
Research Article | DOI: https://doi.org/10.31579/2578-8868/214
1 Endovascular Therapy Fellowship, Universidad Nacional Autonoma de Mexico, Instituto Nacional de Neurología y Neurocirugía Manuel Velasco (INNN)
2 Neuroradiology, Endovascular Therapy, Universidad Nacional Autonoma de Mexico, Instituto Nacional de Neurología y Neurocirugía Manuel Velasco (INNN)
3 Department of Endovascular Therapy, Universidad Nacional Autonoma de Mexico, Instituto Nacional de Neurologia y Neurocirugia Manuel Velasco (INNN)
4 Neuroradiology Fellowship, Universidad Nacional Autonoma de Mexico, Instituto Nacional de Neurología y Neurocirugía Manuel Velasco (INNN)
*Corresponding Author: Cindy Díaz, Unit, Endovascular Therapy Fellowship, Universidad Nacional Autonoma de Mexico, Instituto Nacional de Neurología y Neurocirugía Manuel Velasco (INNN)
Citation: Cindy Díaz, Alfredo Montenegro, Jorge Balderrama, Alba Herrera (2021). Intracranial Atherosclerotic Stenosis: An Up-to-Date Review. J. Neuroscience and Neurological Surgery. 9(5); DOI:10.31579/2578-8868/214
Copyright: © 2021 Cindy Díaz, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 19 October 2021 | Accepted: 01 November 2021 | Published: 08 November 2021
Keywords: intracranial atherosclerotic stenosis; cerebrovascular accident; ischemic stroke
In this review, we discuss recent clinical assays that have contributed to understanding the disease process associated with ICAD, risk factors associated with CVA recurrence in this subgroup of patients, imaging characteristics related to the prognosis, and an update on the treatments that reduce CVA recurrence.
ICAD: intracranial atherosclerotic disease
CVA: cerebrovascular accident
IS: ischemic stroke
TIA: transient ischemic attack
TCD: transcranial doppler
MCA: middle cerebral artery
MRA: magnetic resonance angiography
A-ICAS: asymptomatic intracranial atherosclerotic stenosis
S-ICAS: symptomatic intracranial atherosclerotic stenosis
CTA: computerized tomography angiography
DSA: digital subtraction angiography
HRMRI: high-resolution magnetic resonance imaging
ICA: internal carotid artery
AMT: aggressive medical treatment
PTAS: percutaneous transluminal angioplasty and stenting
PTA: percutaneous transluminal angioplasty
ICH: intracerebral hemorrhage
ACA: anterior cerebral artery
PCA: posterior cerebral artery
EICS: elective intracranial stenting
Cerebrovascular accidents (CVA) or strokes are one of the main mortality and morbidity causes around the world. Large-vessel atherosclerosis represents 20% of ischemic strokes (IS), 50% are intracranial, and it is associated with a high risk of recurrent CVA compared with other CVA subtypes, despite even the best medical care [1]. Intracranial atherosclerotic disease (ICAD) is one of the main causes of IS, representing almost 5-10% of intracranial atherosclerotic strokes in the USA, and up to 50% in Asia [2].
Materials and Methods
A search was made in the databases of PubMed (http: //www.ncbi.nlm.nih. Gov / PubMed / medline.html), OVID (http://www.ovid.com/), Ebsco (http : //www.ebsco.com) with the following terms: intracranial atherosclerotic disease, ischemic stroke, symptomatic intracranial atherosclerotic stenosis, medical treatment, endovascular treatment
Epidemiology
ICAD causes between 5 and 10% of IS in white people, between 20 and 30% of transient ischemic attacks (TIA) or CVA in black people, and up to 30 to 50% of CVA in Asian people (3)(4). From a total of 900,000 CVA or TIA that occur each year in the USA, approximately 70,000-90,000 are caused by intracranial atherosclerotic stenosis [3,5]. The risk of recurrent CVA in these patients could be as high as 15% per year [6,7], and on other studies in patients with high-grade S-ICAD (stenosis: 70-99%), up to 23% per year despite aggressive antithrombotic therapy and standard vascular risk factor management [8,9]. Due to this elevated recurrence rate, there are alternative therapeutic options for the prevention of recurrent CVA in patients with severe ICAD that do not respond to medical treatments such as balloon angioplasty or stent placement [9,10].
Risk Factors
Symptomatic and asymptomatic ICAD risk factors include:
-Age
-Race: Afro American, Hispanic, and Asian compared to white people. [4,11].
-Cardiovascular risk pathologies:
*High blood pressure: In the Warfarin Aspirin Symptomatic Intracranial Disease (WASID) study, the most important modifiable risk factor that increases the risk of recurrent CVA and cardiovascular events (acute myocardial infarction and vascular death) associated with ICAD is high blood pressure (Systolic arterial pressure ≥ 140 mm Hg, HR= 1.79, p = 0.0009) [12].
*Diabetes Mellitus: High levels of A1C hemoglobin are not correlated to the severity of the ICAD, but diabetes mellitus remains as an independent risk factor [13].
*Hyperlipidemia: Those that are associated to a higher risk of recurrent CVA and ICAD progression are: total cholesterol serum levels ≥ 200 mg/dl (WASID study: Warfarin Aspirin Symptomatic Intracranial Disease, HR= 1.44, p = 0.048) (5)(12), increase in the apolipoprotein B (apoB)/apolipoprotein A-I (apoAI) rate (TOSS-2 study: Trial of cilOstazol in Symptomatic intracranial Stenosis 2), decrease in serum levels of high-density lipoprotein cholesterol- HDL [14].
*Metabolic syndrome [15,16].
-Sedentary lifestyle and diet [17]
-Smoking [18].
-Morphological characteristics of the stenosis: The risk of CVA in the territory of the stenotic artery was higher in severe stenosis ≥ 70% (HR= 2.03, p = 0.0025) [19].
-Collateral circulation: The presence of good collaterality in patients with stenosis ≥ 70
Diagnostic tools used to identify ICAD include:
Non-invasive methods:
- Transcranial Doppler (TCD): It is superior when providing flow information in real time and evidencing the direction of flow, collaterality, embolization (microembolic signs are an independent predictor of recurrence of CVA in patients with S-ICAD), and steal phenomenon, compared with static CT and MRA images [31]. It is useful for the standardized exploration protocol of Stroke Outcomes and Neuroimaging of Intracranial Atherosclerosis (SONIA) criteria to identify stenosis ≥ 50% stenosis. The optimal combined criteria for stenosis ≥ 70% were MCA average velocity >120 cm/s, or a stenosis/pre-stenosis ratio ≥3, or average-low velocity. In vertebral artery/basilar artery it varies >110 cm/s or stenotic/prestenotic ratio ≥ 3 [32].
- Magnetic resonance angiography (MRA): TOF-MRA is a flow sequence, accentuating hemodynamic characteristics and, as such, it generally overestimates the grade of stenosis, especially in cases with low distal flow to the ICAD location. The advantage of this sequence is that it makes it possible to evaluate the hemodynamic impact of the lesion [33].
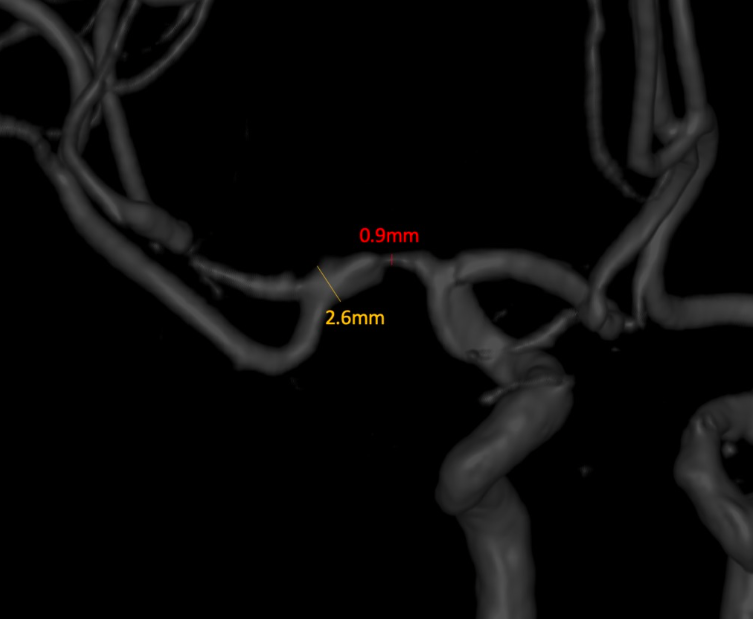
Measurement techniques like the WASID Measurement Technique have been developed. Two measurements for each intracranial ACI are taken: 1) a linear measurement at the location of the most severe stenosis in the images either the MIP or axial source images; and 2) a linear measurement of the widest normal, non-tortuous portion of the petrous ACI parallel to the location of the stenosis. Using these measurements, we calculated the WASID grade of stenosis using the following equation (Figure 1): Percentage of stenosis = [(1 - [D stenosis / D normal])] x 100, where D stenosis is the diameter of the artery at the location with the most severe grade of stenosis and D normal is the diameter of the proximal artery in its widest, non-tortuous normal segment [34].
Computerized tomography angiography (CTA): It provides a better delimitation of the anatomy of intracranial arteries, which allows for higher diagnostic precision of luminar stenosis in ICAD compared to the TCD and MRA, with a sensitivity >95% in the diagnosis of ICAD (35) using DSA as the reference standard, even though the visualization of petrous and the cavernous segments of the internal carotid artery (ICA) by CTA could be affected by bone artifacts. Recently, CTA has been used more and more to evaluate collaterality in ICAD, including the leptomeningeal collaterals, which have been correlated to the risk or recurrent events, and recurrent CVA rates have been reported in patients with high grade stenosis (70-99%) of none vs good collaterality: HR= 4.60, and poor vs good collaterality: HR= 5.90 [3637]. Consequently, collateral flow is one of the most essential mediators in cerebral ischemia due to ICAD, making it an important indicator in the prediction of risk and the assignment of treatment in patients with symptomatic ICAD.
The anterograde and collateral blood flow (AnCo) scoring system is useful as a score to predict the state of anterograde and collateral blood flow in patients with S-ICAD of the MCA. The AnCo scoring system consists of the anterograde score (AnS) and the collateral score (CoS) [38].
Bash et al, after analyzing 115 sick vessels, found that CTA has higher sensitivity than MRA to detect ICAD (98% vs 70%, p <0>
-High-resolution magnetic resonance (HRMRI): It help in the assessment of the morphology of the intracranial plaque and the adjacent arterial wall, revealing the morphology and components of the plaque, including intraplaque, lipidic nucleus, and fibrous layer hemorrhage [37].
-Perfusion images (PerfuMRI or PerfuCT): this imaging modality makes it possible to identify potentially recoverable tissue or ischemic penumbra, so that they could be used to quantify the real collateral flow in the context of ICAD [40].
Invasive methods:
-Digital subtraction angiography (DSA): It is currently considered as the reference standard for the diagnosis of intracranial vascular diseases, including ICAD, because of its excellent spatial and contrast resolution to represent the vessels, and its capability to reveal temporal information about anterograde and collateral flow. A disadvantage as an invasive method is that it may lead to complications during the procedure, with rates of 1:1000 general neurological complications being reported (close to 2% in patients with ICAD) [33]. Therefore, DSA should not be routinely used to diagnose ICAD.
A challenge posed by these diagnostic tests is their limited capability to differentiate between an atherosclerotic plaque and other pathologies such as partially occlusive thrombus, vasospasm, vasculitis, or even preocclusive Moyamoya disease. Lately, high-resolution images of the vessel wall have been used to identify substenotic but active atherosclerotic plaques. In patients with ICAD, eccentric arterial thickening, and fibrous cap thickening in the image of the vessel wall could favor atherosclerosis of the thrombus or vasculitis [41].
The SONIA (Stroke Outcomes and Neuroimaging of Intracranial Atheroclerosis) study assessed the precision TCD and MRA compared to DSA, and it concluded that both have high negative predictive values (86 and 91%, respectively), but low positive predictive values (36 and 59%, respectively). Both techniques identify 50 to 99% of stenoses of large intracranial vessels non-invasively with substantial negative predictive value. This means that TCD and MRA are efficient for the exclusion of ICAD, but are less useful to establish a diagnosis of ICAD and to estimate the severity of the stenosis. Additionally, abnormal findings in TCD and MRA require a confirmation test, such as DSA, to reliably identify stenosis [31].
DSA is the diagnostic test that more precisely measures the grade or percentage of intracranial stenosis, above non-invasive tests. In conclusion, DSA is the gold standard for diagnosis and quantification of luminal stenosis of intracranial circulation, which is an independent predictor of recurrent CVA in the context of ICAD [41]. However, the grade of stenosis is not the only determining factor. Other factors are collateral circulation (hemodynamic impact), and morphological characteristics of the atherosclerotic plaque (plaque components) [33].
There are three types of treatment for ICAD: Medical, endovascular, and surgical treatment.
Medical treatment
In 1995, Chimowitz et al (Warfarin-Aspirin Symptomatic Intracranial Disease Study Group: WASID) published the multicentric and retrospective study: the “Warfarin-Aspirin Symptomatic Intracranial Disease Study”, to compare the efficacy of warfarin vs aspirin in the prevention of major vascular events (CVA, AMI or sudden death) in patients with S-ICAD. Seven centers and 151 patients participated; 88 were treated with warfarin and 63 with aspirin. The follow-up median was 14.7 months (warfarin group), and 19.3 months (aspirin group). Kaplan-Meier analysis showed a significantly higher percentage of patients free of major vascular events among patients treated with warfarin (p = 0,01). The relative risk of an important vascular event for these patients was 0.46 (95%CI: 0.23-0.86) as opposed to patients treated with aspirin. Important hemorrhagic complications occurred in three patients treated with warfarin (including two deaths) in 166 patients-year of follow-up, and none in the patients treated with aspirin in 143 patients-year of follow-up. This study suggests a favorable risk-benefit relation for warfarin, compared to aspirin for the prevention of major CVA in patients with S-ICAD [43]. This resulted in anticoagulation being informed for the first time as treatment for S-ICAD. Figure 2.

Later on in 2005, Chimowitz et al (Warfarin-Aspirin Symptomatic Intracranial Disease Study Group: WASID) published the multicentric blind clinical trial: “Comparison of Warfarin and Aspirin for Symptomatic Intracranial Arterial Stenosis”, where they randomized patients with these inclusion criteria: age ≥ 40 years, non-incapacitating TIA or CVA occurring 90 days before randomization, and which was attributable to a 50-99% stenosis verified by DSA in a main intracranial artery, a modified Rankin score ≤ 3, in two groups: warfarin 5 mg per day (INR objective 2.0-3.0) vs aspirin (total dosis per day: 1300 mg, 650 mg every 12 hours). In total, 569 patients were randomized, the study was stopped because of the worry regarding the safety profile of the arm of patients assigned to warfarin. During an average follow-up period of 1.8 years. The death ratio due to vascular causes was 3.2% aspirin vs 5.9% warfarin (p = 0.16); the death ratio due to non-vascular causes was 1.1% vs 3.8%, respectively (p = 0.05). In conclusion, warfarin was associated with significantly higher rates of adverse effects and did not provide any benefits compared to aspirin in this study. Aspirin should be preferably used instead of warfarin in patients with ICAD. A subanalysis was performed in the following contexts: severe stenosis (70-99%), vertebrobasilar stenosis or CVA symptoms in patients with antithrombotic treatment (therapeutic failure or failure in the response), who were previously thought to be benefitting from anticoagulation therapy. However, the WASID study findings showed that none of these subgroups have a significant benefit with warfarin [5].
In 2009, Turan et al published “Failure of Antithrombotic Therapy and Risk of Stroke in Patients With Symptomatic Intracranial Stenosis”, where they compared CVA or vascular death rates in ON vs OFF patients (patients in antithrombotic treatment or warfarin at the time when the index event occurred to be included in the WASID study vs patients without treatment). Concluding, patients with S-ICAD who fail in antithrombotic therapy do not have a higher risk of CVA than those that do not fail with this therapy. Given the fact that patients with antithrombotic treatment ON and OFF have a higher risk of CVA in the territory, the intracranial stent placement assays should not be limited to only those who fail in this therapy [44].
In 2012, Xin Wang et al, published “The effectiveness of dual antiplatelet treatment in acute ischemic stroke patients with intracranial arterial stenosis: a subgroup analysis of CLAIR study”, where they carried out an analysis of subgroups of the CLAIR study in patients with CVA or TIA with ICAD and microembolic signs confirmed with TCD recorded on days 1, 2, and 7. They included patients during the first seven days after the onset of symptoms, randomizing in two groups: group 1, clopidogrel (day 1: 300 mg and subsequently 75 mg/day plus aspirin (75-160 mg/day) for seven days (dual treatment), or just aspirin (75-160 mg/day) for seven days (monotherapy). They included 70 patients, 34 in the dual treatment dual and 36 in the monotherapy group. To conclude, dual treatment with clopidogrel and aspirin for seven days is more effective than only aspirin for reducing microembolic signs in patients with S-ICAD [45].
In 2012, the “Stenting versus Aggressive Medical Therapy for Intracranial Arterial Stenosis, SAMMPRIS Trial Investigators” was published, supporting the use of dual antithrombotic in the short term with aspirin and clopidogrel, followed by just aspirin. In this study they compared the aggressive medical treatment (AMT) vs percutaneous transluminal angioplasty and stenting (PTAS) to prevent recurrent CVA. The AMT in the SAMMPRIS study included:
-Dual antithrombotic therapy: aspirin 325 mg/day + clopidogrel 75 mg/day for 90 days after enrollment and subsequently, aspirin 325 mg/day during the rest of the assay.
-Control of primary risk factors: blood pressure <140>
-Control of secondary risk factors: diabetes mellitus, elevated non-high-density lipoprotein (non-HDL) cholesterol, smoking, obesity, and sedentarism aided by a lifestyle modification program.
The common practice of keeping blood pressure slightly high in patients with S-ICAD to reduce the risk of CVA by distal hypoperfusion, and increasing the systolic arterial pressure during follow-up in WASID did not reduce the risk of CVA in the stenotic artery territory, but in fact it increased the risk of recurrent CVA.
Patients who had had a recent (30 days) TIA or CVA attributed to 70-99% stenosis of the diameter of a major intracranial artery with AMT or AMT plus PTAS with a Wingspan stent were randomly assigned. The primary outcome was CVA or death within the following 30 days after enrollment or after a revascularization procedure for the qualifying lesion during the follow-up period or the CVA in the territory of the qualifying artery after the 30 days. The study stopped at the beginning of 2011, regardless of the fact that follow-up will finish in 2013. In total, 451 were randomized, because the rate of CVA or death at 30 days was 14.7% in the PTAS group (12.5% non-fatal CVA and 2.2
In summary, substantial progress in the treatment of patients with ICAS has been achieved in the past decade, which has led to better prognosis for patients with this high-risk disease. Multidisciplinary medical treatment that incorporates short-term dual antiplaque treatment (for 90 days), followed by monotherapy with aspirin, together with intensive treatment of vascular risk factors, is the preferred treatment for CVA prevention in these patients. In spite of this aggressive medical treatment, a large subgroup of patients still have a high risk of recurrent CVA. For them, the advancement of endovascular therapy devices are offering better effectiveness and safety rates, which explains the frequent reporting of successful treatment studies with stenting.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
