
Case Report | DOI: https://doi.org/10.31579/2639-4162/053
1 Nephrology, Dialysis and Kidney Transplantation Department. La Rabta Teaching Hospital, Faculty of medicine of Tunis, University of Tunis El Manar, Tunisia.
2 Cardiovascular Surgery Department. La Rabta Teaching Hospital, Faculty of medicine of Tunis, University of Tunis El Manar, Tunisia
3 Cardiology Department. Hbib Thameur Hospital. Faculty of medicine of Tunis, University of Tunis El Manar, Tunisia
*Corresponding Author: Sobhi Mleyhi, Department of cardiovascular surgery, La Rabta Hospital, Jabbari Street 1007 Tunis, Tunisia
Citation: Ikram Mami, Soumaya Mekki, Jalel Ziedi, Imtinene Ben Mrad, Mleyhi Sobhi, et al. (2021) Intra-Atrial Tunneled Dialysis Catheter as Vascular Access: Ultimate Choice in a Hemodialysis Patient. J. General medicine and Clinical Practice, 4(1); Doi:10.31579/2639-4162/053
Copyright: © 2021 Sobhi Mleyhi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 September 2021 | Accepted: 11 October 2021 | Published: 18 October 2021
Keywords: end-stage renal disease; hemodialysis; trans-lumbar tunneled catheter; intra-atrial tunneled dialysis catheter or deleterious treatment
Recurrence of complications related to usual vascular access leads to exhausted vasculature. Several options were described in similar cases like tans-lumbar catheter and intra-atrial tunneled dialysis catheter.
We report the case of a 22-year-old- male, with kidney failure, anuria and exhausted vasculature. Emergent kidney transplantation was not suitable to his case. We decided to combine peritoneal dialysis with once-a-week hemodialysis using a tans-lumbar tunneled catheter at first time, then an intra-atrial tunneled dialysis catheter as vascular access of last resort.
Development of renal replacement therapy expose nephrologist to new challenges. Working on alternative therapy is inspiring, but rationalizing exploitation of current options meanwhile is imperative.
AVF: arteriovenous fistula
AVG: arteriovenous graft
CVC: central venous catheters
IATDC: intra-atrial tunneled dialysis catheter
TDC: tunneled dialysis catheters
TLDC: translumbar tunneled dialysis catheter
RRT: renal replacement therapy
PD: peritoneal dialysis
HD: hemodialysis
Hemodialysis (HD) is the major modality of renal replacement therapy requiring an adequate vascular access as arteriovenous fistula (AVF). However, recourse to central venous catheters (CVC) is often necessary in adult patients. For children as well, age-related anatomical limitations and expectations for early transplantation were correlated with CVC preference up to 30% at dialysis initiation [1]. The use of dialysis catheters induces at many times venous stenosis and occlusion exposing to vascular access loss and exhaustion of conventional vascular access [2, 3]. This point is not clearly defined, and depends on institutions and surgical practices [4, 5]. Consequently, the prevalence of hemodialysis patients with exhausted vasculature is not established yet, but seem to be increasing.
The management of end-stage renal disease patients includes continuous researches to improve both life-expectancy and life-quality in this population. Then, unconventional tunneled dialysis catheters (TDC) have been reported in patients with no upper and lower body venous access including different sites as: translumbar, transhepatic or transrenale. [6]
Intra atrial tunneled dialysis catheter (IATDC) is a vascular access reserved at last resort and salvage therapy. Only, a few cases or small series were reported in the literature [7]. We report an exceptional case of combined peritoneal dialysis (PD) to HD used translumbar and IATDC.
A 22-year-old- male with end-stage renal disease (ESRD) undergoing dialysis, was admitted at first time in our department for vascular access exhaustion 3 years ago.
In childhood, he was diagnosed with ureteropelvic junction obstruction, and vesicoureteral reflux. Then, he developed a kidney failure and ended up on dialysis at fourteen.
Then, he was referred to our department at the age of 20 for exhausted vasculature. At that time, he had required several tunneled and non-tunneled venous catheters in femoral and jugular sites, three AVF and two arteriovenous graft (AVG). Considerable attempts to get adequate venous access in usual sites failed.
Computed tomography scans and angiographies showed thrombosis of both subclavian veins extended to superior vena cava. Further imaging confirmed thrombosis of both femoral venous. Etiological investigations didn’t reveal thrombophilia.
A translumbar tunneled dialysis catheter (TLDC) has been inserted in
extreme emergency by cardio vascular surgeon. Because of the poor outcomes of unconventional TLDC, peritoneal dialysis was combined to once weekly hemodialysis. Icodextrin was used as peritoneal solution because of anuria. In less than a year, trans-lumbar catheter was removed for dysfunction. Computed Tomography scans confirmed persistent superior vena cava and an inferior vena cava thrombosis. Renal transplantation was discussed but considered as not appropriate.
Fourteen months ago, he was admitted for severe septicemia and was treated with broad-spectrum antibiotics. During hospitalization, patient had edema, hyperkalemia and severe anemia requiring urgent hemodialysis. The use of intra-atrial tunneled dialysis catheter (IA TDC) as vascular access was indicated by cardiovascular surgeons as salvage therapy.
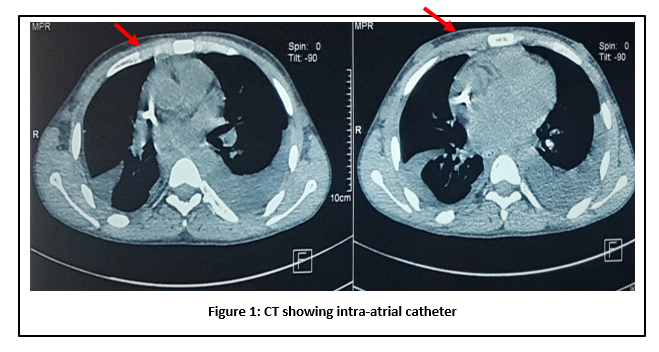
The surgery was carried out under general anesthesia by a right anterior thoracotomy. After opening the pericardium, the catheter was placed in the right atrium, fixed and tunneled [Figure 1et 2]. When closing the various incisions layer-by-layer, double tube was inserted in the pericardium and pleural cavity to drain possible hemorrhage, while the cuff was put in the chest wall.

Throughout four weeks, an infection related to IA TDC was reported with favorable outcome.
Nine months later, PD catheter became not functional after severe peritonitis and was removed.
Nearly 2.3 million people worldwide depend on HD [8]. Despite progress, vascular access remains the weak chain in HD adequacy, and a critical determinant of median survival and life quality for HD patients. All guidelines recommend creation of AVF followed by AVG and CVC at last.
However, CVC are increasingly used as a temporary option pending AVF maturation, or as a permanent alternative after expiration of different possibilities. In fact, according to the Annual Data Report of end stage renal disease in the United States, 80% of patients used a tunneled central venous catheter at hemodialysis initiation, 17% used a fistula, and 3% a graft; 90 days after dialysis initiation, 69% of the patients were still using a catheter [9].
Infections and thrombosis, as the main complications related to CVC, lead to a loss of vascular access in the relevant vein respectively in 10% and 30 to 40% [10, 11]. Consequently, many patients, like ours, exhaust their veins.
When conventional venous sites as internal jugular, femoral and subclavian are exhausted, several unconventional catheters have been used in the literature as alternative solution like translumbar, trans-hepatic, trans-renal, great saphenous, azygous, hemi-azygous veins [6, 12, 13]. Rahman S. and al. reviewed technical challenges and complications of common unconventional dialysis catheter [14]. The highest incidence of immediate and early complications was recorded with transhepatic catheter. Although the overall morbidity and mortality was at higher rate comparing to traditional TDC, different technique proved efficiency and extended patients ‘life few months to several years.
In our case, TLDC was used in first time because of thrombosis of superior vena cava but lasted less only one year. Lund and al. described initially this alternative in 1995 [15].The main complications affecting significantly the median survival were infection and catheter dysfunction. However, prevalence of problems related to central venous catheter are significantly more important with TLDC. Recent studies reported that 41.6% of patients presented a catheter-related first infection after 98 ± 72.1 (6-201) days and estimated long-term patency at 12 months was 45%. [13, 16]. This type of catheter can be considered as a safe, temporary alternative access for selected hemodialysis patients with exhausted vasculature [13]
Our patient had another type of unconventional TDC as IATDC after both superior and inferior vena cava thrombosis. At that time, it was the only solution to maintain him alive. This technique was first reported by Chavanon et al. in 1999 [17]. Since then, other case reports and small series recorded similar illustrations [18-21].
Recently a systematic review included 51 patients with IATDC [7]. All the patients had exhausted conventional vascular accesses. All IATDCs were put by cardiovascular surgeons following the same method described in our case report. [7]
In the same review, six patients developed IATDC-related sepsis. At the end of follow-up, 13 patients died: seven patients died within 15 days following IATDC insertion: 3 catheter related deaths and 1 septic shock. Six additional patients died later than 15 days not related to catheters. Median survival time in patients with IATDC was 25 months, lower than conventional TDC which was 36 months [7, 22].
Combination of once-weekly hemodialysis with peritoneal dialysis, as in our case, reduce manipulation of the IATDC which can lower related risks and enhance median survival, but not indicated often although it has proven efficiency. [23, 24]
In fact, bimodal dialysis is associated with lower vascular access infection, and lower all-cause mortality compared with PD [25-27] This therapy is widely used in Japan (20% of all PD patients) [27]. Our experience with bimodal dialysis lasted for nine months before switching patient to exclusive hemodialysis.
There are innumerable publications that approved PD as renal replacement therapy, but few data about the outcomes of anuric patients on PD, or about life expectancy when transferred from HD [28].
Vascular exhaustion is a big challenge for nephrologists. The uncommon TDC can be used. But complications related to this type of catheters should be more frequent and consequently lower survival time. For this, we reported bimodal dialysis as another alternative to get better survival period. Based on our experience, we propose the following algorithm for management of ESRD [Figure 3].

No Conflits of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
