagittal sinus, lateral sinus | Anticoagulation | Good |
| Aidi et al, 1999 | 36/ F | None | Yes | Yes | 3 days | Superior sagittal sinus | Anticoagulation | Good |
| Giorgetti et al, 2001 | 34/ F | None | Yes | Yes | 8 days | Superior sagittal sinus, transverse sinus, sigmoid sinus | Anticoagulation | Good |
| Mouraux et al 2002 | 35/ F | None | Yes | No | 2 days | Anticoagulation | Good | |
| Benzon et al, 2003 | 32/ M | Lymphoblastic leukemia | Yes | No | Anticoagulation, Epidural blood patch | Good | ||
| Vandenberghe et al, 2003 | 23/ F | Oral contraceptive pill intake | 6 days | Superior sagittal sinus, lateral sinus, straight sinus | Poor | |||
| Vandenberghe et al, 2003 | 19/ F | Oral contraceptive pill intake | 9 days | Superior sagittal sinus | Good | |||
| Pfeilschifter et al, 2009 | 49/ F | Protein S & heterozygous Factor V Leiden Mutation | Yes | No | 5 days | Superior sagittal sinus, vein of Trolard | Anticoagulation, Decompressive surgery | Poor |
| Ferrante et al, 2009 | 19/ F | Oral contraceptive pill intake | Yes | Yes | Few days | Lateral sinus | Anticoagulation | Good |
| Casado-Menendez et al, 2011 | 44/ F | None | Yes | Yes | 3 days | Superior sagittal sinus, cortical vein | Anticoagulation | Good |
| Sánchez et al, 2014 | 20/ M | Heterozygous prothrombin G20210A mutation | Yes | Yes | 5 days | Superior sagittal sinus | Anticoagulation | Good |
| Michel et al, 2015 | 17/ F | Idiopathic focal epilepsy, Heterozygous prothrombin G20210A mutation, high lipoprotein A serum level | No | No | 4 days | Superior sagittal sinus | Anticoagulation | Good |
| Edwards et al, 2020 | 32/ F | Optic neuritis, Iron deficiency anemia | Yes | Yes | 5 days | Right parietal cortical vein | Anticoagulation | Good |
| Kannarkat et al, 2021 | 33/ F | Heterozygous prothrombin G20210A mutation | Yes | Yes | 1 day | Anticoagulation, Epidural blood patch | Good | |
| Kannarkat et al, 2021 | 17/ F | Heterozygous prothrombin G20210A mutation, Oral contraceptive pill intake | Yes | Yes | 3 days | Superior sagittal sinus and left cortical veins | Anticoagulation | Good |
Table 5: Review of literature of cerebral venous thrombosis associated with post-diagnostic lumbar puncture intracranial hypotension in non-obstetrical population.
Most cases of IH resolve spontaneously with increased hydration and excessive caffeine administration [17]. However, if conservative measures fail to improve symptoms, there are several treatment options available. The most common treatment is an epidural blood patch, which can provide relief for around one-third of patients and can be repeated if necessary. Other options include percutaneous placement of fibrin sealant and surgical repair, but these treatments require pinpointing the precise location of the CSF leak [18].
The primary goal of managing CVT is to restore the flow of the occluded vessel and prevent expansion to other parts of the venous system [19]. This objective can be achieved by administering anticoagulation therapy, with low molecular weight heparin (LMWH) being typically the preferred drug. However, LMWH and heparin are contraindicated in patients with recent cerebral hemorrhage, severe hypertensive episodes, hemorrhagic disorders, or peptic ulcer disease. Additionally, LMWH products should be administered cautiously in patients with chronic kidney disease. In such cases, heparin may be a more suitable alternative [20]. Recent evidences also recommend the initiation of direct oral anticoagulants (DOACs) such as factor Xa inhibitors like rivaroxaban in the outpatient setting for easier oral administration compared to the subcutaneous injections of LMWH [21].
Neurosurgery consultation and decompressive craniectomy or hemicraniectomy should be considered for patients with evidence of cerebral herniation. Mechanical thrombectomy or endovascular thrombolysis may also be an option for patients with worsening neurological symptoms despite adequate systemic anticoagulation.
ICVT poses a risk of increased intracranial pressure, and patients should be admitted to neuro-intensive care for frequent ICP monitoring. Additional measures such as elevating the head of the bed, administering osmotic agents like mannitol or hypertonic saline, and allowing permissive hyperventilation may be necessary. Intravenous dexamethasone is not recommended for treating ICVT.
Seizure prophylaxis is essential for patients who present with seizures, edema, infarction, or hemorrhaging on imaging. Levetiracetam or valproate are the preferred first-line drugs. Following stabilization and discharge, anticoagulation therapy should be considered for at least three months to prevent ICVT recurrence [23].
Intracranial hypotension is a common complication of iatrogenic procedures involving a dural puncture. Patients with IH may be at risk for ICVT due to the increase in the blood flow to the brain to compensate for the CSF loss. Any changes in the characteristics of the headache of the patient, or the onset of new neurological symptoms should warrant further investigations of possible ICVT in the setting of IH. Prophylactic systemic anticoagulation might cautiously be indicated in high-risk patients with IH to prevent ICVT.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper
Dr. Filippaios’s time was supported by NIH grant 2T32HL120823
A special thank you to the patient for allowing disclosure of his medical history.
Fady El Tom: Writing - original draft, Writing - review & editing.
Yara Skaff: Writing - original draft, Writing - review & editing.
Melissa Bou Malham: Writing - original draft, Writing - review & editing.
Jordy Mehawej: Supervision, Writing - original draft, Writing - review & editing.
Andreas Filippaios: Supervision, Writing - original draft, Writing - review & editing.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
