
Research Article | DOI: https://doi.org/10.31579/2641-0419/114
* Associate Professor Department of cardiology Burdwan medical college and Hospital West Bengal, India.
*Corresponding Author: Goutam Datta, Department of Cardiology, the First Affiliated Hospital of Nanjing Medical University.
Citation: Goutam Datta (2020) Intracoronary Thrombolysis in no Flow after Primary Percutaneous Coronary Intervention in Acute Myocardial Infarction. J. Clinical Cardiology and Cardiovascular Interventions, 3(13); Doi:10.31579/2641-0419/114
Copyright: © 2020 Goutam Datta, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 November 2020 | Accepted: 10 December 2020 | Published: 17 December 2020
Keywords: primary percutaneous coronary intervention; no flow; intracoronary tenectaplase
Introduction: Mechanical revascularization of the infarct-related artery (IRA) is the most effective treatment modality in ST-segment elevation myocardial infarction (STEMI).No-reflow occurs in ∼8.8-10% of cases of primary percutaneous coronary intervention(PCI) in STEMI patients. Intracoronary tenectaplase was used when there was huge thrombus causing no flow in coronary artery following primary PCI in STEMI patients.
Methods: Five hundred and eighty primary PCI patients were studied over a period of two years i.e. January 2016 to December 2017. Drug eluting stents were used in all cases. Majority of our patients (>90%) came 6 hours after onset of chest pain. There were many patients where there was no flow even after mechanical thrombus aspiration and pharmacological vasodilator therapy. We have given 20 mg of tenectaplase through microcatheter in those cases.
Results: There were 44 cases of no flow in our series (7.75%). TIMI 3 Flow was reestablished in thirty two patients after intracoronary tenectaplase (72%). Amongst twelve failure cases LAD involvement was most common eight cases. RCA was involved in four patients. One month mortality rate in no flow group was 50% and 6.25% in successful recanalization group. One year mortality was 12.5% in successful recanalization group and 66% in no flow group. Both were statistically significant.
Conclusion: Refractory no reflow during primary PCI in STEMI is associated with high mortality and morbidity. There is no established strategy to solve this phenomenon. Intracoronary thrombolysis is an option to salvage these patients.
Acute myocardial infarction is due to plaque rupture and thrombotic occlusion of epicardial coronary artery. Primary percutaneous coronary intervention of infarct related artery(IRA)is the most effective treatment modality in ST-segment elevation myocardial infarction(STEMI) . Early revascularization of IRA will lead to favorable myocardial remodeling. It will reduce size of the infarct, improve left ventricular systolic and diastolic function and thereby will reduce MACE rate. Incidence of no flow is ∼8.8-10% in primary PCI of STEMI patients and it is associated with different risk factors like advanced age ,delayed presentation, ectatic coronary artery and huge thrombus burden. [1]
No flow after primary PCI may occur due to incomplete stent expansion, vaso spasm, dissection or in situ thrombosis. Microvascular obstruction and distal embolization are other contributing factors. Clinically no flow may present with the recurrence of chest pain, heart failure, malignant ventricular arrhythmias and cardiogenic shock. Angiographic no flow after PCI is associated with reduced myocardial salvage, larger infarct size and adverse cardiac remodeling. Early detection, preventive measures and treatment of no flow will decide final outcome after primary PCI. Routine use of aspiration catheter and Gp IIb/111a receptor blocker in primary PCI is not recommended now. [2] No therapies have been shown to prevent no-reflow. Different fibrinolytic agents are in use for systemic thrombolysis in STEMI. We have tried intracoronary tenectaplase when there is huge thrombus causing no flow in IRA after PCI in STEMI patients. There are case reports of intracoronary thrombolysis in STEMI patients when there is huge thrombus burden.3 It will lyse thrombus and will facilitate future revascularization. But we used intracoronary thrombolysis in those patients where there is no flow in IRA after primary PCI.
Methods: Our objective was to study whether intracoronary tenectaplase is beneficial or not in no flow in coronary artery after primary PCI. 'Ethical approval and consent to participate' was taken before conducting the study. Patients in the age group of 18 to 75 were only considered for our study. No flow was defined by Thrombolysis in myocardial infarction(TIMI) zero grade flow or TIMI I flow. We have studied 580 primary PCI patients done in our hospital over a period of two years i.e. January 2016 to December 2017. Drug eluting stents were used in all cases. Majority of our patients(>90%) came 6 hours after onset of chest pain. Average presentation was 8-12 hrs after onset of chest pain. Protocol guided periprocedural medication include Aspirin(325 mg first dose, then 75 mg daily), Ticagrelor(180mg first dose, then 90 mg twice daily),atorvastatin(80 mg first dose, then 80 mg daily). Patients with atrial fibrillation were excluded from the study. Long lesions requiring overlapping stents were also excluded from our study. Direct stenting was tried in all cases. Predilatation at low pressure was done where there was difficulty in stent delivery. Infarct related artery only was addressed in our study and only single stent strategy group was included in this study.We have used thrombus aspiration catheter and Gp IIb/IIIa receptor blocker when there is huge thrombus load ( TIMI thrombus grade 3 or more).Intracoronary adenosine and nicorandil were used as adjunctive pharmaco therapy to alleviate no flow. There were many patients where there was no flow even after mechanical thrombus aspiration and pharmacological vasodilator therapy. We have given 20 mg of tenectaplase through micro catheter in those cases. We have taken our patients 48 hours after procedure for routine repeat coronary angiography as study protocol. There were few haemodynamically unstable patients and we have taken them for repeat angiography after 7 days .TIMI 3 flow was taken as successful recanalization criteria.
Inclusion criteria for intracoronary tenectaplase :
1) Age group 18-80
2) Primary PCI patients
3) No flow flow after mechanical thrombus aspiration and pharmacological vasodilator therapy
4) No prior history of intracranial hemorrhage
Statistical analysis: Instat 3 software was used for statistical analysis.
Fisher exact test was done to evaluate statistical significance between two groups.
Majority of our procedures (70%) were done by radial route and rest (30%) by femoral route. Manual compression was done to secure haemostasis.We have observed 44 cases of no flow in our series. Incidence is around 7.75%.Twenty six patients were suffering from diabetes. Incidence was 60%.Thirty patients were male and fourteen were female patients. Male prevalence was 68% and female prevalence was 32%. (Table 1and 2) Twenty four patients were hypertensive. Incidence is about 54%.
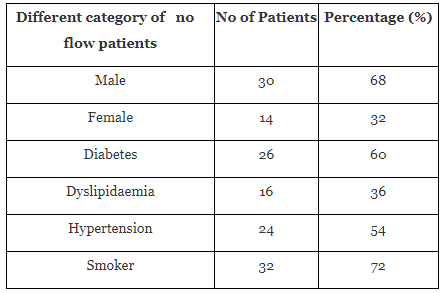

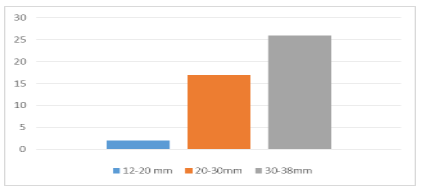
Thirty two patients were smokers taking more than 10 cigarettes per day. Prevalence is around 72% and it was most common risk factor. Dyslipidaemia was seen only in sixteen patients and incidence was about 36%.No flow was common in elderly patients. Only four patients were below 40 years age group. Twelve patients were in the 40-60 years age group. (Chart 1) Twenty patients were in the age group of 60 –80.Fourteen patients were in cardiogenic shock requiring pharmacological pressure support mainly noradrenaline, dobutamine and dopamine.

We did not use mechanical circulatory support device in any of our patients. Amongst patients with cardiogenic shock ten patients had anterior wall STEMI and four patients had inferior wall STEMI. Amongst cardiogenic shock cases ten patients were diabetic. Incidence is 70%. Majority of them were having multi vessel disease. Two patients died during hospital stay. They were suffering from anterior wall STEMI. We could not reestablish flow in those patients. They were having persistent cardiogenic shock. Incidence of no flow was higher in longer stent length. (Chart 2)Left anterior descending artery(LAD )was involved in eighteen patients. Right coronary artery(RCA) was culprit in twenty four cases. No flow was most common in RCA territory. Least common was left circumflex(LCX) artery. (Chart 3) Only two caseswere seen in LCX territory. TIMI 3 Flow was reestablished in thirty two patients. Success rate was around 72%. (Chart 4) Out of twelve failure cases LAD involvement was most common ---eight cases. RCA was involved in four patients.
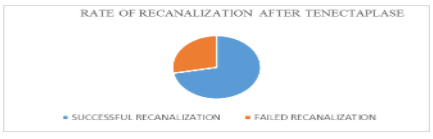

Though incidence of no flow was higher in RCA territory but successful TIMI 3 flow restoration was also most common in RCA. Average diameter of RCA was greater than LAD. Most RCA were tortuous, dilated and ectatic. Overall failure rate was 28%. Amongst failure cases two patients died in their hospital stay and they were having persistent cardiogenic shock. Four patients died during thirty days. One died in his home probably because of arrhythmia. Two died due to persistent heart failure later on. Another was admitted with heart failure but died due to incessant ventricular tachycardia refractory to recurrent electrical cardioversion. Two more patients died within one year again due to heart failure. Amongst successful recanalization group two patients died due to ventricular arrhythmia in first month. Two patients succumbed within a year because of heart failure. None of them died during their hospital stay. One month mortality rate in no flow group was 50% and 6.25% in successful recanalization group. (Table 3). (Chart 5) One year mortality was 14.5% in successful recanalization group and 72% in no reflow group. (Table 4) One month mortality rate in no flow group was 50% and 6.25% in successful recanalization group.


Relative risk of dying within one month in no-reflow group as compared to successful recanalization group is highly significant (RR is 8.00 ;95%Confidence interval 1.864 to 34.333; with a p-value of 0.0027). Thirty two patients died in first year in no reflow group(72%). Seventy six patient died in first year in successful recanalization group(14.4%).Relative risk of dying within one year in no-reflow group as compared to successful recanalization group is statistically significant (RR is 5.333 ;95% Confidence interval 1.961 to 14.504; with a p-value of 0.0009).
No flow is seen around 8.8-10% patients of primary percutaneous intervention(PCI) in ST elevation myocardial infarction(STEMI) patients. No flow is associated with increased morbidity and mortality. No flow can result in poor healing of the infarct, adverse left ventricular remodeling and it increases risk for major adverse cardiac events, including congestive heart failure and death. Despite considerable insight in recent years regarding who is at risk for no-reflow and how management strategies work, no specific therapies have been devised, and the evidence in support of their use remains contentious in many cases.
No flow is accompanied by chest pain, electrical instability and possible hemodynamic compromise. The mechanisms of no reflow are thrombus-plaque embolisation, platelet activation, release of vasoconstrictors and vasospasm. Thirty day mortality of refractory no flow is 32%. [4] No reflow is directly proportional to thrombus burden. Lot of STEMI patients have huge thrombus burden. After stent deployment or balloon dilatation thrombus may fragment and migrate distally in coronary artery. Routine use of aspiration catheter and Gp 11b/111a receptor blocker in primary PCI is not recommended now. TASTE trial has proven that routine use of aspiration catheter is not beneficial but it increases incidence of stroke. [5]
Rezkalla et al had studied 347 STEMI patients treated with primary PCI and found no-reflow phenomenon in 32% of patients. Patients with no-reflow had received pharmacological vasodilator therapy like intracoronary nitroprusside, nicardipine, or verapamil and they had experienced improvement in coronary flow and better prognosis. [6] Factors known to be associated with high risk of no flow in STEMI patients include delayed presentation to the catheterization laboratory, hyperglycemia, and hypercholesterolemia. No flow is also more frequently encountered in association with female sex, hypertension, mild-to-moderate renal insufficiency, and elevated inflammatory markers. [7] There are also lesion-specific features that may increasethe risk of no flow, such as plaque composition and hrombus burden as detected by intravascular ultrasound. [8] In patients with diabetes, optimal blood sugar control before the procedure can reduce the occurrence of no flow. In individuals with hyperlipidemia, intensive statin therapy before PCI is beneficial in reducing no-reflow.9Prevention strategies should include primary stenting, avoidance of high pressure stent deployment, and thrombectomy before the intervention if there is huge thrombus load. [10] In a study by Sezer M et al, primary PCI followed by the intracoronary low-dose streptokinase was compared with standard primary PCI without the use of intracoronary streptokinase. In the streptokinase group, 250 kU of streptokinase diluted with 20 ml of saline was infused through the guiding catheter. It has been shown that intracoronary strptokinase therapy prevents left ventricular dilation, preserves systolic function, and decreases long-term LV infarct size by 31%. [11] Daniela Boscarelli et al had studied thirty STEMI patients having large thrombus burden after failed mechanical thrombus aspiration. Intracoronay thrombolysis was used in low dose by infusion catheter (one-third systemic dose of tenecteplase 27% cases) or alteplase (73% cases). In their series thirty three percent patients presented 12 hours after onset of chest pain and seventeen percent were in cardiogenic shock. TIMI flow grade improved from 0/1 at baseline (93%) to ≥2 in most patients (97%). Blush grade 2–3 was observed in 85% of patients and there were more than 50% ST-segment resolution in 82% of cases. In-hospital mortality was 10%. They did not observe any major bleeding complication. [12] Kelly et al had studied thirty four STEMI patients who had no flow after primary PCI. They have used GP 11b/111a receptor blocker and low dose intracoronary tenectaplase. Mean dose of 10.2 ± 5.2 mg. There was improvement in angiographically visible thrombus and/or intracoronary blood flow in 31 (91%) patients. But there were four in‐hospital deaths, two reinfarctions, no stroke, one major bleeding event, and three minor bleeding events in their series. [13]
In our study incidence of no flow was 7.75%.Relative risk of death was higher in this group(9.75). TIMI 3 flow was established in 72% of cases after intracoronary tenectaplase. Relative risk of death in patients who did not achieve TIMI 3 flow after intracoronary tenectaplase were high( one month relative risk 8 and one year relative risk 5.3).Right coronary artery was most commonly involved and least common was left circumflex artery. Left anterior descending artery was most recalcitrant artery for TIMI 3 flow restoration after thrombolysis. Thrombus burden and vessel ectasia were two important predisposing factors for no flow. Late presentation could be contributing factor for large, recalcitrant thrombus burden. There was no major bleeding complication in our study. We did not observe any intracranial of gastrointestinal bleeding complication. Local puncture site haematoma were also not significant after intracoronary thrombolysis Primary PCI is associated with high rates of distal embolization due to high thrombus burden. The sequelae of distal embolization results in reduced myocardial perfusion and increased myocyte damage. Macroscopic distal embolization may be seen in up to 16% of patients undergoing primary PCI and suboptimal tissue perfusion may be seen in 20% to 40% of patients despite restoration of TIMI 3 epicardial flow in the catheterization laboratory. [14] A number of vasodilator agents have been shown to improve TIMI flow rate, corrected TIMI frame counts, and wall motion score index. Such vasodilator agents include adenosine, verapamil, nicorandil, and norepinephrine and sodium nitroprusside. [15]
Conclusion: Refractory no reflow during primary PCI in STEMI is associated with high mortality and morbidity. There is no established strategy to solve this phenomenon. Intracoronary thrombolysis is an option to salvage these patients.
Limitations: Majority of or patients had presented six hours after onset of chest pain making thrombus burden heavy. It was a single centre observational study, not a randomized trial. There could be selection bias in our observation.
Conflict of interest: I do not have any conflict of interest.
Financial:
I do not have any financial disclosure regarding this manuscript
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
