
Literature Review | DOI: https://doi.org/10.31579/2637-8892/158
*Corresponding Author: Emenike J Umesi, Visiting Lecturer, Global Distance Learning Institute, Abuja, Nigeria.
Citation: Emenike J Umesi (2022) Interventions for Persons Affected by Conflicts & Insurgency: An Assessment of Psychosocial Support in Idp Camps In Nigeria. Psychology and Mental Health Care, 6(3): DOI: 10.31579/2637-8892/158
Copyright: © 2022, Emenike J Umesi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 November 2021 | Accepted: 05 January 2022 | Published: 22 January 2022
Keywords: psychosocial, interventions, mental health, internally displaced persons, war-affected youth
Armed conflicts and insurrections are a precursor for mental health challenges in children, adolescents and young adults. A wide range of psychosocial approaches have been suggested for managing such challenges which result from these conflicts driven situations. This study investigated the extent to which psychosocial intervention programmes are implemented for the internally displaced persons (IDPs) in the camps in Maiduguri, Borno state, Nigeria and how these programmes are able to meet the needs of the affected persons. A qualitative research design was adopted, and three research questions were generated. Subjects are 200 respondents that are selected from a target population of 1005 displaced persons in two (2) camps in Borno state, through simple random sampling. Instruments used for data collection included questionnaire, interviews and focus group discussions. The result of the study showed that several psychosocial approaches were utilized in the management of the post trauma challenges and were rendered by various professional and volunteer groups in the camp. The study concludes that effective and efficacious interventions for these conflicts driven challenges require strengthening and that these services which are available in the camps require retooling, deepening and some conscious improvement.
By January 2017, the total number of displaced persons in the world was about 40.3 million, and out of this figure, the newly displaced within their own countries by natural disasters, conflict or human rights violations at the end of December 2016, amounted to roughly 31.1 million. Sub Saharan Africa contributed 2.6m of the 6.9m figures for conflict-induced displacement. (IDMC, 2017)
Nigeria as of January 2020 had a total of 2,583,000 persons internally displaced due to violence and conflict out of the world’s over 40.0 million displaced persons. This displacement comes with a lot of incidents and experiences that leave the victims or affected persons traumatized. By the peculiar nature of these incidents, families have been separated, communities have been destroyed, and basic infrastructure damaged. The basic social and economic activities in the various communities have been disrupted making the need for humanitarian action inevitable. In the last few years, displacements have occurred in various parts of the country, coming along with its trademark of trauma and other social issues that also has a lot of impact on the mental health of the affected persons. Some of the states affected by displacement in the country include Adamawa, Borno, Yobe, Zamfara, Benue, Nasarawa, Cross River, Katsina, Ebonyi, etc. The causes of these displacements range from human induced to natural disaster incidents. The resulting effects of these incidents go a long way to affect the displaced persons in the form of post disaster trauma. In cases of this nature, a consciously planned programme of psychosocial intervention is supposed to be in place and made available to all affected persons who require such mental health related services. It is based on the above, that this study is being carried out to assess the extent to which this sensitive aspect of social work intervention programmes is made available to the affected persons and whether it has helped to effectively mitigate the post disaster trauma challenges being faced by the internally displaced persons in the camps in Maidugur.
There are a lot of studies on the psychosocial interventions for persons affected by insurgencies and conflicts. However, these studies have significant gaps that justify the need for this study. Below is the review of the related literature.
The exposure to life threatening events overwhelms adults, as well as infants and children and could lead to emotional distress and traumas. The manifestation of these traits could be in form of delays in development, changes in behaviour, and other severe health and psychological conditions. Stucki and Cieza (2014) explained that programming of psycho social services involve arranging activities which are aimed at managing the psychological and social advancement of people in order to enhance their resilience against factors that attack their behavioural wellbeing. To establish normal family life after a bloody conflict takes a lot of time and utilizes the return of family normalcy and familiar routines that engage the mental abilities of family members to understanding that life is gradually normalizing.
The challenges from emergencies, which result in traumas, therefore, will require special attention to be managed. According to Riefels (2013) the extension of post trauma services to the internally displaced persons has been recognized as an important step towards averting challenges of mental health towards victims of disasters. (North and Pfefferbaum, (2013); Norris, Friedman, & Watson, (2002); Bonanno, Brewin, Kaniasty, & LaGreca, (2010); Ritchie, Watson, & Friedman, (2006).) The Inter Agency Standing Committee (IASC) guidelines for psychosocial disaster responses recommend a multilevel support strategy to be utilized depending on the situation of the internally displaced population (Inter-Agency Standing Committee, 2007). The results of violence driven, and some natural disasters result into some trauma and the survivors are classified into five categories. (Cohen 2002). These are as follows:
To treat this survivors, psychosocial support professionals can use community-based intervention, rendering of direct assistance, and support such as Psychological First Aid. They can also apply other mental health treatments such as eye movement desensitization and reprocessing therapy, Or Eye Movement Desensitization and Reprocessing Therapy (EMDR); or pharmacotherapy or trauma-focused cognitive behavioural therapy, or TF-CBT; to avoid the development of further complex mental health conditions. Wietse et.al (2014) in their work also suggested a lot of preventive and treatment therapies being used in the psychosocial interventions at the individual, family and group levels. Among the methods include Huggy-puppy intervention, psychological first aid, trauma focused cognitive behaviour therapy, narrative exposure therapy, testimonial therapy, Dyad psychological support. They also listed group interpersonal psychotherapy and creative play, dance and movement therapy, mind body technique, skills and psychoeducation intervention, vocational training and psychosocial support intervention, readiness via group therapy plus education, teacher led trauma/ grief psychotherapy, and the nonformal education plus trauma healing etc. Umeda et.al (2020) in their study concluded that there is need for post disaster trauma patients need to be managed using psychosocial support and that the responders who are the third level survivors should also not be excluded from the services of these professionals. Wietse et.al (2014) in his review of over 160 reports on funding and implementation of psychosocial interventions in humanitarian settings from 2007 -2010 from around the globe listed the top five models being used in humanitarian setting as follows.
“In 160 reports, the five most commonly reported activities were basic counselling for individuals (39%); facilitation of community support of vulnerable individuals (23%); provision of child-friendly spaces (21%); support of community initiated social support (21%); and basic counselling for groups and families (20%).” p.1
Illagan (2018) in one of his several studies on Marawi Internally displaced persons and the provision of psychosocial support and emergency mental health posits that several organizations are positioned to render the service (about 25 of them) in the camps and that the IASC guideline was used as minimum standards and Tier 1-3 services were readily available but Tier 4 was rendered as an out-of-town service rendered from a hospital out of the camp local district by professionals. He also found that as the number of IDPs grew the services became less regular and almost non-existent. He concluded that MPHSS cluster was a challenge especially when the incident control system (ICS) for the intervention made it difficult for the cluster to fit in within the local council ICS.
Psychosocial and mental health support services in Nigeria’s humanitarian sector is managed by the MPHSS cluster which is headed by the World health organization (WHO). Other notable members of this cluster include the United Nations International Children’s Education Fund (UNICEF), Save the Children, International Organization for Migration (IOM), etc. The mental health and psychosocial support (MPHSS) cluster in Nigeria has been very active in both the health and protection sectors of the humanitarian platform in Nigeria. According to IOM (2019) it has provided 405,467 individuals with psychosocial services in Adamawa, Borno and Yobe states in the camps and host communities. It has also provided these services through 12 safe spaces, and 18 mobile teams. UNICEF in her 2021 appeal hopes to reach 218,000 children and caregivers who need access to mental health and psychosocial support. It has played an active role in the management of care for children and mothers who use the psychosocial services provided in the camps and host communities in the North east of Nigeria. (UNICEF 2019).
ICRC (2017) stated in her report that the organisation carried out over 100 sensitization sessions to raise awareness of mental health issues stemming from conflict and violence were organized with a total of 5,060 community members and 14 health staff in attendance and almost 5,510 displaced persons benefitted from International Committee of the Red Cross (ICRC)’s mental health and psychosocial support (MHPSS) program. 260 victims of violence received group counselling support while 60 hospitalized wounded patients benefited from individual counselling support. In all, 1,030 group and 90 individual MPHSS sessions were conducted in January to June 2017. While in ICRC (2019) it was able to sensitize over 6,200 persons on mental health care while 396 persons who experienced trauma in relation to the conflict received face to face consultations. 800 persons also attended group counselling sessions, all within the northeast.
According to Adesina, Olufadewa and Oladele (2020) in their work on the northeast, they listed the following organizations as playing key roles in the MPHSS sector in the country. Their study revealed that Centre for Community Health and development (CHAD), Save the Children and Street Child of Nigeria are the key players in the psychosocial support services for young children. The support for adults and youths is being spearheaded by IOM and NEEM Foundation. These organizations are operating in most of the camps in Maiduguri. The UNICEF is operating in two local governments of Bama and MMS. Médecins du Monde is involved in the management of individual and group counselling sessions and the IRC is involved in the provision of psychosocial services for mother and children in the Northeast, and all these are coordinated by the world health organization.
The MPHSS in other places where there are displaced persons resulting from herders / farmers conflict and other communal conflicts and natural disasters range from Benue, Katsina, Ebonyi, Kaduna, Cross River and Abuja Federal Capital Territory. It is apparent that this specialized intervention would always require the services of many organizations as no one organization would be able to take care of the entire service requirements and needs of the affected persons.
To ensure high standards and quality assurance for the delivery of these services, many organizations involved in the MPHSS have developed guidelines on how to manage a mental health or psychosocial intervention to ensure global best practices are upheld. To show how serious these procedures are, the IASC issued a worldwide guideline for the MPHSS cluster. According to IASC (2007) the “IASC guidelines for mental health and psychosocial support in emergency setting reflect the insights of numerous agencies and practitioners worldwide and provide valuable information to organizations and individuals on how to respond appropriately during humanitarian emergencies. The guideline provides specific action sheets which offer useful guidance on mental health and psychosocial support, and cover the following areas: coordination, assessment, Monitoring and Evaluation Protection and Human Rights standards Human Resources, community Mobilisation and support, Health services, Education, Dissemination of Information, Food security and Nutrition, shelter and site Planning, and Water and sanitation.” This document has been of great assistance to practitioners of MPHSS in the world. However, this has not stopped further improvements or guidelines from being introduced by other practising organizations. To be able to enhance the harmonisation of this practice in the field, many stakeholder organizations have gone ahead to develop their not so peculiar guidelines on the subject.
UNICEF (2015) developed operational guidelines for community – based mental health and psychological support in humanitarian setting using a three tiered system of support for children and families. These guidelines was specifically developed in response to children’s well-being, safety and optimal development and is generally aimed at;
Other stakeholders such as UNHCR, IOM, ICRC have all developed their own guidelines depending on their areas of concentration and core competence, while Save the Children has also adopted the guidelines of the UNICEF. (UNHCR 2015, IOM 2017, Save the children 2016).
The importance of this mental health service is very critical in disaster response, especially when it is a conflict driven emergency, where some of the affected persons witnessed the killing of their loved ones or the destruction of their properties or saw their loved ones defiled or themselves violated. This service acts as a catalyst for proper healing of the emotional and psychological wounds of the disaster. According to Goodwin, Leszcz et al (2001) on the study on the effect of group psychosocial support on metastatic breast cancer, the use of psychosocial intervention does not prolong the survival of affected persons, but, It improves mood and the perception of pain, particularly in women who are initially more distressed. Spiegel (1994) also posits that Psychosocial treatments, including group, individual, and family therapies, are of proven efficacy and deserve inclusion as standard components of biomedical treatment for patients with cancer. These goes a long way in showing the various forms of psychosocial interventions being used in and outside the camps. Wessells (2009) in his study of psychosocial support in international emergencies states that there is high need for psychosocial support on a large scale after international emergencies. However, the researcher posits that these tools are used in forms that cause further harm, and these are caused by issues such as security, humanitarian coordination, and inappropriate approaches and misplaced context and lack of knowledge of the background of the affected persons and that “these and related problems can be avoided by the use of critical self-reflection, greater specificity in ethical guidance, a stronger evidence base for intervention, and improved methods of preparing international humanitarian psychologists”.
Fenn(2018) in her work wondered if the psychological responders actually meet up the need for this services in any incident location as it was very intensive and demanding with the level of expertise it requires. She concluded that as critical incidents continue to increase in number and severity, there is need for professionals to come up with more appropriate ways to respond. A need is also there for more practitioners to sign up to go out there to render these services and be part of the humanitarian community. This also calls for the training and capacity building for responders since the services are of a continuing type and requires special skills. (Ras. 2007, Umeda et.al 2020) The review of over 260 literatures on psychosocial services brought this to the fore. Fleet and McCann (2007) also advocates the use of Filal therapy, Illagan(2018) proposes socio-therapeutic approach while Docena (2015) in his study concluded that the potential value of intervention is not only to nurture individual resilience but also enables community resilience. The use of these services and adopting the best practices is a sure way of achieving optimal performance.
Design and setting: This is a qualitative, descriptive, cross sectional study carried out in the IDP camps located in Maiduguri, Borno state.
Population, sample and sampling technique: The population of the study consists of the 45,019 internally displaced persons located in eight (8) camps in Maiduguri according to the displacement matrix of the Internal Organisation for Migration (IOM) and the National Emergency Management Agency (NEMA) namely Christian Association of Nigeria Centre, Arabic Teachers College, Teachers Village, NYSC Camp, Mogolis Camp, Bakasi Camp, Shehu Sanda Kyarimi Camp, and Goni Kachallari Camp. The sampling method was used to select 250 respondents, out of which 243 respondents finally participated.
Instrument: This study used interviews, questionnaires and focus group discussion as instruments used to elicit responses on the extent to which this service is being rendered to the affected persons.
Ethical Clearance: Ethical clearance was sought from both Borno state ministry of health, SEMA, the state’s focal organisation for emergency management and NEMA, The focal organisation for emergency management for Nigeria and coordinator of camp activities in Nigeria.
Research Questions
Three research questions were generated to guide this study.
Research question 1: What types of psychosocial support services are being used in the
various internally displaced persons camp in Maiduguri?
Research question 2: Which organizations are rendering these services in the camps?
Research Question 3: To what extent has these psychosocial services assisted in resolving the challenges of post disaster trauma in the various IDP camps?
Research questions 1 and 2 were answered using interviews and discussions in the camps with the respondents, while the third research question was answered using the questionnaire. The focal group discussion was used to elicit in depth responses that will aid the analysis and discussion of the findings.
Research question 1: What types of psychosocial support services are being used in the various internally displaced persons camp in Maiduguri?
The respondents identified the following services as present in the camps; Community support services 203 (83.54%), specialized services for at risk groups such as widows, orphans, injured and handicapped persons 198 (81.48%) etc. and direct support services for people with mental health issues 211 (86.84%). recreational activities for children and youth 199 (81.89%), informal education for adults 210 (86.42%), counselling and support groups 112 (46.09%). They also agreed that majority of the people fall under the “at risk groups” while the mental health issues are handled at referral levels.
The respondents also averred that many of the organisations in the camp have developed their own Mental Health and Psychosocial Support (MHPSS) activities, multidisciplinary psychosocial support mobile teams have been providing services to internally displaced persons (IDPs) and host community members, since 2014. According to IOM (2018) The teams composed of teachers, health care workers, counsellors and social workers offer a range of services including recreational activities for children and youth, informal education for adults, counselling and support groups. Through sensitization and focus group discussions, PSS teams are key in engaging with the local communities to identify and address cross cutting issues on gender based violence (GBV), security, protection, and various life stressors in the conflict environment.
Research question 2: Which organizations are rendering these services in the camps?
The majority of the respondents agreed on the presence of various activities in the camp and also that many of the camp dwellers that have mental or psychological issues have benefitted from these services. 213 (87.65%) respondents identified the presence of the International Office for Migration (IOM), in the camps and identified them with the psychosocial activities, 184 (75.7%) identified UNICEF with psychosocial activities in the camp especially as it concerned the children around schools in the camp. UNHCR was also identified by 86 (35.4%) respondents, IRC with 95 (39.1%) respondents while street for kids had 105 (43.21%) respondents identifying them as providers. 213 (87.65%) respondents identified ministry of health, NEMA, and BOSEMA as the organizations coordinating all these services. The respondents also identified some indigenous NGOs who are providing some level of activities relating to psychosocial activities in the camps, top amongst whom are NEEM Foundation, who were identified by 198 (81.5%) respondents, and also Médecins du Monde who are cognized by the 164 (67.5%) respondents are involved with both individual and group counselling. The respondents listed the names of organisations involved in rendering these services to include International Office for Migration (IOM), Nigerian Red Cross, International Committee for Red Cross (ICRC), NEMA & BOSEMA, UNICEF, UNHCR, FMWA and other NGOs in the camps. They explained that these organisations in course of their performing these roles have continued to improve as they understand the context better and as they also continue to receive both material assistance and capacity building from their various organizations.
Research Question 3: To what extent has these psychosocial services assisted in resolving the challenges of post disaster trauma in the various IDP camps?
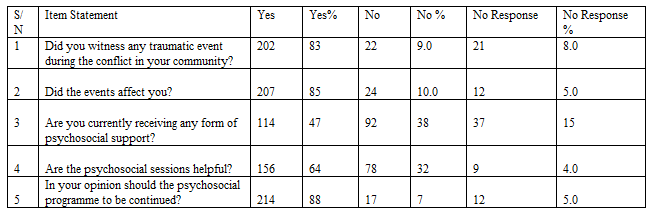
The third research question is analysed as follows with the aid of the tables above. The analysis presented on Table 2 showed that 202 respondents (83.%), 22
(9.0 %) and 21 (8.0 %) said Yes, No and No response respectively on item 1; 207 (85%); 24 (10.0%) and 12 (5.0 %) said Yes, No and No response respectively on item 2; 114(47%); 92 (38%) and 37(15%) said Yes, No and No response respectively on item 3; 156 (64%), 78 (32%) and 9 (4.0%) said Yes, No and No response respectively on item 4 and 214 (88%), 17 (7%) and 12 (5.0%) said Yes, No and No response respectively.
The focal group discussion revealed that the average time each of the respondents has stayed in a camp was 16 months with the least as 3 months. It also showed that more than 40% of the displaced persons have witnessed a death or torture of a close relative, except those who left early enough before the onset of the hostilities. Most of the IDPs still remember the ugly incidents and most of them agree that they have at one time or the other talked about the incident and about 60% of them agree that they have been treated for the trauma through counseling and other support techniques and are happy with the programme so far.
To strengthen the provision of MHPSS services, the organisations both local and international additionally support existing specialized mental health service facilities through the establishment of referral mechanisms, the rehabilitation of psychiatric wards, the training of mental health care workers and the deployment of psychiatric nurses into hard-to-reach areas. The project also offers integrated livelihood opportunities, as well as trainings on MHPSS interventions and MHPSS mainstreaming into the humanitarian response sectors and partners - including government, non-governmental actors, community leaders, United Nations agencies and civil society organizations.
Additionally, given the large scale protection concerns in the north east, they are ensuring protection mainstreaming throughout their emergency response and have rolled out GBV trainings for various sectors, conducting safety assessments, and working with partners to ensure GBV mainstreaming throughout the humanitarian response.
Psychosocial service is a prominent part of the maintenance and cares segment of the response phase of the disaster management cycle. It plays an important role especially in crisis driven disasters such as wars and insurgency. The post disaster traumas experienced by affected persons are the effects of punishment suffered by the individuals or their close relatives. It could also be as a result of experiences of other affected persons as observed by the individuals. It is therefore very important that these services be effectively rendered with the intention of promoting sense of safety and security, establishment of trust, strengthening of relationships, enhancing resilience and ensuring sustainability. It is also recommended that the responders should not be exempted from these services where necessary.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
