
Case Report | DOI: https://doi.org/10.31579/2690-4861/448
1Singida Regional Referral Hospital, Tanzania
2 Singida Region Medical Officer
*Corresponding Author: Gilbert Waria, Singida Regional Referral Hospital, Tanzania.
Citation: C. Ramadhan B. Kabala, Rukia Ibrahim, Mwanaid Mkwizu, Rogatus Duwe, Faraja P. Kazuba, Yazan Alamro, Essa Kadiri, et al, (2024), Double Trouble Unmasked: Femoral Pseudoaneurysm and Deep Venous Thromboses Following Coronary Angiography, International Journal of Clinical Case Reports and Reviews, 17(5); DOI:10.31579/2690-4861/448
Copyright: © 2024, Gilbert Waria. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2024 | Accepted: 25 April 2024 | Published: 17 June 2024
Keywords: haemorrhagic stroke; radiological investigations; ischemic stroke
Background: Pediatric hemorrhagic stroke is rare and frequently associated with vascular lesions. Children with congenital heart diseases commonly present with ischemic stroke and rarely presenting with hemorrhagic stroke.
Case presentation: We present a 9 years old girl with one day history of right sided weakness (hemiplegia) preceded by headache for two days. Radiological investigations were helpful in confirming left cerebral haemorrhage, transposition of great arteries, common atrium and situs inversus with levocardia in this patient. Laboratory investigations indicated high haemoglobin level and high red blood cell counts. We report a rare case of intracerebral haemorrhagic stroke in a child with multiple congenital malformations
Conclusion: We concluded that high haemoglobin and red blood cell counts due to the recurrent hypoxia from deoxygenated blood and strenuous activities can occasionally cause spontaneous bleeding in visceral organs including the brain.
Paediatric stroke is a relatively rare occurrence with an annual incidence of 1.2-13 cases per 100,000. Haemorrhagic strokes account for half of these cases. In adults, haemorrhagic strokes are predominantly hypertensive in aetiology. However, in paediatric population, haemorrhagic strokes are frequently associated with vascular lesions (50%) such as Arteriovenous malformations (AVMs), arteriovenous fistulas or cavernous malformations. Other causes of ICH in paediatric population include bleeding diathesis (21%) due to liver failure, DIC and congenital coagulopathies, thrombocytopenia due to malignant (Acute lymphocytic leukemia, Acute Myeloblastic Leukemia), congenital (aplastic anaemias, bone marrow failure), immune- mediated, and autoimmune (1)
The remaining 25% of aetiology of intracerebral haemorrhage in paediatric population includes aneurysm (9%), haemorrhagic primary intracranial tumour (6%) and 10% are due to CNS infections, cerebral vasculitis, and Mayomayo disease (1). congenital heart disease (CHD) is present in about 1% of live births and is the most common congenital malformation. Congenital heart disease is the major risk factor for ischemic stroke and stroke recurrence in children (2).
In congenital heart disease the frequent use of anticoagulant drugs in previously diagnosed children for prevention of ischemic increases the intracranial haemorrhage risk. Intracerebral haemorrhage in children with congenital heart disease and who is not on anticoagulant drugs
is an extremely rare condition and to the best of our knowledge, it has not been previously reported
A 9 years old female presented in our hospital complaining of right-sided body weakness for one day which was of sudden onset progressively increasing in severity with time. However, it was associated with aphasia, left-sided mouth deviation, and loss of consciousness. There was a history of headache two days before the current presentation. There was no history of vomiting, fever, or convulsion. The past medical history revealed recurrent dry cough, chest tightness, palpitation, and easy fatiguability on exertion however no history of bluish discoloration of lips and skin. The patient reported a history of nasal bleeding two weeks prior to admission, however no history of easy skin bruising, excessive bleeding on minor injury, gum bleeding or yellow discolouration of the eyes.
On examination, the patient was not pale, had no pedal oedema, normal pulse rate of 78 bpm, BP ,119/83mmHg, RR ,17, afebrile 36.7oC, SPO2 ,98% , had precordial hyperactivity, apex beat located at 4th intercostal space midclavicular, had facial asymmetry, right-sided weakness of power for upper limb and lower limb of 1/5 with reduce tone and bulkiness.
Haematology parameters were as follows: Hb, 17.2g/dl (11.2 – 14.5), RBC, 6.78x1012/l (4.0 – 5.5 x 1012), HTC ,54.4% (35 – 44) , MCV=80.3Fl (82.4 – 87.3), MCH=31.7g/dl (32.0 –36g/Dl), WBC=5.30x109/l, Lymphocytes % ,42.0, Eosinophils %, 8.1, Platelets, 141x109/l (150-450x109/l), sickle cell scan, HbAA and RBG ,6.3mmol/l, (5.3-9.9mmol/l)
On radiological examination, Echocardiography revealed a common atrium due total absence of the interatrial septum, mild tricuspid regurgitation, preserved ejection fraction of 58.9% and preserved ventricular geometry (Figure 1). Ultrasonography of the abdomen revealed transposition of the major visceral organs (the spleen and stomach are located on the right side). Liver is enlarged occupying the whole upper part of the abdomen. There are two main hepatic veins (with 3 branches, each) joining before draining directly to the common atrium (CA) and left-sided inferior vena cava (IVC) (Figure 2).
Chest x-ray showed prominent central pulmonary vessels, increased pulmonary lung markings, and an enlarged heart narrowed superiorly (string-on-egg sign) (Figure 3).
Subsequent computed tomography (CT) of the brain revealed a hyperdense lesion 2.9x4.1cm of blood density in the left parietal lobe involving the thalamus suggestive of hematoma (Fig 4). The computed tomography of the chest showed cardiomegaly with laevocardia, common atrium connected to the right and left ventricle separately, right-sided aorta connected to the right ventricle, pulmonary artery connected to the left ventricle, left-sided inferior vena cava (IVC) draining both upper and lower left part of the body directly into the common atrium on the left side, single right-sided superior vena cava (SVC) draining the right upper part of the body into the common atrium on the right side (Fig 5). The upper abdomen revealed transposition of the major visceral organs. There are two main hepatic veins (with 3 branches, each) joining before draining direct to the common atrium (CA) (Fig 6)
Patient Course
The patient was managed by physiotherapy and IV Ceftriaxone +Sulbactam for 8 days in the ward, then was discharged home to continue with physiotherapy.
After 2 weeks Patient regained power on her right lower limb and was able to walk again, but there was still some weakness on her right upper limb (power 3/5) which improved as she continued with physiotherapy. Then she was given a referral to the National Heart Institute for further management.
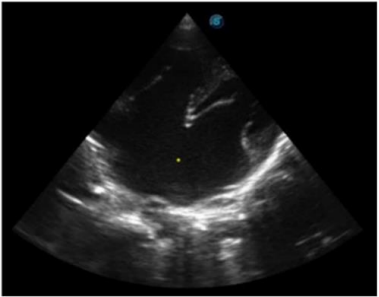
Figure 1: Echocardiography showing common atrium *
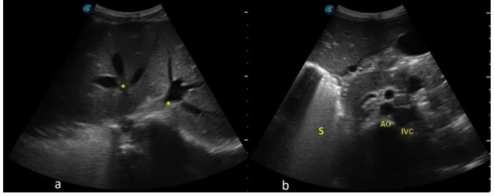
Figure 2: (a)Ultrasound showing liver with two lobes each drained by its own three hepatic veins * (b)Ultrasound showing left placed inferior vena cava and right placed stomach (S).
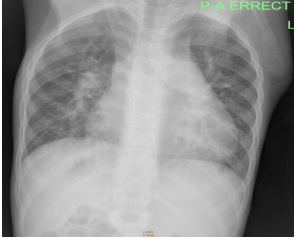
Figure3: Chest x-ray showingincreased pulmonary vasculature with marked cardiomegaly.
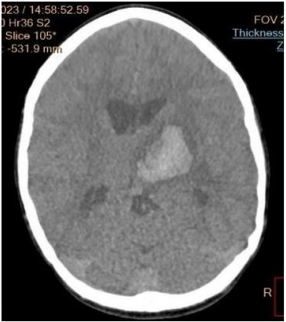
Figure 4: CT scan of the brain showing left cerebral hematoma at the levelof the thalamus.
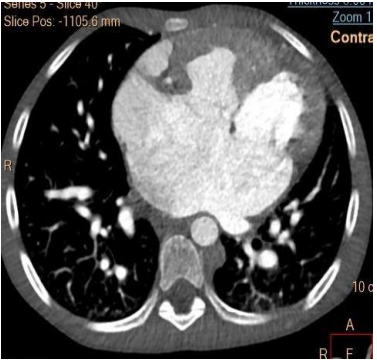
Figure 5: CT scan ofthe chest showing a common atrium and left IVC.
Spontaneous Intracranial haemorrhage
Intracranial haemorrhage is presented with headache followed by focal neurological deficit and decreased in level of consciousness that may progress to coma like in our case. Emboli form congenital heart disease (CHD) is a major risk for developing ischaemic stroke in paediatric
(2). Ischaemic stroke may progress to the haemorrhagic infarction which will present with headache preceded by a neurological deficit in contrast with this patient (3). Moreover, one- third of ischaemic stroke resulted from cerebral venous thrombosis may proceed to haemorrhage and these patients commonly present with seizures in contrary to our case (4). Haemorrhagic stroke in child with congenital heart disease (CHD) is relatively rare and may be due to other causes. In this patient, laboratory investigation revealed high haemoglobin
17.2g/dl and high red blood cell counts 6.78x1012/l which may commonly cause ischaemic stroke. However, some of the effects of high haemoglobin and RBC counts are headache and easy bruising or bleeding due to dysfunction of platelet aggregation and the prolongation of activated prothrombin time (5). Our case presented with episodes of nasal bleeding two weeks and headache a day prior to onset of stroke which may be due to high haemoglobin and high RBC count (polycythaemia).
Transposition of great arteries (TGA)
The ventricles are inverted and connected to the opposite great artery, right ventricle to the aorta and the left ventricle to the pulmonary artery, thus forming a total transposition of great arteries. In patients with complete TGA the systemic and pulmonary circulations are in parallel. Thus, TGA is a severe congenital heart disease incompatible with extrauterine life (6,7). However, survival of this patient had been possible due to atrial shunt resulting from the common atrium (CA) and transposition of the inferior vena cava (8). This case represents a beautiful example of how nature resolves hemodynamic problems.
Systemic Venous drainage
The inferior vena cava which is transposed to the left side is joined by the left brachiocephalic vein before draining in the left side of the common atrium. The liver has two main hepatic veins joined and drain directly into the common atrium slightly to its left side. Thus, the major systemic venous drainage is connected to the left side of the heart allowing most of the deoxygenated blood carried to the lung via transposed pulmonary artery.
The superior vena cava is formed by the confluence of the right brachiocephalic vein and right subclavian vein and drains to the right side of the common atrium, thus only a small amount of deoxygenated blood enters the right ventricle, hence the aorta.
There is no history of cyanosis in this patient which is explained by the above abnormal systemic venous drainage allowing most of the deoxygenated blood to the pulmonary artery. However, the small amount of deoxygenated blood (about 25%) in the circulation from the superior vena cava triggers the production of high red blood cells (polycythaemia) due to tissue hypoxia during strenuous activities in this child.
Isolated levocardia (Situs inversus with levocardia)
There is a reversal of the abdominal viscera in this patient in which the spleen and stomach are on the right side while the inferior vena cava and the liver are on the left side. In most cases of situs inversus the cardiac apex lies on the right side but rarely it will lie on the left side (Isolated
levocardia) as in our case (9). The incidence of congenital heart disease is 100% in patients with situs inversus with isolated levocardia and only about 5% to 13% of patients survive more than 5 years as in our case (9).
Intracranial haemorrhage is rare in the child with congenital heart diseases however recurrent hypoxia from deoxygenated blood and strenuous activities may cause high blood viscosity (polycythemia) that not only can cause ischaemic stroke but also can occasionally cause spontaneous bleeding in the visceral organs including the brain. Clinicians and Radiologists need to rule out congenital heart diseases in patients who present with situs inversus and levocardia.
This study is exempt from ethical approval at our institution, no ethical clearance is required as it only involves case reports. The written consent was obtained from the parent of the patient.
The authors declare that they have no conflict of interest.
No fund granted for this study
Ramadhan B. Kabala: Radiologist who interpreted all Radiological investigations, reviewed all the medical history and laboratory investigations and manuscript writing
David Mwasota, Ibrahim, Mwanaid Mkwizu, Rogatus Duwe, Roza Majengo, and Patrick Ng’unda: Clinicians in the Paediatric Department Medical department who attended the patient, performed clinical evaluation, reviewed laboratory investigations and patient management and treatment.
Faraja P. Kazuba: Intern Doctor who reviewed all the medical history and laboratory investigations and manuscript writing.
Baraka Hezron: Radiographer who performed Echocardiography and Computed tomography
Victorina Ludovick, Gilbert Waria, and Lugano Daimon: Research Scientists, Epidemiologists, Biostatisticians, public health research monitoring and evaluation experts who reviewed the literature and reviewed the final edits of the manuscript
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
